Article Text

Abstract
Objective We sought to conduct a systematic review and meta-analysis of evidence to inform policies that reduce density and proximity of tobacco retailers.
Data sources Ten databases were searched on 16 October 2020: MEDLINE via PubMed, PsycINFO, Global Health, LILACS, Embase, ABI/Inform, CINAHL, Business Source Complete, Web of Science and Scopus, plus grey literature searches using Google and the RAND Publication Database.
Study selection Included studies used inferential statistics about adult participants to examine associations between tobacco retailer density/proximity and tobacco use behaviours and health outcomes. Of 7373 studies reviewed by independent coders, 37 (0.5%) met inclusion criteria.
Data extraction Effect sizes were converted to a relative risk reduction (RRR) metric, indicating the presumed reduction in tobacco use outcomes based on reducing tobacco retailer density and decreasing proximity.
Data synthesis We conducted a random effects meta-analysis and examined heterogeneity across 27 studies through subgroup analyses and meta-regression. Tobacco retailer density (RRR=2.55, 95% CI 1.91 to 3.19, k=155) and proximity (RRR=2.38, 95% CI 1.39 to 3.37, k=100) were associated with tobacco use behaviours. Pooled results including both density and proximity found an estimated 2.48% reduction in risk of tobacco use from reductions in tobacco retailer density and proximity (RRR=2.48, 95% CI 1.95 to 3.02, k=255). Results for health outcomes came from just two studies and were not significant. Considerable heterogeneity existed.
Conclusions Across studies, lower levels of tobacco retailer density and decreased proximity are associated with lower tobacco use. Reducing tobacco supply by limiting retailer density and proximity may lead to reductions in tobacco use. Policy evaluations are needed.
- prevention
- public policy
- advertising and promotion
Data availability statement
Data are publicly available in the East Carolina University dataverse, https://doi.org/10.15139/S3/6175L7.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Novel strategies focused on reducing the supply of tobacco products are recommended to help achieve the tobacco endgame and promote health equity.1 2 Governments around the globe are increasingly regulating3 4 the retail supply of tobacco by: (1) limiting the sales of tobacco products near youth-serving locations such as schools,5 (2) limiting the total number of locations selling tobacco products in a given area6 and (3) limiting the types of stores (eg, pharmacies) that can sell tobacco products.7 While not all of these policy options are possible in any given jurisdiction, the burgeoning interest in tobacco supply reduction highlights the need for a robust understanding of the evidence underlying these policy efforts to reduce tobacco retailer density and decrease proximity.
Both tobacco retailer density and proximity are hypothesised to influence behaviour8–10 and thus, ultimately, health. This influence is thought to operate through reduced travel costs,11 increasing exposure to cues to purchase and, in some jurisdictions, increased exposure to marketing when there are more tobacco retailers.12 Retailer density and proximity may also influence social norms around smoking.13 However, prior reviews provide inconsistent evidence for these hypotheses. One meta-analysis focused on youth14 and four systematic reviews examined the association between density and proximity and youth15–17 and adult18 tobacco use. In a 2014 review, Gwon et al reported on nine studies about adolescent smoking behaviours, finding a pattern of positive associations between retailer density, retailer proximity and lifetime and past-year smoking, with less evidence regarding smoking susceptibility and past-month smoking.17 In a 2017 systematic review, Nuyts et al identified 20 studies, reporting inconsistent evidence for a positive association of density and proximity with adolescent smoking. Notably, this review identified ‘fundamental challenges in study design and exposure measurement’ hindering the interpretation of findings (p. 239).16 In a 2017 meta-analysis of 11 studies, Finan et al reported a significant positive relationship between density around participant homes (but not schools) and past-month smoking.14 In a 2019 systematic review, Marsh et al identified 35 studies regarding youth, finding evidence of an association between density and smoking but not of the relationship between retailer proximity and smoking.15 In a 2019 systematic review that included 40 studies of youth and adults, Valiente et al found a pattern of positive associations of density with smoking and initiation, and a negative association with cessation. However, proximity measures were only associated with cessation.18
To date, there has been no meta-analysis of studies about density/proximity and adult tobacco use behaviours. Additionally, the literature examining tobacco retailer density/proximity in relation to health outcomes, such as hospital admissions and birth outcomes, is sparse19–21 and warrants greater attention. Other gaps in the literature are questions about the underlying methodology and measures of tobacco retailer density and proximity.16 18 To fill these gaps, this systematic review and meta-analysis examines the relationships between tobacco retailer density/proximity and adult tobacco use behaviours as well as health outcomes.
