Article Text

Abstract
Background Waterpipe smoking is more prevalent than cigarette smoking among adolescents in the Eastern Mediterranean Region (EMR); however, simple prevalence masks complex waterpipe smoking patterns and makes uncertain its contribution to risk of tobacco-related harm. This study aimed to integrate the impact of cigarette and waterpipe tobacco use on toxicant exposure among EMR adolescents.
Methods A cross-sectional model made equivalent individual-level toxicant exposure data for cigarettes and waterpipes, and aggregated it to 23 countries in the EMR using the Global Youth Tobacco Survey. The waterpipe model adjusted for estimated frequency of use, session duration and sharing behaviours. The final model included 60 306 12–17-year olds, and modelled as outcomes nicotine, carbon monoxide (CO) and 14 carcinogens. Sensitivity analyses substantially reduced session duration and proportion of solo use.
Results Our model suggests waterpipe use may contribute a median of 36.4% (IQR 26.7–46.8%, n=16) of the total toxicant exposure from tobacco, and may reach up to 73.5% and 71.9% of total CO and benzene exposure, respectively. Sensitivity analyses reduced all values by 4.3–21.0%, but even the most conservative scenarios suggested over 50% of benzene and CO exposure was from waterpipe use. Between 69.2% and 73.5% of total toxicant exposure derived from dual cigarette and waterpipe users, who smoked cigarettes and waterpipe more frequently and intensely than single users.
Conclusions More research is warranted to refine our model's parameters. Tobacco control researchers should consider a move towards a single unit of measure for cigarette and waterpipe tobacco exposure in order to better inform health policy.
- Carcinogens
- Low/Middle income country
- Non-cigarette tobacco products
- Smoking topography
- Toxicology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Waterpipe smoking is a broad term to describe tobacco smoke that passes through a water apparatus prior to inhalation. Burning charcoal is placed on the apparatus head, separated from underlying tobacco by pieced aluminium foil, resulting in inhalation of a mixture of charcoal and tobacco smoke.1 Unflavoured waterpipe tobacco is centuries old, highly toxic, smoked frequently and largely confined to adult males in the Eastern Mediterranean Region (EMR) and south Asia.2 Flavoured waterpipe tobacco became popular in the 1990s, is ‘less toxic’ than its unflavoured counterpart, smoked infrequently and more commonly smoked by adolescents of both genders in the EMR and south Asia.2 ,3 Among 13–15-year olds in the EMR, past 30-day waterpipe prevalence is highest in Lebanon (36.9%) and the West Bank (32.7%).3 Its popularity has recently extended to Western settings: among 11–18-year olds in the USA, past 30-day waterpipe prevalence increased from 4.1% to 9.4% between 2011 and 2014,4 and in the Eastern European region past 30-day waterpipe prevalence among 13–15-year olds is highest in Latvia (22.7%) and the Czech Republic (22.1%).3
Observational studies have shown that waterpipe tobacco use results in significant nicotine, carbon monoxide and carcinogen exposure.1 ,5 However, such studies are conducted in tightly controlled laboratory environments and may not reflect true population-level waterpipe smoking patterns. In addition to the type and volume of tobacco use, toxicant exposure is likely to be additionally dictated by factors described in table 1.
Factors affecting waterpipe tobacco toxicant exposure
While the available evidence suggests waterpipe tobacco smoking is significantly associated with lung cancer and other tobacco-linked diseases,6 ,7 in these studies waterpipe smoking is often defined as frequently smoking unflavoured waterpipe tobacco (see online supplementary appendix 1), so long-term clinical risks of infrequent waterpipe smokers, or users of flavoured waterpipe tobacco, are uncertain. Health surveys of waterpipe tobacco smoking often omit key information such as frequency and intensity of use which accounts for the wide variability and complexity in which waterpipe tobacco is smoked.8 It therefore remains unclear what volume and concentration of toxicants are being delivered to waterpipe tobacco smokers on a population level, and how this compares to toxicants being delivered to cigarette smokers. The aim of this study was to integrate the impact of cigarette and flavoured waterpipe use on adolescents in the EMR through assessment of exposure to tobacco-related toxicants.
