Article Text

Abstract
Objectives: This paper examines the prevalence of tobacco use among sexual minorities in the US through a systematic review of literature from 1987 to May 2007.
Methods: Seven databases were searched for peer-reviewed research (Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library via Wiley InterScience, Education Resources Information Center (ERIC), Health Source: Nursing/Academic, Institute for Scientific Information (ISI) Web of Science, PsycINFO via EBSCO Host and PubMed). No language restrictions were used. Abstracts were identified in the literature search (n = 734) and were independently read and coded for inclusion or exclusion by two reviewers. When agreement was not reached, a third reviewer acted as arbitrator. Abstracts were included if they presented data collected in the US from 1987 to May 2007 and reported prevalence or correlation of tobacco use with sexual minority status. Studies reporting data from HIV-positive samples were excluded. The identified articles (n = 46) were independently read by two reviewers who recorded key outcome measures, including prevalence and/or odds ratios of tobacco use, sample size and domain of sexuality (identity, behaviour, or desire). Factors relating to study design and methodology were used to assess study quality according to nine criteria.
Results: In the 42 included studies, 119 measures of tobacco prevalence or association were reported. The available evidence points to disparities in smoking among sexual minorities that are significantly higher than among the general population.
Conclusions: Ongoing, targeted interventions addressing smoking among sexual minorities are warranted in tobacco control programs.
Statistics from Altmetric.com
Tobacco use is a major contributor to morbidity and mortality in the US and throughout the world.1 2 The relative burden of tobacco-related disease will be affected by disparities in tobacco use among different socio-demographic groups. In the US, disparities in smoking prevalence have been demonstrated by age, educational attainment, race/ethnicity and gender.3
With respect to sexual minority populations (including individuals with gay, lesbian, bisexual and transgender identity, and individuals with same-sex relationships and/or attraction), past research has suggested that sexual minority status is associated with higher risk of smoking. In 2001, Ryan and colleagues4 conducted the first systematic review of smoking among sexual minority populations and identified 12 studies reporting smoking prevalence by sexual orientation. Although the review found some evidence for higher smoking prevalence among sexual minorities, the strength of its conclusions was limited by poor sampling methodology in the identified articles as well as variations in definitions of sexual orientation and smoking. A more recent but limited review of smoking among sexual minority women identified 16 studies and came to similar conclusions.5
This article updates previous reviews and reports findings from 42 studies, many with rigorous sampling designs, identified through a systematic search of the published literature from 1987 to May 2007. The identified studies answer our key question: what is the prevalence of tobacco use in sexual minority populations compared to the general population? Our review includes information on gender, sampling methodology, and the domain of sexuality used to determine sexual minority status. Domain of sexuality has been shown to influence the measurement of smoking prevalence,6 and can be divided into at least three categories: identity (gay, lesbian, queer, bisexual, etc.), behaviour (same-sex relationships, sexual contacts, partners, etc.) and attraction (same-sex desire, which may or may not be acted upon).7 The findings of the present review are relevant to the primary care of sexual minority populations; the design, implementation and evaluation of effective tobacco control policy (to ensure disparities are addressed and not exacerbated);8 9 and, the improvement of research and data collection.
METHODS
Data sources
Seven databases were searched for peer-reviewed research articles (Cumulative Index to Nursing and Allied Health Literature (CINAHL), Cochrane Library via Wiley InterScience, Education Resources Information Center (ERIC), Health Source: Nursing/Academic, Institute for Scientific Information (ISI) Web of Science, PsycINFO via EBSCO Host and PubMed) published between 1987 and May 2007. No language or geographic restrictions were used. Search terms (see Appendix) covered sexual minority status and tobacco use. No attempts were made to identify unpublished or non-peer reviewed studies.