Methods
Search
Following best practices, a professional health sciences librarian (KBS) iteratively developed the search strategy (see Footnote1), translated it between databases and implemented the search.22 We limited our search to records published in 2000 or after, corresponding to the initiation of this literature in 2002.23 The search was implemented in 10 databases: MEDLINE via PubMed, PsycINFO, Global Health, LILACS, Embase, ABI/Inform, CINAHL, Business Source Complete, Web of Science and Scopus. The search was last updated on 16 October 2020. We also reviewed supplemental tables from a systematic review that included studies of adults.18
To assess the grey literature, we conducted backwards searching of systematic reviews and conducted a search of the New York Academy Medicine Grey Literature database, Google Custom Search for non-governmental organisation publications, Dissertations and Theses through ProQuest and the RAND Publication Database. We deduplicated references in EndNote and then loaded references into Covidence software (covidence.org) for screening.
Eligibility
As defined in our registered protocol, PROSPERO #CRD42019124984, which is available from East Carolina University Dataverse, https://doi.org/10.15139/S3/6175L7, we sought to include peer-reviewed or grey literature with the following characteristics: records that (a) use inferential statistics with (b) individual-level data to examine an association between (c) tobacco retailer density or proximity and (d) tobacco use (initiation, use, cessation, quit attempts, health outcomes) for (e) adults in (f) an Organization for Economic Cooperation and Development (OECD) member country. Ecological studies of area-level behaviours were not eligible. We defined tobacco retailers as stationary retail locations that sell tobacco and excluded studies focused on retailers that only sell vaping products, as this literature is emerging and may have different relationships with the outcomes of interest.
Inclusion coding
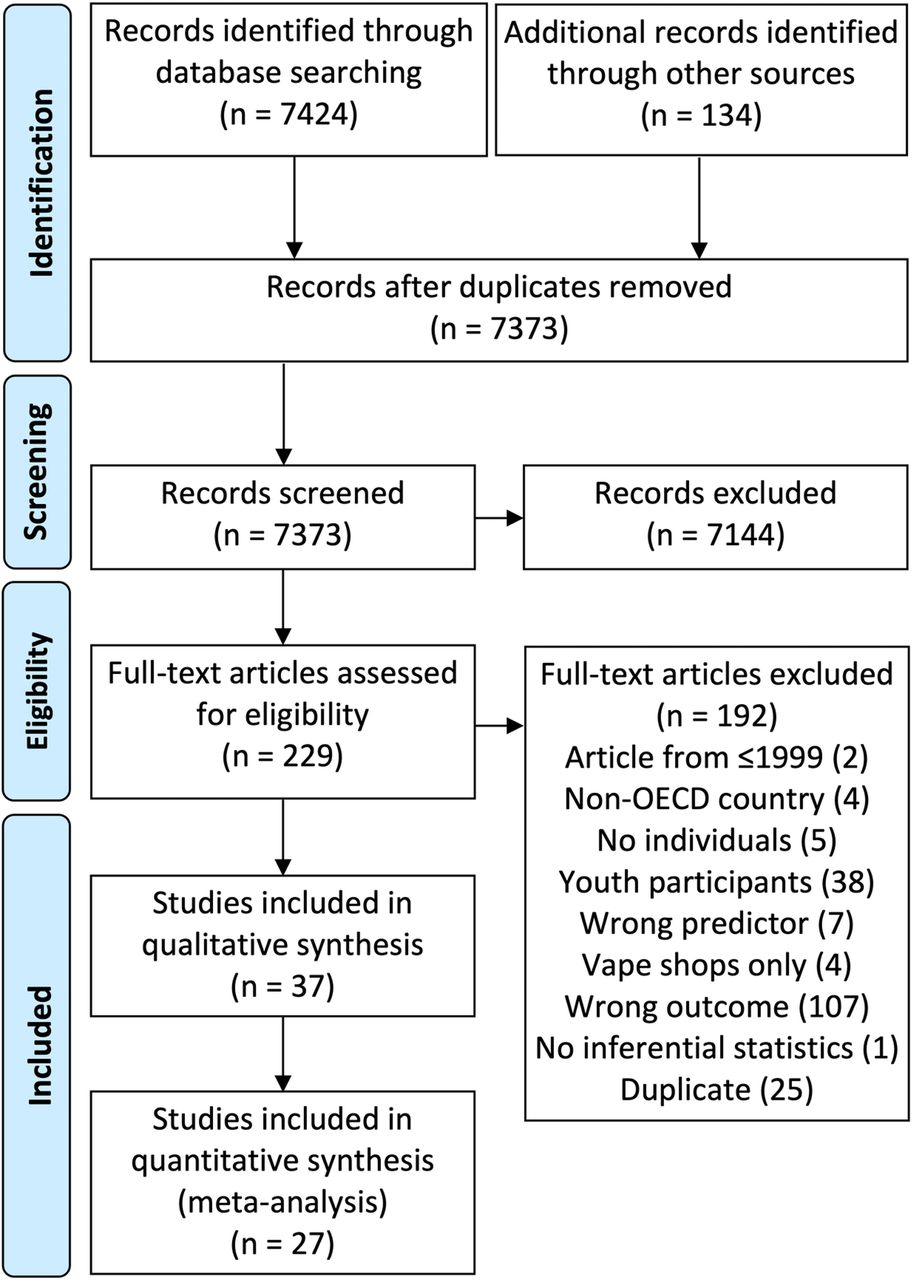
First, each record’s title and abstract were reviewed by two independent coders for inclusion. Second, each record identified as eligible in the title and abstract screening had its full-text reviewed by two independent coders. At both stages, disagreements were resolved by consensus. Figure 1 shows the flow diagram.

