Article Text

Abstract
Objective: To describe the characteristics of betel quid chewers and to investigate the behavioural and mortality relations between betel quid chewing and cigarette smoking.
Method: Prevalence and mortality risks of betel quid chewers by smoking status were calculated, based on the National Health Interview Survey in 2001 and a community based cohort, respectively. Cox’s proportional hazards model was used to adjust mortality risks for age, alcohol use, and education.
Results: Almost all betel quid chewers were smokers, and most started chewing after smoking. Chewers were predominantly male, mostly in their 30s and 40s, more likely being among the lowest educational or income group, and residing in the eastern regions of Taiwan. On average, betel quid chewers who smoked consumed 18 pieces of betel quid a day, and smoked more cigarettes per day. Far more smokers use betel quid than non-smokers (27.5% v 2.5%), but ex-smokers quit betel quid more than smokers (15.1% v 6.8%). The significantly increased mortality of betel quid users who also smoked, for all causes, all cancer, oral cancer, and cancer of the nasopharynx, lung, and liver, was the result of the combined effects of chewing and smoking. Smokers who chewed betel quid nearly tripled their oral cancer risks from a relative risk of 2.1 to 5.9. Increasing the number of cigarettes smoked among betel quid chewers was associated with a synergistic effect, reflective of the significant interaction between the two.
Conclusion: To a large extent, the serious health consequences suffered by betel quid chewers were the result of the combined effects of smoking and chewing. Betel quid chewing should not be considered as an isolated issue, but should be viewed conjointly with cigarette smoking. Reducing cigarette smoking serves as an important first step in reducing betel quid chewing, and incorporating betel quid control into tobacco control may provide a new paradigm to attenuate the explosive increase in betel quid use in Taiwan.
- IARC, International Agency Research against Cancer
- ICD-9, International classification of diseases, 9th revision
- NHIS, National Health Interview Survey
- PPS, probability proportionate to size
- betel quid
- prevalence
- health risks
Statistics from Altmetric.com
- IARC, International Agency Research against Cancer
- ICD-9, International classification of diseases, 9th revision
- NHIS, National Health Interview Survey
- PPS, probability proportionate to size
Areca nut chewing is a practice of great antiquity in many parts of Asia and among some migrant communities in Africa, Europe, and North America.1–4 It is said to be the fourth most commonly used psychoactive substance in the world after caffeine, tobacco, and alcohol.5 While most populations chew areca nut by adding tobacco, in Taiwan, the product, called betel quid, is used without tobacco.1,6 Betel quid in its most basic form consists of betel leaf (Piper betel), areca nut, slaked lime (aqueous calcium hydroxide), and various spices.1,5,7 In contrast to other Asians using sliced pieces of ripe betel quid, people in Taiwan consume the green unripe areca fruit in its entirety, approximately the size of an olive. Three major types are commonly encountered: (1) Lao-hwa quid—a split areca nut is sandwiched with the inflorescence (flower) of Piper betle Linn., spiced with red lime; (2) betel quid—a whole areca fruit is wrapped with betel leaves spread with white lime; (3) stem quid—a split areca fruit is sandwiched with the stem of Piper betle Linn., spread with white lime. This last type is exclusively consumed by aborigines in a home grown environment.1
Areca growing and the sale of betel quid have increased since the opening of the cigarette market and are now a rapidly expanding business in Taiwan.8 Although international tobacco companies have not been directly involved in marketing the product, betel quid producers have created innovative neon-lit roadside kiosks nationwide, using thinly clad young women, popularly known as “Betel Quid Barbie”, to sell betel quid and cigarettes to motorists.9
The per capita consumption of betel quid in Taiwan has increased more than fivefold in 15 years, from 1.4 kg in 1981 to 7.5 kg in 1996.10 This large increase has occurred despite government efforts alerting the public of its hazards and mounting extensive screening programmes for early signs of oral cancer.11
Betel quid contains phenolic compounds and alkaloids, and the mixture has both stimulant and tranquilising pharmacological effects.3,12,13 Like tobacco, the alkaloids are known to be psychoactive on both the sympathetic and parasympathetic nervous system by releasing adrenaline or noradrenaline (epinephrine and norepinephrine), with the modulation of cholinergic and monoamine transmission.3,14,15 Chewing betel quid is a complex, poorly studied behaviour. It has been reported to produce a multitude of subtle effects, such as increasing body temperature and pulse rate, improving concentration, heightening alertness, staving off hunger, or lifting one’s mood with a sensation of wellbeing.16,17 A variety of sociocultural factors, such as peer pressure, social identity, family support, and the attractiveness of Betel Quid Barbie in promoting its sale6,18–25 has been associated with the initiation of betel quid.