Study selection
A total of 734 abstracts were identified in the initial literature search. These were read and coded for inclusion or exclusion by two independent reviewers (GKG, JGLL). When agreement could not be reached, a third reviewer acted as arbitrator (CLM). Abstracts were included if they presented data collected in the US from 1987 to May 2007 and reported prevalence or correlation of tobacco use with sexual minority status. Like Ryan and colleagues,4 we excluded studies reporting data from HIV-positive samples because of potential confounding between HIV status and tobacco use. Abstracts that were either unavailable or not published in English were excluded. In cases where the abstract did not provide sufficient information for exclusion, studies were included until the full text of the article could be evaluated. Excluded articles that were otherwise relevant to tobacco use among sexual minorities were coded as background. In cases where the same data and study questions were reported upon in multiple publications, the most complete work was retained. Four articles including previously published data sets were thus excluded.10–13 Additionally, three articles14–16 whose results were incorporated into the one identified meta-analysis17 were excluded as we determined the meta-analysis to be more informative than the inclusion of several smaller samples. Lastly, studies that reported on the National Longitudinal Survey of Adolescent Health (known as Add Health)18–20 and the 1995 Massachusetts and Vermont Youth Risk Behaviour Surveillance Surveys21–23 were all included because they analysed the data for different study questions.
Data extraction
A total of 46 studies were found to meet all inclusion criteria and were retained for further analysis (fig 1). Full-text versions of these studies were obtained and read by two independent reviewers (GKG, JGLL), who recorded key outcome measures, including prevalence and/or odds ratios of tobacco use, sample size and domain of sexuality (identity, behaviour, or attraction). When agreement was not reached, a third reviewer acted as arbitrator (CLM). Because of the wide variety of study designs and study populations, we did not combine data.
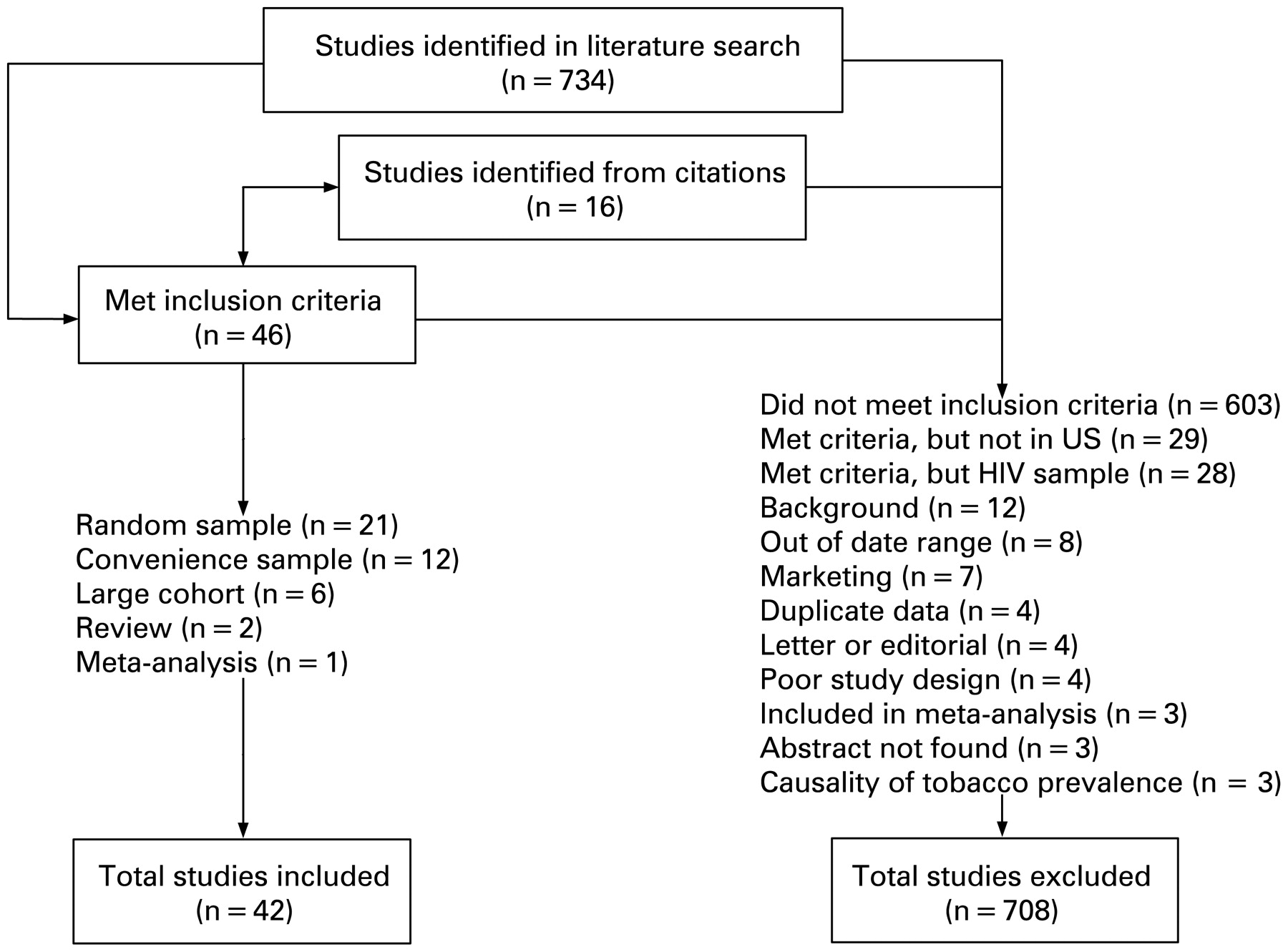
Summary of literature search and study identification.
Quality of studies