Flow diagram of study coding and inclusion. OECD, Organization for Economic Cooperation and Development.
Data abstraction
Data abstraction was conducted by one author (JGLL) and confirmed by a second (AYK). Data abstraction included design, study area, area units used, use of activity space (ie, calculating the area unit based on participant movements), statistical approach, sample size, variable definitions, prevalence of the outcome for the reference group and effect sizes. Based on the included records, effect size measures for behavioural effect sizes included initiation; smoking; quitting; relapse and psychological constructs directly related to quitting, such as smoking urges, pro-cessation attitudes and self-efficacy. Effect size measures for health outcomes included hospital admissions, overall survival among cancer patients and pregnancy outcomes such as low birth weight. We excluded effects that simultaneously controlled for multiple measures of density (eg, measures of proximity that held the count of stores constant).
Based on country and year(s) of data collection, we coded each included effect size in the context of two policies: (1) a policy that prohibits retail advertising and (2) a policy that restricts retail displays of tobacco products. We coded policies based on reports from the International Tobacco Control Project,24 Campaign for Tobacco-Free Kids Country Profiles25 and published reports.26 27 The coding considered policies in Canada and Australia at the subnational level. In the event that a policy changed during data collection, we coded whichever policy covered the greater proportion of data collection.
Study risk of bias assessment
To assess risk of bias in studies, we used a modified Downs and Black checklist,28 creating a risk of bias index (0–7, with greater numbers indicating higher risk). We planned to exclude studies with a score of four or higher of bias a priori; however, the mean score was 0.49 (range 0–2). Thus, no studies were excluded based on risk of bias. Additionally, we examined records for evidence of being published in likely predatory journals, which is an emerging best practice in systematic reviews.29 We did not exclude any records based on coding for predatory journals. See online repository protocol file for details of both risk of bias assessments.
Meta-analysis
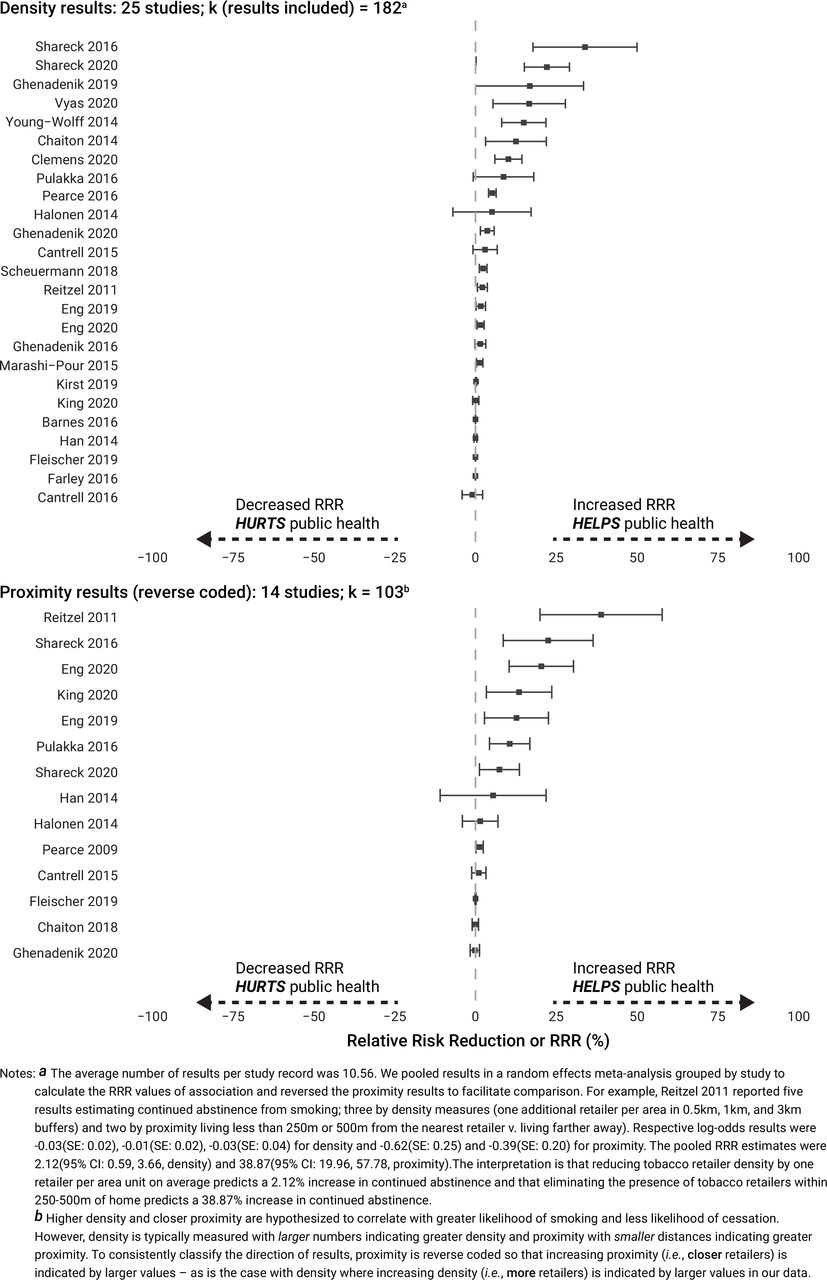
We first converted results into a relative risk reduction (RRR) using methods proposed by Mirzazadeh et al 30 including a correction proposed by Zhang and Yu.31 This effect size is recommended for translational research and can be computed from results of various statistical analyses.30 A Dictionary of Epidemiology explains the RRR as, ‘[t]he amount by which a person’s risk of diseases is reduced by elimination or control of an exposure to risk’.32 The RRR is the per cent reduction in the outcome expected from the reduction in exposure measured in any given analysis. However, the exact interpretation of the RRR is based on how the outcomes and exposures were operationalised and analysed in the reviewed studies. For example, outcomes could be measured as the likelihood of being a current smoker, the likelihood of quitting or the likelihood of relapse. Tobacco retailer density reduction could be analysed as one fewer retailer per thousand population or as the difference between being in the highest vs lowest quartile of exposure. In this meta-analysis, a positive RRR indicates a relative reduction in risk corresponding to an average tobacco-related outcome from an average reduction in exposure to density or decrease in proximity across the studies. For example, a RRR of 4.92 indicates we would expect an approximately 5% reduction in tobacco use using an average study’s measures of tobacco use as a result of a reduction of density or proximity using an average study’s measure of density or proximity. In the included studies, density is typically measured with larger numbers indicating greater density, and proximity is typically measured with smaller distances indicating greater proximity. To consistently classify the direction of results, proximity was reverse coded so that increasing proximity (ie, closer retailers) is indicated by larger values—as is the case with density where increasing density (ie, more retailers) is indicated by larger values in our data.