While betel quid chewing has been extensively studied in populations in many parts of the world,5 its relation with smoking has received less attention. Such a relation is of particular importance in Taiwan where the public and the medical professionals have long considered betel quid chewing and smoking as two separate issues. This is because chewing and smoking appear to be two distinctly different behaviours and the physiological effect of betel quid does not involve nicotine addiction, an important component of smoking. The purpose of this study is to describe the characteristics of betel quid chewers and to investigate the behavioural and mortality relations between betel quid chewing and cigarette smoking.
METHODS
Betel quid use and smoking
The prevalence of cigarette smoking and betel quid chewing was calculated from National Health Interview Survey data in 2001.26 With the family serving as a survey unit under a scheme of PPS sampling (probability proportionate to size of the population), the resulting survey included 6592 families, covering 26 685 individuals of the non-institutionalised resident population. Over 90% of the households (91.1%) and individuals (94.2%) responded to the survey. As a result, the sample is nationally representative and no further weighting was necessary.27
Current smokers were defined as daily or occasional smokers, who had smoked at least 100 cigarettes in their lifetime.28 Ex-smokers were those smokers who had not smoked for the previous 30 days. Chewers were asked the number of years they had chewed, age of initiation of betel quid use, and whether they were currently chewing (either daily or occasionally), or had already quit. We excluded those having tried betel quid only once or twice in their lifetime. The number of years since quitting was also obtained from ex-chewers. Only data from males were used in the analysis because of the low rates of smoking (4.7%) and betel quid chewing (1.5%) among females. A total of 8985 male subjects ages 12 and above were included in the analysis.
The data also contained information on sociodemographic characteristics and residence. We consider rates differences by these characteristics. Rate ratios (relative risks) adjusted for age were also calculated for betel quid use between smokers and ex-smokers. Similar analyses were conducted to assess the influence of fathers in their smoking or betel quid use habit on their sons.
Mortality risks
The relative mortality risks were analysed from a cohort, recruited from 1982–1992 for a multiple risk factor study.29,30 Nineteen townships and precincts in Taiwan were selected to represent metropolitan precincts, urban and rural townships in the northern, central, and southern part of Taiwan. Residents in the study areas were invited to participate, provided they were at least 18 years old and had no previous history of cancer or other major diseases.
All participants were interviewed at recruitment. The standardised interview assessed sociodemographic characteristics. Participant’s history of cigarette smoking, betel quid chewing, and alcohol consumption, including initiation age, quantities and years consumed, were also collected. Alcohol use was classified by the response made by the individual to the drinking question. Drinkers, or alcohol users, were limited to those “drinking on a regular basis”, thus excluding occasional or party drinkers. Education was classified as elementary school or lower, middle or high school, and college or higher.
Vital status as of 31 December 2000 and cause of death information were ascertained through matches between cohort members and the computerised national death files. The causes of death were coded according to the International classification of diseases, 9th revision (ICD-9). Among 25 246 men recruited into the study cohort, 19 719 subjects of age 35 or above with complete smoking and betel quid data were selected for the mortality risk analysis. In this paper, we use the generic term “oral cancer” to describe malignant neoplasms of the lip, oral cavity, and pharynx (ICD-9 140–149) in the mortality analysis.