Supplementary appendix 1
Methods
Model design overview
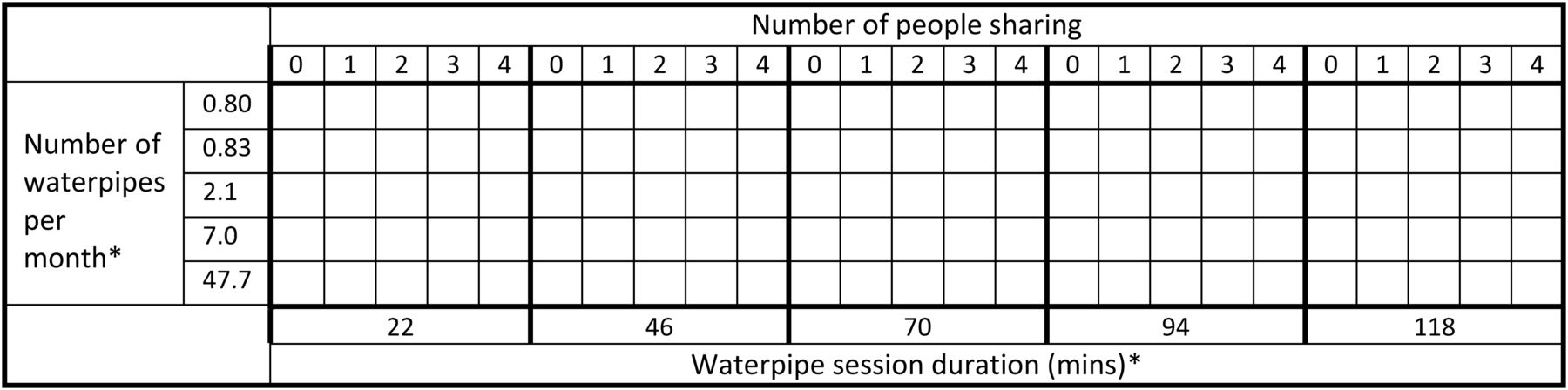
A cross-sectional model applied equivalent individual-level cigarette and waterpipe toxicant exposure data to population-level data in 23 EMR countries, adjusting for consumption patterns that affect waterpipe toxicant exposure. It aimed to determine whether 16 selected toxicants from tobacco were mainly derived from cigarette or waterpipe tobacco use, and from single or dual users. The model distributed past 30-day cigarette users across five states, and waterpipe users across 125 states (figures 1), based on their expected patterns of use. Model input data were of two types: behavioural factors (number of cigarettes/waterpipes per month, waterpipe session duration and group waterpipe behaviour) and toxicant exposure data.

{kind=link}
Overview of the 125 states in the waterpipe model. *Data categorised into quintiles for model simplification.
Behavioural factors
Number of cigarettes and waterpipes per month
We analysed the most recently available data from the Global Youth Tobacco Survey (GYTS) to obtain the number of cigarettes and waterpipes per month among adolescents in the EMR. Details on the GYTS methodology are found elsewhere;18 however, in brief, it is a cross-sectional, self-administered survey that uses a two-stage random probability cluster design to produce nationally representative data among secondary school students typically aged 13–15 years. Of 34 GYTS data sets available from the EMR,19 23 included optional waterpipe tobacco prevalence questions. For the purposes of our model, we assumed all GYTS waterpipe tobacco smokers used flavoured (Mo'assel) waterpipe tobacco.20 ,21
The number of cigarettes and waterpipes per month was ascertained by combining the answers to two GYTS questions. The first question was (A) ‘During the past 30 days (1 month), on how many days did you smoke [cigarettes or waterpipe]?’, and its seven options (0/1–2/3–5/6–9/10–19/20–29/all 30 days) were recoded to correspond to their mean (0.0/1.5/4.0/7.5/14.5/24.5/30.0, respectively). The second question was (B) ‘During the past 30 days (1 month), on the days you smoked how many (cigarettes or waterpipe sessions) did you usually smoke?’ Six options for cigarette use (<1/1/2 to 5/6 to 10/11 to 20/>20 cigarettes per day) were recoded to correspond to their mean (0.5/1.0/3.5/8.0/15.5/20 cigarettes per day, respectively), as were the four options for waterpipe use (<1/1/2 to 5/>5 sessions per day recoded to 0.5/1.0/3.5/5.0 sessions per day, respectively). Multiplying the recoded variables from answers to questions (A) and (B) produced two new variables, one for the number of cigarettes per month (7×6=42 categories) and one for the number of waterpipe sessions per month (7×4=28 categories). For each variable, two duplicate categories were merged into one.