Meta-analysis techniques for synthesising the results of multiple studies were originally developed for testing the results of interventions.33 Observational studies present challenges in that they represent different methodological approaches and study characteristics.34 For example, the included literature addresses different outcomes (eg, initiating, quitting and disease outcomes such as hospitalisations and birth outcomes); measures predictor variables in different ways; uses different study designs; controls for covariates in different ways at one, both or neither of individual and neighborhood-levels. The observational studies included in this review do not typically report a ‘main effect’. Instead, many report results from sensitivity analyes (eg, results when density is calculated within 500 m vs 250 m of a participant’s home).
These sources of heterogeneity in the literature have been identified as a challenge to the interpretation of existing evidence about tobacco retailer density and proximity.16 Heterogeneity is often thought of as a noise or nuisance in meta-analysis; however, it can also help with understanding patterns of results across different study characteristics and populations. For example, studies conducted in different policy environments may have greater or lesser exposure to pro-smoking cues at the point of sale. Following guidance from the Cochrane Handbook on addressing heterogeneity,35 we addressed this challenge in four ways.
First, we used a random effects meta-analysis framework and calculated I2 heterogeneity statistics36 to indicate the percentage of variability in the estimate due to heterogeneity in studies rather than chance from sampling.37 Following the assumptions of random effects meta-analysis, we also calculated a prediction interval (ie, the interval in which 95% of the future values are estimated to be) and an opposite effects proportion (ie, the proportion of the population for whom the effect will be in the opposite direction). While the opposite effects proportion was hypothesised to be low, it represents an important consideration in the presence of heterogeneity.
Second, we reported the estimated proportion of effect sizes that are meaningful at the population level,38 which we defined as a 1% or larger reduction in the measured outcome (eg, smoking). We selected this cut-off given overwhelming evidence of the harms of tobacco use and that even small declines at the individual level have meaningful population effects.39
Third, we then conducted separate meta-analyses for each study characteristic to assess the consistency of our findings across diverse studies. Each analysis was conducted using a subpopulation command to better estimate standard errors. We did not further adjust for multiple comparisons following the logic of Rothman.40
Fourth, we examined the role of different study and measurement characteristics on the magnitude and direction of effect sizes in a meta-regression framework. While separate meta-analyses can tell us how the association between retailer density/proximity and the risk reduction in tobacco use and related disease differ by each study characteristic, they can be confounded by other study characteristics. Results from an adjusted meta-regression controlling for all assessed study characteristics can help further disentangle which specific study characteristics, settings or specific populations may be associated with this reduction. That is, we regressed study characteristics on effect size estimates to identify whether study characteristics were associated with a change in effect size while controlling for all other study characteristics. With an intra-class correlation of 0.17 across our effect sizes, we used multilevel modelling for our meta-regression to address dependence in the data from having multiple effects nested within studies.