Study quality and design were assessed according to nine criteria: population-based (vs convenience) sampling, random sampling, equal risk at baseline between comparison groups, sampling not restricted to sexual minority populations, no stringent selection criteria (eg, having a family history of breast cancer or being the child of a nurse), bisexuality reported separately from exclusive homosexuality, similar ascertainment methods between comparison groups (using the same survey for the population of interest and the comparison group), statistical analysis for confounding variables (eg, age, education), and the ability to generalise the sample to the population of interest. Four studies meeting either none or just one of these criteria were classified as having a poor quality study design and were excluded from further analysis.24–27 One exception was a study28 that was retained despite poor study quality because it reported on smoking prevalence by race and ethnicity among sexual minorities (for which there are very limited data). A total of 42 studies were retained for final analysis.
RESULTS
In all, 21 studies used population-based sampling,6 21–23 29–45 6 were from large cohorts,18–20 46–48 1 was a meta-analysis,17 and the remaining 12 were convenience samples.28 49–59 Results of the two previous reviews are not reported here.4 5
Studies defined tobacco use in nine different ways or failed to report a definition. In most studies, tobacco use was defined as smoking in the past month, current smoking, or smoking in the past month with over 100 cigarettes consumed over the course of the respondent’s lifetime (table 1).
The 42 included studies reported 119 measures of tobacco prevalence or association. Most measures reported the prevalence of smoking or smokeless tobacco use among a sexual minority population (n = 97). Of these, 88 reported prevalence in a comparison population. Some (n = 59) reported an odds ratio (OR) or risk ratio (RR), but only 37 reported the corresponding 95% confidence intervals (CIs). Very few (n = 12) reported other measures of association. One reported only non-significance. A total of 43 measures were reported for men, 67 for women and 9 (reported in the Appendix) aggregated gender. Two reported on smokeless tobacco use and the remainder reported on cigarette smoking. Table 2 illustrates the number of measures for men and women by domain of sexuality.
Among studies reporting ORs and 95% CIs, ORs for sexual minority tobacco use ranged from 0.9 to 6.3 in comparison to heterosexual populations. Figure 2 graphs the ORs that were reported with 95% confidence intervals by gender, stratifying by homosexuality, bisexuality and the aggregation thereof. Each category may include multiple domains of sexuality: behaviour, attraction and/or identity. Studies generally showed a positive association between sexual minority status and cigarette use with ORs between 1.5 and 2.5.