The rate ratios (RR)—that is, relative mortality risks—and their 95% confidence intervals (95% CI) of current smokers with or without betel quid chewing were calculated by comparing them to non-smoking, non-chewing subjects, based on Cox’s proportional hazards model using SAS PHREG procedures.31 These rate ratios were adjusted for age, alcohol use, and education. For cancer and cirrhosis of the liver, we also adjusted for the presence of hepatitis B surface antigen (HBsAg). We conducted a test for parallelism and test for equal intercepts between the two regression lines to examine the interaction between smoking intensity and betel quid chewing on the mortality of oral cancer.32
RESULTS
Betel quid use
Based on the 2001 National Health Interview Survey in Taiwan, 14.4% of males age 18 or above were current betel quid chewers and 4.5%, ex-chewers (table 1). Only 1.5% of females (data not shown) were current chewers and 0.2% ex-chewers. More than one out of four current smokers was a current chewer (27.5%) among adult males, but, in the age group 30–49, one out of three (34.2%). Non-smokers rarely chewed betel quid (2.5% current chewers and 0.5% ex-chewers). Betel quid chewing typically began in adolescence, increased substantially after high school, and peaked between ages 30–49, when the chewing rate reached 20.6%. In other words, one out of every five middle aged men in Taiwan chewed betel quid in 2001.
Prevalence rate (%) of current chewer and ex-chewer of betel quid by smoking status for males in Taiwan
Blue collar workers had a higher chewing rate compared to white collar workers or service industry workers (p < 0.05). Among blue collar workers, more than one out of four was a current chewer (27.3%). Education and income were inversely correlated with the rate of current chewing. The chewing rate of those with the lowest education was significantly higher than those with higher educational levels, and similarly for the lowest income group compared with the higher income groups.
Regional variations were pronounced. The eastern region, a rural, poorer area of Taiwan, had the highest rate (24.0%), while Metropolitan Taipei, an urban, relatively affluent area, had the lowest rate (9.3%). There was a 2.5-fold difference in betel quid use among different areas of the country. The aborigines, residing in some 30 aboriginal townships, and constituting a small fraction of the Taiwan population (0.4%), had an exceptionally high chewing rate of 41.1% for males and 25.3% for females (data not shown). Rates of current chewers in the seven regions were found to be significantly correlated with their respective proportions of those with the lowest education, grade 9 or below, (R = 0.90) or those with the lowest income, US$7000/year or less (R = 0.69). These correlations with the lowest education or lowest income also existed for smoking, but they were stronger for betel quid than for smoking, with current smokers at R = 0.57 or 0.30, respectively.
Almost all chewers were smokers (92.6%), but only a subset of smokers were betel quid chewers. In other words, one third of smokers had ever used betel quid (34.3%). The current rate of betel quid use was substantially higher among current smokers than among non-smokers (27.5% v 2.5%), but a higher rate of ex-smokers quit betel quid than smokers (15.1% v 6.8%). The chance of becoming a betel quid user among smokers was nearly 10 times higher than among non-smokers (age adjusted RR 9.6, 95% CI 7.8 to 11.8). Similarly, ex-smokers were twice as likely to quit chewing as current smokers (RR 2.2, 95% CI 1.8 to 2.9). The proportion of ex-chewers among ever chewers was 20% among smokers, but increased to 69% among ex-smokers, an increase of more than threefold. This observation implied that once the smoker moved on to become an ex-smoker, he also had a much higher chance of quitting betel quid chewing.
The median and mean number of pieces of betel quid chewed by chewers in Taiwan was 15 and 18 per day, respectively. A comparison of the daily smoking amount between chewers and non-chewers (data not shown) indicated that chewers smoked far more than non-chewers for all age groups. For those chewers under age 60, 19% were heavy smokers (20 or more cigarettes per day), but only 8% of non-chewers were heavy smokers.
A male adolescent who had a father who smoked or used betel quid increased their chance of becoming a betel quid user by more than twofold, with RR 2.2 (95% CI 1.3 to 3.5) or RR 2.5 (95% CI1.7 to 3.7), respectively (data not shown).
Table 2 presents the proportion of smokers quitting smoking versus chewers quitting chewing. The chewer/ex-chewer ratio was 3.1 (14.4/4.6), half the smoker/ex-smoker ratio of 6.4 (47.6/7.4). Among those who had ever used betel quid, 24% were ex-chewers, while among those who had ever smoked, 13% were ex-smokers. At any given age, proportionately more chewers quit chewing than smokers quit smoking.