We pooled the results of each study by use of density or proximity predictor variables and present these results in a forest plot. To assess for publication bias, which is the propensity of researchers to publish findings reaching historical thresholds of statistical significance more frequently than findings not reaching such thresholds, we examined a funnel plot to assess for asymmetry.41 The presence of publication bias can indicate that an effect size is overestimated given the absence of null findings.41
We used SPSS V.27/Macintosh for data management and conducted the meta-analysis in Stata IC V.16/Macintosh. Files are available from the East Carolina University Dataverse, accession doi:10.15139/S3/6175L7, at https://doi.org/10.15139/S3/6175L7.
Results
Meta-analysis
As shown in table 1, we identified 37 records from 8 countries: Australia,19 42 Canada,20 43–52 Denmark,53 England,54 Finland,55–57 New Zealand,58 Scotland59–61 and the USA.21 62–77 We constructed an evidence table (see online repository files). Over one-third of the records (n=14) leveraged longitudinal data from Canada,20 44 45 49–51 Finland,55–57 New Zealand,58 the UK54 59 and the USA.68 70
Included records, n=37, characteristics, effect sizes identified (n effects), effects included in meta-analysis (k) and risk of bias (RoB) index score
From the 37 records, we abstracted 349 results (see online repository files). From these, we identified 285 results with sufficient information to calculate an effect size for the meta-analysis. Effect sizes were derived from 27 records (average number per study: 10.56, range: 1–38). Ten records were excluded from the meta-analysis because we could not calculate effect sizes from available information for a linear outcome variable,21 70 72 74 studies reported results for just one type of tobacco retailer (eg, alcohol stores that sold tobacco),62 the analysis was a conference presentation that was later published,56 60 or publications did not provide enough details to calculate an effect size.53 67 73
Figure 2 shows a forest plot of pooled results by study and by use of density or proximity. A funnel plot presented in the online repository files shows visual evidence of asymmetry, indicating the likely presence of publication bias.

{kind=link}
{kind=link}
Forest plot of pooled study (n=27) results (k=285) by use of density and proximity showing estimated relative risk reduction (RRR) expected from reduced exposure to tobacco retailers. RRR, relative risk reduction.
We calculated effect sizes for behavioural (k=255) and disease (k=30) outcomes. The meta-analysis of all behavioural effect sizes (k=255 from n=26 studies) indicated a statistically significant relative risk reduction of 2.48 (95% CI 1.95 to 3.02). This indicates that based on all included studies, there is an estimated 2.48% reduction in risk of tobacco use with reduced exposure to tobacco retailer density and proximity. However, consistent with substantial methodological diversity across studies, we identified considerable levels of heterogeneity in the literature (I2=99.82). Heterogeneity of studies also results in a 95% prediction interval of −3.17 to 8.14, which does not meet historical thresholds of statistical significance. The prediction interval describes the likely result of a future study based on the existing literature generation process. Heterogeneity also resulted in a higher than expected opposite effects proportion of 19.0%, which can be interpreted, for example, as indicating that reducing exposure to tobacco retailers decreases likelihood of smoking for 81.0% of populations while increasing it for 19.0%. A meta-analysis of health outcome effect sizes (k=30 from n=2 studies) indicated no statistically significant association: RRR=0.01 (95% CI −0.01 to 0.03). However, 24 of the 30 effects came from a single study.19 All subsequent results are reported solely for behavioural outcomes unless noted.
Regarding the estimated proportion of meaningful effects (ie, finding a RRR of ≥1.00), an estimated 70% of behavioural effect sizes would be of a meaningful magnitude and direction to improve public health.
Separate meta-analyses
Table 2 shows separate meta-analyses by outcome variable measurement, predictor variable measurement, study design, reporting of population-specific results and policy context. Each row can be interpreted as its own meta-analysis including just the study results corresponding to the characteristic reported in that row. For example, there is an estimated 2.06% (95% CI 1.26 to 2.85) reduction in risk of smoking with reduced exposure to tobacco retailer density and proximity in those studies that measured smoking as an outcome variable.