{kind=link}
{kind=link}
Odds ratios and 95% confidence intervals (CIs) of cigarette smoking among sexual minority men and women.
Smoking among sexual minority women
The 2006 National Health Interview Survey reported the national estimate of smoking among women in the US to be 18%.3 For women who reported exclusively homosexual identity, behaviour, or attraction, ORs ranged from 0.6 (exclusively same-sex behaviour) to 4.9 (exclusively lesbian identity) (table 3 (online only)) both in a single random sample of college students at one Midwestern university.6 All other ORs, however, fell between 1.2 and 2.0. Prevalence of smoking, which is complicated by the use of different definitions of smoking, was lowest (7% to 10%) among women participating in biomedical studies, among older women, and in a California convenience sample. Among adolescents, there was no statistically significant difference in smoking prevalence reported in two studies using data from Add Health.18 19 The prevalence in the four randomly sampled, non-college studies ranged from 25% to 37%. All randomly sampled, non-college studies were from California.
Among women with bisexual identity, behaviour, or attraction, ORs ranged from 1.5 among women reporting past female partners but a current male partner in the California Women’s Health Survey30 to 3.5 in the National Alcohol Survey33 (table 3 (online only)). There was a notable and statistically significant risk for adolescent women in Add Health and Growing Up Today (a cohort of children of nurses enrolled in the Nurses’ Health Study II) that was not seen for adolescent women reporting exclusive homosexuality in Add Health (exclusive homosexuality was not analysed in Growing Up Today).18 19 46 In the five randomly sampled non-college studies, prevalence ranged from 27% to 50%. All but one were from California.
When bisexual and homosexual identity, behaviour and attraction are aggregated, the risk of smoking was also elevated. Most alarmingly, the odds of smoking among lesbian and bisexual adolescents in Growing Up Today, were 6.3 (95% CI 3.4 to 11.6) times greater than for their straight counterparts.46 Only one study was randomly sampled outside of a university campus: the California Women’s Health Survey reported a 1.8 OR (95% CI 1.5 to 2.3) of current smoking for any women with one or more same-sex partner compared to women with only opposite-sex partners.30
Among studies reporting on the association of smoking with female sexual minorities, all random samples outside of college students were conducted in California, except for a small sample from the National Alcohol Survey. With the exception of women in California reporting “other race”, when compared to a Latina reference group, all randomly sampled, non-college-based studies that reported an OR and CI showed a statistically significant association between female sexual minority status and cigarette smoking, ranging from 1.5 to 3.5. Of these, all ORs but one fell between 1.5 and 2.1.
Smoking among sexual minority men
The 2006 National Health Interview Survey reported the national estimate of smoking among men in the US to be 24%.3 For men who reported exclusively homosexual identity, behaviour, or attraction, ORs ranged from 1.1 in a national random sample of college students34 to 2.4 in a random sample of a northern California healthcare plan37 (table 4 (online only)). Only two studies were randomly sampled outside of college campuses. The previously mentioned California healthcare plan and the California Health Interview Survey45 both found the odds of smoking to be over twice as great as for heterosexual men (significant at OR 2.4 and 2.1, respectively). As among sexual minority adolescent women, exclusive homosexuality was generally associated with decreased likelihood of smoking in Add Health.18 19 The prevalence in randomly sampled, non-college studies ranged from 24% to 33%.