After recoding non-smokers (ie, answering ‘0’ for question A) as missing values, to maintain model simplicity each of these variables was divided into quintiles of equal numbers, for each of which the mean number of cigarettes or waterpipe sessions per month was calculated. For cigarettes, the quintiles were 0.8, 1.3, 4.6, 29.9 and 321.8 cigarettes per month, with 1145 respondents per quintile. For waterpipes, the quintiles were 0.80, 0.83, 2.1, 7.0 and 47.7 waterpipe sessions per month, with 1382 respondents per quintile. In a sensitivity analysis, quintiles were replaced with the original categories for the number of monthly cigarettes (ie, 42) and waterpipes (ie, 28).
We also calculated the prevalence of past 30-day cigarette and waterpipe use, and survey weights were used to account for the complex survey design. Observations with missing data for cigarette or waterpipe prevalence variables were deleted. Past 30-day prevalence calculations were conducted using Stata V.12 (StataCorp), and the model was developed using Microsoft Excel.
Waterpipe session duration
Online supplementary appendix 2a details the search strategy for ascertaining waterpipe session duration data. We took session duration data from a Syrian study by Asfar et al; the only EMR study to our knowledge to report a mean duration with a measure of dispersion (71.1±35.8 min).22 This was a well-designed study among Syrian adults. The following assumptions about this study were made:
Adults have the same session duration as adolescents;
Syrians have the same session duration as all EMR populations;
Session duration has not changed in the past 10 years (ie, since the study was conducted);
Session duration is a normally distributed variable, no <10 min or no >130 min;
All past 30-day waterpipe users fall into one of five smoking durations.
Supplementary appendix 2
The waterpipe session duration was simplified to 70.0±35.0 min and five duration categories were calculated as follows: on a standardised distribution, z-values were calculated for 24 min increments between 10 and 130 min to create five portions under the curve (ie, (130–10)/24=5)). A standard normal table converted z-values to the proportions of cases under each portion of the curve. Resultantly, past 30-day waterpipe users fell into one of five categories for session duration: 22 min (12.1% of past 30-day waterpipe users), 46 min (23.3%), 70 min (29.2%), 94 min (23.3%) and 118 min (12.1%). In a sensitivity analysis, the mean duration was reduced to 50 min (SD 25 min; model A) and 30 min (SD 15 min; model B).
Group waterpipe behaviour
Online supplementary appendix 2a details the search strategy for ascertaining group waterpipe behaviour. Two methodologically sound studies were used to calculate group waterpipe smoking behaviour in three steps. In the first step, Maziak et al,35 a study again among Syrian adults, reported the proportion of solo versus group use among past 30-day waterpipe users. In the second step, among group users, Maziak et al35 also reported the proportion of those who shared the same pipe in each session. In the third step, among group users who shared the same pipe in each session, Jawad et al,23 a study among Lebanese adolescents, reported the number who usually shared their pipe as one, two, three, more than three people. The following assumptions about these two studies were made:
For Maziak et al:35
Adults have the same group behaviours as adolescents;
Syrians have the same group behaviours as all EMR populations;
Group behaviours have not changed in the past 11 years (ie, since the study was conducted);
Smoking in a group, but not sharing a waterpipe, is analogous to solo use.
For Jawad et al23
Lebanese adolescents have the same group behaviours as adolescents from all other nationalities in the EMR;
Sharing with ‘more than three people’ is analogous to sharing with four people.
Based on these three steps, five categories were created for group waterpipe smoking behaviour, reflecting the number of people sharing the same pipe (0, 1, 2, 3 and 4). Maziak et al35 also stratified data by frequency of use, so waterpipe users fell in one of five categories as follows:
Daily use (>29 waterpipe session per month): sharing with 0 (80.2%), 1 (6.5%), 2 (4.8%), 3 (4.9%) or 4 (3.6%) people;
Weekly use (4–29 waterpipe session per month): sharing with 0 (57.5%), 1 (14.0%), 2 (10.3%), 3 (10.5%) or 4 (7.7%) people;
Monthly use (<4 waterpipe session per month): sharing with 0 (47.4%), 1 (17.3%), 2 (12.7%), 3 (13.0%) or 4 (9.5%) people.