Separate meta-analyses by study characteristics estimating relative risk reduction (RRR) in tobacco use from reduction of tobacco retailer density and proximity, k=285, n=27
Meta-regression
We modelled the estimated change in the size of the effect based on study characteristics in unadjusted and adjusted multilevel models (table 3). For example, in the unadjusted model, compared with studies measuring smoking as the outcome variable, studies measuring quitting (reverse coded) are associated with a larger estimated RRR (b=3.81, 95% CI −2.09 to 9.71), which did not reach statistical significance. After controlling for other study characteristics in the adjusted model, again compared with studies measuring smoking status as the outcome variable, studies that assessed quitting were associated with a smaller RRR (b=−1.17, 95% CI −7.49 to 5.16), which also did not reach statistical significance.
Unadjusted and adjusted mixed models regression predicting change in effect size from study and effect size characteristics, k=285
Given the substantial heterogeneity in studies and their reported effect sizes, many characteristics are not statistically significant. However, after adjustment for other study characteristics, there were some differences by type of outcome measured, with smaller estimated RRRs for studies measuring relapse, initiation and other psychosocial variables than for those measuring smoking. Results from longitudinal studies showed significantly greater RRR versus those from cross-sectional studies (b=11.09; 95% CI 5.95 to 16.23). In other words, studies that were longitudinal found a larger benefit to public health from reducing tobacco retailer density and proximity. Significant adjusted results were present for effect sizes where a study predictor variable was delinearised or collapsed into two or more categories (which would, by definition, increase effect sizes78). We found significantly higher RRR in studies focused on men compared with results aggregating men and women and for levels of smoking intensity. However, the 40 effect sizes reported for specific genders and the 32 effect sizes reported for specific levels of intensity should be interpreted with caution as they come from just three studies55 57 59 and one study,55 respectively. Other characteristics with few effect sizes or effect sizes from few studies should also be interpreted with caution.
Discussion
Principal findings
Overall, the meta-analysis indicated that there was an estimated 2.48% reduction in risk of tobacco use behaviours with reduced exposure to tobacco retailer density and proximity as defined by the average included study. In the separate meta-analyses, the pattern of results was the same for both studies of smoking and quitting, although findings from studies of relapse, adult initiation and health outcomes were equivocal. Relatively few studies assessed these outcomes. Results were also in the same direction across different study designs, countries and policy contexts suggesting that our principal findings are robust. The direction of results did differ among results specific to certain populations: unlike for results specific to low-income individuals, results specific to high-income populations were in the opposite direction, suggesting less impact of density and proximity for high-income than low-income populations. Similarly, among results specific to tobacco use intensity, results suggested density mattered more for people who used tobacco more rather than less. While these findings are based on few studies for individual and area-level income44 63 and smoking intensity,55 they suggest further attention is needed to the moderating role of participant income and nicotine dependence as well as the possibility that retailer reduction policies might reduce health inequities.
In the regression approach, we controlled for potentially confounding study characteristics. One of the most striking findings is the larger effect sizes from studies with longitudinal (vs cross-sectional) designs. That better causal inference from longitudinal data is associated with findings that are suggestive of greater public health benefit from supply reduction is promising. Compared with studies that assessed smoking, studies that assessed relapse, young adult initiation and psychosocial variables (eg, quit efficacy, stages of change) showed smaller effects. For disease and young adult initiation, it is plausible that tobacco retailer density and proximity may have limited impact and thus the smaller effect sizes are consistent with the underlying theory of influence. Each of these was also measured in few studies. Further studies should directly assess relapse. We also examined the associations of retail advertising and product display restrictions with the magnitude of the RRR, but neither was significant after controlling for other study characteristics.
Regarding measurement of density and proximity, meta-analysis results were consistent in magnitude and direction, except for measures of density assessed retailers per population, which was not significant and had an estimate near zero. Differences in the size of the magnitude of associations may also result from the meaning of a one-unit change in retailer density or proximity. For example, many count-based studies reported a one-unit change in the number of retailers. But, a one-unit change in retailers per land area as well as approaches that tertile and dichotomise could produce a larger effect size as an artefact of the one-unit-change interpretation in the regression model. Interpreting the existing literature is made more complex by the varied approaches to operationalise exposure variables such as the presence of a retailer (also identified by Valiente et al 18) or dichotomising based on comparisons of quartiles, which may inflate effect sizes and reduce power to detect an effect.78 Just one study measured tobacco retailer density per population,76 which is more commonly measured in studies about inequitable distribution of tobacco retailers.79 80 Further studies should assess the use of per population measures of retailer density with adult tobacco use behaviours and health outcomes.
Logically, strategies to reduce tobacco retailer availability are designed and implemented to focus on administrative boundaries (eg, capping the number of retailers within a district). However, further research that captures dynamic activity spaces, rather than static residential areas, is important to better measure individual-level exposure to tobacco retailers and can provide evidence about the need to implement policies that reduce tobacco retailer availability everywhere and promote a more equitable distribution of tobacco retailers.