Among men with bisexual identity, behaviour, or attraction, ORs ranged from 0.9 for bisexual men in the California Health Interview Survey45 to 2.6 for “mostly heterosexual” men in a random sample at a Midwestern university.6 As with sexual minority adolescent women, bisexuality was generally associated with increased risk of cigarette smoking in Add Health and Growing Up Today for men.18 19 46
When bisexual and homosexual identity, behaviour and attraction were aggregated, one large random sample in Tucson, Arizona and Portland, Oregon, found an elevated prevalence of smoking among white gay or bisexual men (42% vs 29% for heterosexual men) but not among American Indian/Native American men and Asian/Pacific Islander men.44 Youth Risk Behaviour Surveillance Surveys in Massachusetts and Vermont found elevated risk for sexual minority male students.22 23
As with studies of female sexual minorities, most randomly sampled studies were conducted on college campuses or in California. The two randomly sampled, non-college studies including ORs reported significant results (OR 2.1 95% CI 1.7 to 2.7 and OR 2.4 95% CI 1.8 to 3.3) for smoking among gay men.37 45 The data for bisexual men are equivocal with non-significant findings in all samples except for adolescent men with bisexual behaviour, attraction and/or identity who were at elevated risk.18 19 46
Studies on sexual minority identity and race/ethnicity
When stratified by race and ethnicity, three studies reported on sexual minority men40 44 45 and four on sexual minority women.28 40 45 58 One additional study reports on measures combining men and women and is reported in the Appendix.20 Only Stall and colleagues sampled randomly, using a random sample from Tucson, Arizona and Portland, Oregon phone books. Black gay or bisexual men had almost double the smoking prevalence of heterosexual black men (62% vs 34%). Hispanic, Asian and American Indian men had relatively similar smoking prevalence to heterosexual counterparts.44
Families, caregivers and couples
In 7 years of data from the National Health Interview Survey, Heck and Jacobson reported that 29% of women and 31% of men in a same-sex partnered household currently smoke compared to 19% and 23% of women and men, respectively, in opposite-sex partnered households.39 The National Health Interview Survey provides the best national data available, albeit including only partnered individuals.
Little is known about smoking in gay and lesbian families. Sanchez and colleagues reported on the percentage of Hispanic (78%) and African–American (58%) lesbian or bisexual smokers who care for their own children or the children of a partner in a largely dance-club-based convenience sample in the Bronx, New York.58 We identified no other studies reporting on smoking and sexual minority families, parents, or caregivers.
DISCUSSION
This review provides strong evidence for the existence of an elevated prevalence of smoking among sexual minorities with odds ratios between 1.5 and 2.5 when comparing against heterosexual counterparts. Among sexual minority women, odds ratios were between 1.5 and 2.0 when comparing against heterosexual women. Among sexual minority men, odds ratios are generally between 2.0 and 2.5 when comparing against heterosexual men. Evidence for adult bisexual men, however, was inconclusive. Limited evidence suggests that bisexual adolescents are at higher risk than their exclusively homosexual peers. A rigorously sampled study in California, which fell outside of our date range, confirms these findings and suggests that prevalence among sexual minority women may be even higher than our estimates.60
The aetiology of these tobacco use disparities can be understood within the social/ecological model articulated by Bronfenbrenner,61 wherein differences in health status are based in the dominant social, economic and political environment and generated at multiple levels: interpersonal, family, community and society. With respect to sexual minority populations, sexual orientation is thus conceptualised not as the cause of tobacco disparities but as a marker of health risk caused by interactions with the social/ecological environment. Using the Bronfenbrenner model, we can begin to conceptualise how sexual minority status could be a marker of tobacco initiation risk and also have a protective effect—depending on the particular interaction between identity, development,62 and the socio-political environment.