In a sensitivity analysis, the proportion of solo use was reduced by 20% (model C) and 50% (model D).
Stratifying all parameters by one another resulted in 125 (=5×5×5) possible states for each past 30-day waterpipe user (Figure 1). The number of participants in each state was populated using GYTS data.
Toxicant exposure data
Online supplementary appendix 2b details the search strategy for ascertaining toxicant exposure data. To our knowledge, only one study24 has calculated area under the curve or 24 h exposure values for toxicants derived from cigarette and waterpipe users in a well-controlled, cross-over design, so only this study was selected for model inclusion. The study included 13, mainly white and male participants. The cross-over design of this study enabled the authors to control for between-person effects. Measured toxicants included plasma nicotine, expired carbon monoxide and 14 urinary carcinogens (16 toxicants in total).
Cigarette toxicant data in Jacob et al24 were given for a cigarette user smoking 11.4 cigarettes per day, so we divided all values by 11.4 to reflect the toxicant exposure for one cigarette. The population-level toxicant exposure for each of the five cigarette states was derived by multiplying this value by the number of monthly cigarettes smoked and the number of respondents in each state. Toxicant exposures for each state were then summed to produce the total population-level toxicant exposure from cigarettes.
Waterpipe toxicant data were given for a solo waterpipe user smoking for 2.8 sessions per day lasting 45.8 min each, so this was standardised to one solo waterpipe session lasting 70 min (ie, by dividing all values by 1.832). The population-level toxicant exposure for each of the 125 states was derived in an identical fashion to cigarettes (multiply toxicant value by the number of monthly waterpipes smoked and the number of respondents in each state), except that the value also factored in waterpipe session duration (ie, multiply by: session duration/70) and the number of others who also share the pipe (ie, multiply by: 1/(number of people sharing+1). Toxicant exposures for each state were then summed to produce the total population-level toxicant exposure from waterpipes.
In these calculations, the following assumptions were made:
All cigarette users smoked with the same intensity and duration;
No cigarette users shared their cigarette with others;
No cigarette or waterpipe users were exposed to secondhand smoke;
The relationship between waterpipe toxicant exposure and (1) session duration and (2) the number of people sharing a waterpipe was proportional, for example, sharing with one person halved the toxicant exposure compared with solo smoking; smoking for 35 min halved the exposure compared with smoking for 70 min;
The amount of tobacco placed in the head of a waterpipe apparatus remained constant regardless of group behaviours and session duration, under the assumption that individual exposure is more a function of underlying dependence rather than starting tobacco weight.25
Sensitivity analyses
Given that most of waterpipe model's data were taken from adult observations, sensitivity analyses adjusted parameters to more accurately anticipate smoking behaviours of adolescents, who we believe are more likely to smoke for shorter durations and engage in more group waterpipe use. The following parameters were changed:
Model A: decrease mean session duration to 50 min (SD 25 min);
Model B: decrease mean session duration to 30 min (SD 15 min);
Model C: decrease proportion of solo waterpipe use by 20%;
Model D: decrease proportion of solo waterpipe use by 50%;
Model E: (1) use the original number of categories for frequency of use to increase number of states for the number of cigarettes per month from 5 to 35, and for waterpipes per month from 5 to 23; (2) increase the number of states for session duration from 5 to 25 by using 5 min increments instead of 24 min increments; resulting in 35 cigarette states and 2875 waterpipe states (=23×25×5).
Given the studies used in these assumptions have small sample sizes and any positive findings may be due to chance or publication bias, parameters in models A–D were not increased. Finally, analyses were stratified by single or dual tobacco use (ie, cigarette only use, waterpipe only use, and dual cigarette and waterpipe use) in order to identify which of these three groups contributed most to population-level toxicant exposure from tobacco.