Findings in context
Our findings are broadly in line with the one meta-analysis focused on adolescent populations by Finan et al, which found a significant relationship between density of retailers around homes and adolescent smoking (OR 1.08, 95% CI 1.04 to 1.13).14 Assuming 20% youth smoking prevalence, the finding by Finan et al converts30 to an estimated RRR of 1.57 (95% CI 0.79 to 2.53), which is only slightly smaller than our estimated RRR of 2.55 (95% CI 1.91 to 3.19) for density.
The current findings complement a series of prior systematic reviews that have found a link between tobacco retailer density with tobacco use behaviours among adolescents and adults.17 18 81–83 However, conclusions from prior research are inconsistent about the impact of proximity with some reviews finding proximity matters,17 others not assessing proximity14 and others finding inadequate evidence.15 16 Valiente et al found only one association of proximity with cessation in their systematic review of youth and adult studies.18 The current study provides more evidence that proximity to tobacco retailers matters for adults. It parallels results of studies published after our search was conducted,84 85 including one showing associations between density and chronic obstructive pulmonary disease hospital outcomes.86 It also parallels studies not eligible for inclusion that found impacts on some smoking behaviours from removal of tobacco in some pharmacy chains.87–89
A review by Glasser and Roberts examined evaluations of change in tobacco retailer density/proximity based on different policy interventions.83 The authors note that although implementation of policy interventions on density/proximity is growing, there has been more attention to immediate end points (eg, tobacco retail availability and environmental equity, as reviewed by Glasser and Roberts) than to subsequent health behaviours (eg, tobacco use/cessation, as reviewed in the current study). Thus, more evidence of the impact of real-world policy interventions on the retail environment and subsequent tobacco-related behaviours is much needed. This meta-analysis is consistent with evidence that such interventions should have a meaningful impact on health behaviours.
Although our review is limited to OECD countries, our findings match a small literature examining these relationships in lower-income countries. For example, Agaku et al found the presence of tobacco retailers on school grounds were associated with smoking behaviours among school personnel in 19 sub-Saharan African countries.90
The findings regarding proximity are consistent with the underlying theoretical frameworks identified to address why the tobacco retail environment matters to health. Shareck et al, drawing on theoretical approaches to understanding neighbourhoods and health,10 argue that the physical environment provides access and exposure to tobacco products and (in many countries) retail marketing.8 Of course, behaviours are also influenced by price, local norms and other community factors. While it is beyond the scope of the current study to test for evidence to support the underlying theories, the findings do confirm that the tobacco retail environment is an important correlate of behaviour and potential target for policy change.83 91 92
Strengths and limitations
A strength of this review is a robust search including grey literature, designed by a health sciences librarian that resulted in the identification of 37 papers. It followed standard systematic review methods to reduce the potential for bias by assessing papers for risk of bias and adding in a screening for predatory journals. This review also included the largest number of studies to date and incorporated distal tobacco-related disease outcomes. However, conclusions may be impacted by publication bias, as indicated by a funnel plot.
We sought to use an effect size (RRR) that is meaningful and easy to interpret in translational research.30 This strength must be balanced against the challenges of converting between asymmetric effect sizes where negative relationships range from 0 to 1 and positive relationships range from 1 upwards. Some research reports likelihood of smoking (hypothesised to be higher) and some reports likelihood of quitting (hypothesised to be lower). The strength of a straightforward measure is also a limitation as it provides the potential for bias in the conversion from odds to risk.93 Nonetheless, we, like Mirzazadeh et al,30 think these limitations are outweighed by the utility of the RRR.
Second, meta-analyses were historically used for one outcome per study, and including more than one outcome per study can violate the assumption of independence in traditional statistical models. Although our approach of including multiple effect sizes from a given study may underestimate SEs and gives more weight to studies reporting more outcomes, it fits with our interest in exploring the heterogeneity between effect sizes, use of stratified and meta-regression approaches and focus on interpreting the pattern of direction in results. Additionally, the regression models we use account for nesting of effects within studies to account for potential bias in SEs.
Third, there is substantial heterogeneity in the reviewed literature, which indicates the included studies did not all measure the same phenomenon. Given the limitations of our approach described above, readers are advised to focus on the pattern and direction of results. However, heterogeneity can also be overestimated with large, precise studies that do not have overlapping CIs, which has been identified as a problem in other meta-analyses.94 Heterogeneity in the current study is likely the result of both factors. Our attempt to control heterogeneity by limiting our review to OECD countries excluded emerging evidence from low-income countries.