Analyses of Add Health data found greatly reduced risk for adolescents who had only same-sex relationships versus those adolescents with same-sex and opposite-sex relationships.18 19 Add Health data could reflect adolescent experiences with difficult stages of identity development or extra stress associated with bisexual identity, but no measures of either were reported. Adolescents identifying as “mostly heterosexual” in Growing Up Today study were also at significantly higher risk of smoking than their “fully” heterosexual peers, but Growing Up Today analyses aggregated bisexual and gay identity,46 and thus cannot confirm the Add Health finding. Many models of identity development for sexual minorities exist, but few have been rigorously tested across sexual minority populations.63 We identified no studies that reported tobacco use by stage of identity development. Because of the aggregation of bisexual behaviour, identity and attraction in all other studies that focus on adolescents, the Add Health finding cannot be verified. The same protection found in Add Health is also evident in some studies of college-age adolescents,6 34 but is not evident among adults. (That exclusively same-sex relationships are protective should not be misconstrued to label bisexuality a risk factor. The aggregation of bisexuality and different stages of identity development could be a driving force in this finding.) It is possible that adolescents age out of the protective effects of sexual minority identity as social and physical environments change. Further research should emphasise the importance of resiliency, protective effects of identity and “within-group” differences in risk.62
Efforts to address disparities in smoking require a better understanding of the aetiology of smoking among sexual minorities. Although a thorough discussion of this subject is outside the scope of this paper, several articles identified suggested possible causal pathways for the creation of tobacco disparities among sexual minorities.64–67 Identified pathways included the linkage between gay and lesbian social spaces (such as bars) with smoking,68 initiation of smoking due to violence, stress and discrimination,69 as well as barriers to healthcare access and treatment services. Targeted marketing by the tobacco industry, which has gone so far as to link “smokers’ rights” with rights for marriage equality,70 is also a likely contributing factor.71–76 Further research into these areas is justified to guide the development of effective interventions.
Race and ethnicity
Addressing disparities also requires a better understanding of the impact of race and ethnicity on tobacco use among sexual minorities. Race and ethnicity, like sexual minority status, do not have an intrinsic link to tobacco, substance abuse, or other risk behaviours.77 However, disparities in smoking among racial and ethnic groups within the US do exist,3 and there is reason to believe that they are determined by the different social, economic, environmental and political contexts of racial and ethnic minorities. How, when and for whom race, ethnicity and sexual minority status combine detrimentally and/or protectively remains a question.78 79
Limitations
Some variability in smoking prevalence was seen across the 42 identified studies. In convenience samples taken at bars and clubs, over-estimates of prevalence are likely given the selection bias inherent in bar samples. As this review relied solely upon studies in the published literature, there is the potential for bias against unpublished studies that showed a null result. Additionally, although some studies stratified results by age, the present review only included the aggregated measure across all ages. Tobacco use among young people, in particular, may appear attenuated given the evidence that young people are more likely to smoke than adults.3 While the findings of this review could offer some insight into tobacco use among sexual minorities throughout the world, further research is warranted to determine its relevance to contexts outside of the US, particularly as the tobacco industry shifts its focus to low-income countries in the “Global South”.
As noted in previous systematic reviews of smoking,80 a major limitation was the lack of standardised definitions of smoking. Smoking was defined in ways as different as having smoked more than six cigarettes during one’s lifetime57 and more than two cigarettes per day.51 The operationalisation of sexual minority status also frustrates attempts to compare across studies. Previous research has documented widespread inconsistencies in how researchers conceptualise and use sexual orientation.81–83 First, measurement of sexual minority status by different domains of sexuality complicates comparisons. Second, research conducted within one domain of sexuality (eg, attraction) may not be applicable for programs targeted by another domain (eg, identity). Third, our understanding of causal pathways for tobacco initiation may be affected by how sexual orientation is defined.
When reporting on tobacco use by race and/or ethnicity, some studies used a comparison group of heterosexual men or women from the same racial/ethnic group, while others compared racial and ethnic groups within the sexual minority sample using either Latino45 or white20 populations for comparison.
What this paper adds
-
There is compelling evidence that an elevated prevalence of tobacco use among lesbian, gay and bisexual men and women exists.
-
National and state surveillance systems should incorporate sexual minority status to monitor the elevated use of tobacco by gays and lesbians.