Results
Cigarette and waterpipe prevalence
Missing data were present in 6.4% of smoking prevalence data, which after removal resulted in 60 306 respondents for analysis. A quarter of the sample originated from the United Arab Emirates (26.0%, n=15 671), otherwise sample sizes from other countries ranged between 932 in Yemen to 4434 in Egypt. All surveys were conducted between 2008 and 2011 except for three (Iran 2007, Qatar 2007 and United Arab Emirates 2005). In line with the target age of GYTS, the majority of respondents were either 14 (22.6%), 15 (23.8%) or 16 (19.0%) years old. Just under half the sample (48.0%) was male.
In total, 6.8% (95% CI 5.9% to 7.9%) reported past 30-day cigarette use and 13.4% (95% CI 11.9% to 15.0%) reported past 30-day waterpipe use. Stratified by single or dual tobacco use, 2.9% (95% CI 2.4% to 3.4%; n=2365) reported past 30-day cigarette-only use, 9.4% (95% CI 8.2% to 10.8%; n=5086) reported past 30-day waterpipe-only use, and 4.0% (95% CI 3.4% to 4.7%; n=3203) reported past 30-day dual cigarette and waterpipe use. The median number of cigarettes per month was 2.0 (IQR 0.75–14.5) for past 30-day cigarette-only users and 7.5 (IQR 1.5–85.8) for past 30-day dual cigarette and waterpipe users. The median number of waterpipe sessions per month was 1.5 (IQR 0.75–7.5) for past 30-day waterpipe-only users and 4.0 (0.75–24.5) for past 30-day dual cigarette and waterpipe users.
Model results
Results of the model are presented in table 2. Across all 16 toxicants, waterpipe users contributed a median of 36.4% (IQR 26.7–46.8%) of the total toxicant exposure from tobacco, and cigarettes contributed the remainder. Four toxicants more derived from waterpipe tobacco smoking than cigarette smoking were carbon monoxide (73.5%), benzene (71.9%), pyrene (56.9%) and phenanthrene (52.1%).
Total population-level toxicant exposure from cigarette and waterpipe smoking among adolescents in the Eastern Mediterranean Region
Table 3 presents results from the sensitivity analysis. Models A–E are presented in terms of waterpipe toxicant exposure as a percentage of total tobacco toxicant exposure. As expected, models A–D showed a reduction in the waterpipe toxicant exposure as a percentage of total tobacco toxicant exposure, with an absolute percentage decrease by 4.3–8.4% for model A (reduce session duration to 50 min), 9.0–21.0% for model B (reduce session duration to 30 min), 5.7–11.5% for model C (reduce proportion of solo use by 20%) and 7.8–17.0% for model D (reduce proportion of solo use by 50%), depending on the toxicant. Model E (increase in the number of cigarette and waterpipe states) showed an increase in waterpipe toxicant exposure as a percentage of total tobacco toxicant exposure by an absolute percentage increase of by 5.6–8.9%, depending on the toxicant.
Results of sensitivity analysis (%)
Table 4 presents the extent to which total toxicant exposure from tobacco is derived from cigarette-only, waterpipe-only, or dual cigarette and waterpipe users. For all toxicants, between 69.2% and 73.5% of total toxicant exposure from tobacco was derived from dual cigarette and waterpipe users. Only five toxicants (carbon monoxide, phenanthrene, pyrene, acrylamide and benzene) were derived in higher proportions from waterpipe-only users compared with cigarette-only users.
Population-level toxicant exposure stratified by single or dual tobacco use (%)
Discussion
Main findings
To our knowledge, this is the first study to attempt to integrate the impact of cigarette and waterpipe tobacco on toxicant exposure using a population-level approach. Though past 30-day waterpipe prevalence was double that of cigarettes (13.4% vs 6.8%), our model suggests the majority of total population-level toxicant exposure from tobacco was derived from cigarette use in 12 out of 16 toxicants. However, waterpipe use may produce substantially higher levels of carbon monoxide and benzene relative to cigarettes, accounting for about 70% of total population-level toxicant exposure from tobacco. Furthermore, our model suggests that around 70% of total population-level toxicant exposure from tobacco may come from the 4% minority of dual cigarette and waterpipe users.