The current study assessed the level (individual vs neighbourhood) at which variables were conceptualised as mediators and confounders. In separate meta-analyses, our pattern of results was similar for studies with individual level and both individual and area-level covariates. Given the compelling prior work of Nuyts et al 16 examining in depth the control for covariates and confounders (and lack thereof) in the youth and young adult literature, the current study did not assess every covariate. We instead refer readers to their excellent discussion of overadjustment (ie, inclusion of potential mediators) and underadjustment (ie, omission of potential confounders).16
Conclusions
In summary, this meta-analysis supports prior reviews’ evidence of the relationship between tobacco retailer density and tobacco use behavious. Regardless of how density and proximity are measured or what country the research is conducted in, the general pattern of association is consistent: reducing the density and proximity of tobacco retailers is consistently associated with reductions in adult tobacco use. We extend the previous body of literature to a larger number of papers, provide the first meta-analysis of this relationship among adult populations and provide clear evidence of the importance of proximity. We suggest that future research attend to the theorised mechanisms through which these associations are produced and leverage stronger quasi-experimental designs that allow for better understanding the mechanisms through which policy changes influence health behaviours and outcomes. Based on the existing literature linking tobacco retailer density and proximity with tobacco use behaviours and other health-relevant outcomes, policymakers should consider that supply reduction strategies to reduce tobacco retailer density and proximity will likely result in improvements to population health.
What this paper adds
The density of tobacco retailers matters to youth tobacco use according to prior meta-analyses.
No studies have meta-analyzed tobacco retailer density and proximity in relation to adult tobacco use behaviors and health outcomes.
Prior research has noted methodological challenges to understanding the role of tobacco retailer density and proximity on behavior.
Overall, this meta-analysis indicated that there was an estimated 2.48% reduction in risk of tobacco use behaviors with reduced exposure to tobacco retailer density and proximity as defined by the average included study.
Policymakers should consider that supply reduction strategies to reduce tobacco retailer density and proximity will likely result in improvements to population health.
Data availability statement
Data are publicly available in the East Carolina University dataverse, https://doi.org/10.15139/S3/6175L7.
Ethics statements
Patient consent for publication
Ethics approval
As no human participants were involved in this study of published papers, we did not seek ethics approval.
Acknowledgments
The authors would like to thank Emmanuel McLeod and Sneha Amaresh for help with screening and record management.
Footnotes
Twitter @Joseph_GL_Lee, @AmandaYKong, @KurtRibisl
Contributors JGLL developed the protocol, coded data, abstracted data, drafted the manuscript and conducted the analyses; AYK developed the protocol, coded data, abstracted data and drafted the manuscript; KBS developed and implemented the search and coded data; SDG developed the protocol and drafted the manuscript; TBC created figures; KMR originated the study, developed the protocol and drafted the manuscript; LH drafted the manuscript. All authors provided critical feedback, edited the manuscript and approved its final submission.
Funding Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health under Award Numbers P01CA225597 and T32CA128582. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests JGLL and KMR hold a royalty interest in tobacco retailer mapping system owned and licensed by the University of North Carolina at Chapel Hill. The software was not used in this research. KMR is a paid expert consultant in litigation against electronic cigarette companies.
Provenance and peer review Not commissioned; externally peer reviewed.
↵((“Tobacco Industry”[Mesh] OR “Tobacco Products”[Mesh] OR “Tobacco”[Mesh] OR “Smoking”[Mesh] OR Tobacco[tiab] OR Tobacconist[tiab] OR Tobacconists[tiab]) AND (“Commerce”[Mesh] OR “Marketing”[Mesh] OR Outlet[tiab] OR Outlets[tiab] OR Retail[tiab] OR Retailer[tiab] OR Retailers[tiab] OR “point of sale”[tiab] OR “point-of-sale”[tiab] OR “points of sale”[tiab] OR “points-of-sale”[tiab] OR Vendor[tiab] OR Vendors[tiab] OR Shop[tiab] OR Shops[tiab] OR Business[tiab] OR Businesses[tiab] OR Sale[tiab] OR Sales[tiab] OR Commercial[tiab] OR Market[tiab] OR Markets[tiab] OR Consumer[tiab] OR Consumers[tiab] OR Seller[tiab] OR Sellers[tiab] OR Store[tiab] OR stores[tiab]) AND (“Residence Characteristics”[Mesh] OR “Censuses”[Mesh] OR “Spatial analysis”[Mesh] OR “Geographic Mapping”[Mesh] OR “Demography”[Mesh] OR “Geopolitical Areas”[tiab] OR Census[tiab] OR Censuses[tiab] OR Density[tiab] OR Proximity[tiab] OR Concentration[tiab] OR Distribution[tiab] OR Spatial [tiab] OR Neighborhood[tiab] OR Neighborhoods[tiab] OR Neighbourhood[tiab] OR Neighbourhoods[tiab] OR Zoning[tiab] OR Mapping[tiab] OR “zip code”[tiab] OR “zip codes”[tiab] OR Tract[tiab] OR Tracts[tiab] OR “area unit”[tiab] OR “area units”[tiab] OR Residential[tiab] OR Residence[tiab] OR County[tiab] OR counties[tiab] OR Cluster[tiab]))