Six significant gaps in the published research were identified. First, there were no data on smoking among transgender populations. Second, there were no evaluations of smoking prevention or cessation interventions in sexual minority populations. Third, data on race and ethnicity remains sparse, particularly from population-based samples. Fourth, there is only one study on adolescent tobacco use that does not aggregate bisexuality. Fifth, only two measures of smokeless tobacco use were identified, although a recent study outside the date range of our search reports a lower prevalence of smokeless tobacco use among sexual minorities in California.84 Sixth, there is little to no evidence about the prevalence of tobacco use among sexual minority families, particularly families with children.
This last gap is of increasing importance as more sexual minority couples start families and parent children, and as legal protections with respect to marriage rights and civil unions evolve.85 Preconceptional health for lesbians may not be considered a high priority by health care professionals,86 and it could be beneficial to begin emphasising tobacco prevention and cessation as lesbians start families and initiate pregnancy. In this regard, future research could investigate smoking prevalence among pregnant sexual minority women, among partnered sexual minority men and women, or among those parenting or planning to parent children.
Conclusions
Increased attention to smoking among sexual minority populations is warranted in clinical practice and in the creation of prevention and treatment programs. In examining the ample evidence of disparities in suicidal ideation among sexual minority adolescents, Morrison and L’Heureux noted that the “[p]revention of GLBQ [gay, lesbian, bisexual, and queer] adolescent suicide thus could entail treating the environments that interface with GLBQ youth in addition to treating the adolescents themselves”.87 The same may well be true for elevated prevalence of smoking among sexual minorities. Moreover, there are specific evidence-based steps that can be taken to reduce the impact of smoking on sexual minority communities.
Prevalence could be assessed and monitored through Youth Risk Behaviour Surveillance Surveys, Youth Tobacco Surveys, Behavioural Risk Factor Surveillance Surveys and Adult Tobacco Surveys. Many states, however, do not include sexual orientation, thus hindering monitoring efforts despite the fact that sampling methodology has been crucial in researchers’ understanding of gay and lesbian health and well-being.88 Population-based interventions such as increasing taxes on tobacco products and banning advertising should be combined with approaches that seek to reduce disparities in vulnerable populations.9 These might include social marketing efforts, mass media campaigns in the gay and lesbian press, community recognition of tobacco as a problem,89 90 extra efforts for smoke-free gay and lesbian venues, targeted cessation services,91 community rejection of tobacco industry sponsorship of events and ongoing collaboration with the National LGBT Tobacco Control Network (http://www.lgbttobacco.org/). Given the leitmotiv of smoking as a health inequality in sexual minorities’ lives, local, state and federal tobacco programs should target lesbian, gay, bisexual, transgender (LGBT) populations in tobacco prevention and cessation interventions and include priority population indicators in the evaluation of program outcomes.
APPENDIX
Acknowledgments
Special thanks to Mellanye Lackey and the UNC Health Sciences Library family for excellent support throughout the research process and to Anna Freeman, Anna McCullough and our very helpful reviewers for constructive feedback on the text.
Search strategy
Search terms covered sexual minority status (homosexuality OR homosexual OR gay OR “sexual minority” OR “female homosexuality” OR “homosexuality, female” OR lesbian OR bisexuality OR bisexual OR transgender OR transsexual OR transsexualism OR transsexuality OR MSM OR queer OR “sexual orientation” OR “men who have sex with men” OR WSW OR “women loving women” OR “women who have sex with women” OR lesbianism) and tobacco use (tobacco OR smoking OR smoker OR smokeless OR lobeline OR cotinine OR cigarette OR cigar OR habits OR habit OR “addictive behavior” OR addiction OR nicotine OR prevalence OR epidemiology). Truncations were not used because of incompatibilities with some databases. Searching was conducted from 26 to 27 May, 2007.
REFERENCES
Footnotes
-
Funding: This work was partially supported by The Robert Wood Johnson Foundation’s Smoke-Free Families National Dissemination Office (grant no. 053311). The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the views of the Robert Wood Johnson Foundation.
-
Competing interests: None.