There is considerable variation in waterpipe tobacco smoking behaviour; however, in general its smoke is less concentrated than cigarette smoke.1 Considering it is often a shared, infrequent activity, waterpipe users are therefore theoretically exposed to less toxicants than cigarette users. While infrequent use may be due to the low nicotine absorption and hence unlikeliness to be dependent, another explanation may be due to the fact that waterpipe tobacco is mainly accessible at cafes and bars, which are expensive venues for regular waterpipe use and should deny access to adolescents for whom it would be illegal to buy tobacco.
Notwithstanding, waterpipe sessions can last several hours, so even infrequent users may be exposed to significantly high levels of toxicants. Young adults may also ‘binge’ on waterpipe tobacco at social venues in a similar fashion to alcohol consumption in this age group;26 a behaviour we hope to have captured in our model given we measured chronic average waterpipe tobacco consumption using a normally distributed session length variable. Furthermore, the fact that waterpipe tobacco requires a continuous combustion source makes it distinctly unique to cigarettes and explains the high levels of carbon monoxide and benzene exposure, which are found in charcoal.27 ,28 The WHO has stated benzene, due to its carcinogenicity, is a major public health concern of which there is no safe level of exposure.29 The long-term implications of carbon monoxide exposure are less clear, but may involve cognitive and neurological deficits and cardiac ischaemia.30
The majority of population-level toxicant exposure appears to derive from dual cigarette and waterpipe smokers rather than single users. Even though only 4.0% of the sample were dual users, the GYTS analysis showed that dual users smoke more cigarettes per month (7.5 vs 2.0), and more waterpipe sessions per month (4.0 vs 1.5), than single users. Dual users attain their nicotine from more than one source and may therefore be more nicotine-dependent than single users, hence resulting in more frequent and intense use of both products.
Strengths and limitations
The integrative approach to cigarette and waterpipe harm that this study sought to address is novel and could be considered more widely in tobacco control. Our model uses large and nationally representative data sets across the EMR, taken from a validated tobacco survey, to accurately measure the prevalence and frequency of tobacco use among adolescents. Even though most other input data were taken from adult studies, sensitivity analyses adjusted the model's parameters to better reflect adolescents' expected waterpipe smoking behaviours.
This study has several limitations. The quality of the model is reflective of the quality of data to inform it. While the GYTS is valid and robust source of data for information on smoking frequency, other parameters used in the model relied only on assumptions from one or two studies that may not be generalisable to the secondary school population of the EMR. For example, data on waterpipe session duration were taken from Syrian adults who smoked at waterpipe-serving premises,22 who are more likely to be dependent,31 and therefore more likely to have longer waterpipe session durations than adolescents. Toxicant data were only single estimates and were taken from mainly white and male US adults, which is important as there are age, gender and ethnic differences in the metabolism of tobacco-derived toxicants.32 Using single toxicant estimates may threaten the validity of our model; however, a recently published meta-analysis of waterpipe tobacco toxicant exposure33 generally agrees that this exposure profile is likely among waterpipe users. Although toxicants used for this model were derived from plasma and urine samples, measurement bias is minimised as the sampling method was conducted for each toxicant across both tobacco products and we did not compare toxicant values against one another. Recently published data from a well-designed cross-over study in the USA suggested that individuals sharing in a dyad session may be exposed to roughly 51% less nicotine and 59% less carbon monoxide compared with individuals in a singleton session,13 which is not too dissimilar to our assumption of a 50% reduction in a dyad session. This, and the systematic review of waterpipe toxicant exposure, has shown that our original estimates are stable and adds weight to the validity of our model. Toxicant exposure data from groups of three or more are still lacking; however, a stepwise reduction in toxicant exposure is likely due to reduced puff frequency.34 Notwithstanding, more research among adolescents is required to confirm or refute existing adult observations about waterpipe-sharing behaviours and session duration. It was not possible to assess criterion validity of our model due to the absence of studies using similar methodological designs. It was also not possible to model our exposure on a single tobacco ‘unit’ as it is unclear which toxicant in tobacco the ‘unit’ should be based on. Validating our model against biological markers or health outcome data was not possible due to the lack of high-quality studies measuring both health outcomes and well-characterised waterpipe use.6 Our model lacks content validity given only 16 toxicants were included out of several thousand identified in tobacco; however, emission data from waterpipe tobacco studies are relatively consistent in that carbon monoxide is among the single most highly produced toxicant.33
The model itself omitted several important adjustments including an estimation of tar exposure and other harmful chemicals likely to induce disease. It did not consider the influence of male gender and dual waterpipe and cigarette use on waterpipe smoking behaviour patterns. These two characteristics are likely to be associated with longer session duration and greater solo use.35 ,36 Age is also an important factor: adults in parts of the EMR nearly exclusively use unflavoured waterpipe tobacco,2 which is ‘more toxic’ than the flavoured tobacco modelled in this study. To the best of knowledge, there are very limited data assessing toxicant exposure of unflavoured waterpipe tobacco users.15
Implications
This study highlights the need for better designs of epidemiological surveys addressing waterpipe tobacco smoking, in order to capture the tobacco type, expected dose of use and subsequent risk of harm. High-quality waterpipe and cigarette toxicant exposure cross-over studies are severely lacking, and these should include larger samples in order to allow meaningful stratification of results by gender and dual cigarette and waterpipe use status. Epidemiological studies on the health outcomes of waterpipe use need more details on waterpipe tobacco exposure in order to estimate its relative long-term harm compared with cigarettes. The lack of literature on unflavoured waterpipe tobacco is concerning given the majority of the adults in parts of the EMR use it instead of flavoured tobacco; details about the potential transition from flavoured to unflavoured waterpipe tobacco throughout the life course is currently unknown. Given unflavoured waterpipe tobacco is ‘more toxic’ and smoked more frequently than flavoured waterpipe tobacco, the relative contribution of waterpipe tobacco toxicant exposure may be even greater if this study was replicated among adults. Tobacco control researchers should consider a move towards a single unit of measure for cigarette and waterpipe tobacco exposure in order to better inform health policy.
Conclusions
While the prevalence of waterpipe tobacco use is higher than cigarette use in this sample of adolescents from the EMR, on a population level our model suggests cigarette smoking remains the main contributor to the burden of toxicant exposure caused by tobacco. Notwithstanding, waterpipe tobacco smoke may expose users to relatively high levels of carbon monoxide and benzene which are likely to increase smoking-related diseases, particularly as the latter is carcinogenic with no safe level of exposure. Better epidemiological data are needed to inform future iterations of our model. Given the widespread popularity of waterpipe tobacco smoking, behavioural interventions should be developed to prevent uptake and promote cessation; particularly among dual users. Ongoing tobacco surveillance is required to understand the epidemiological course that waterpipe tobacco is taking alongside greater tobacco control measures.
What this paper adds
Waterpipe tobacco smoking is more prevalent than cigarette smoking among adolescents in the Eastern Mediterranean Region.
Waterpipe tobacco use is associated with adverse health outcomes typically seen with cigarette use.
Studies on health outcomes are restricted to frequent and established users of unflavoured waterpipe tobacco, whereas adolescents intermittently use the ‘less toxic’ flavoured (Mo'assel) waterpipe tobacco.
Prevalence measures do not capture the complexity of waterpipe tobacco behavioural patterns.
This study highlights a new approach to integrating the impact of cigarette and waterpipe smoking on a population level.
Our model suggests the majority of population-level toxicant exposure continues to derive mainly from cigarettes, especially for nicotine.
However, products of charcoal combustion (carbon monoxide and benzene) are mainly derived from waterpipe tobacco use, not cigarette use.
This study highlights a need for more accurate data on waterpipe smoking behaviours and the need for control measures to minimise harm from waterpipe tobacco use.
Acknowledgments
The authors thank Simon Fraser and Nisreen Alwan, at the Academic Unit of Primary Care and Population Sciences, for reviewing this study's protocol. They also thank Kamran Siddiqi, Senior Lecturer in Public Health at the University of York, for providing constructive comments on an earlier draft of this manuscript.
References
Footnotes
Contributors MJ and PR conceptualised the study. MJ conducted the literature review, developed the model and conducted the statistical analysis under the supervision of PR. MJ wrote the first draft of the manuscript. Both authors read and approved the final version of the manuscript.
Competing interests None declared.
Ethics approval Local ethical approval was sought for each institution involved in the Global Youth Tobacco Survey.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are publically available—the authors have referenced this in the manuscript.