Comparison of the proportion of quitters among ever smokers and quitters among ever chewers
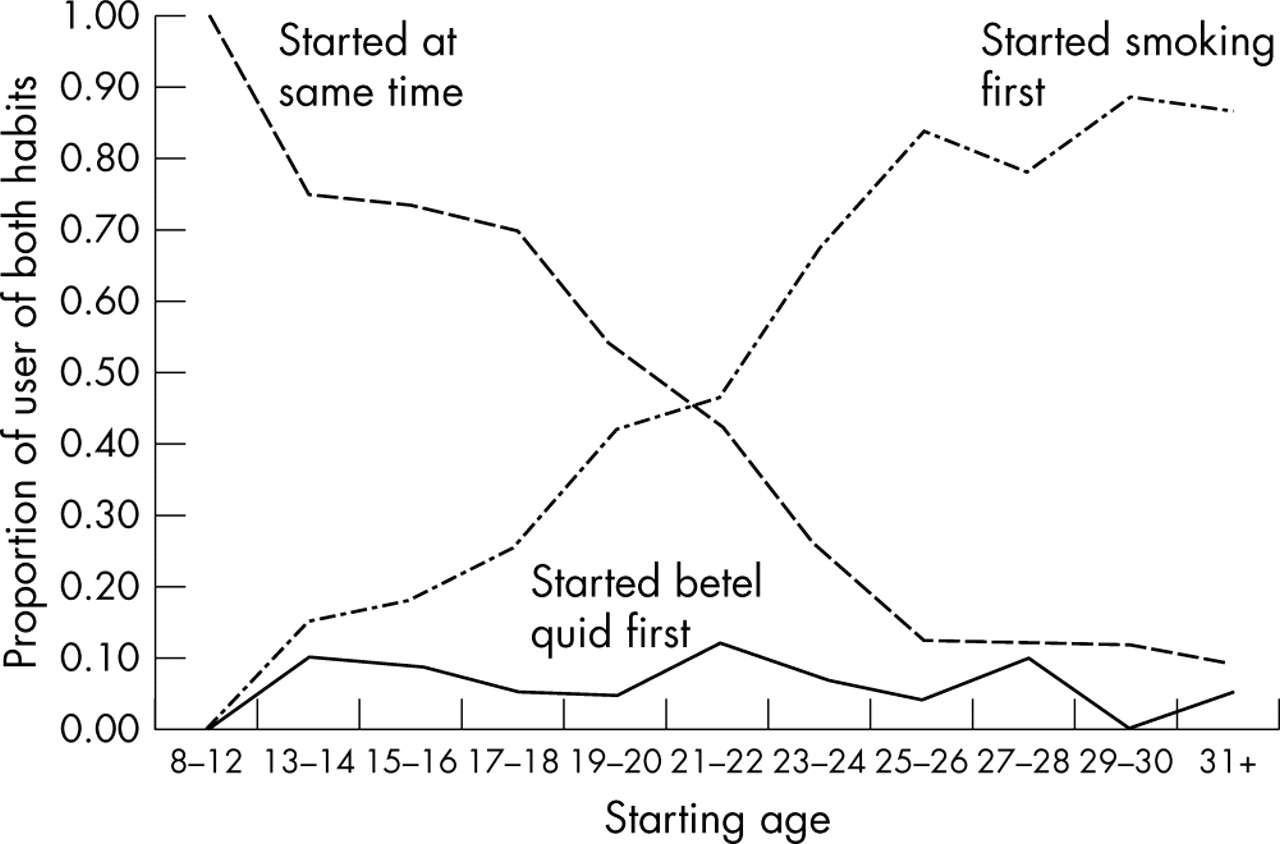
Table 3 examines the distribution of initiation ages of betel quid use relative to the initiation age of smoking among those with both habits. The majority (52%) began chewing betel quid after they started smoking, and only rarely did the chewers start chewing betel quid before the onset of smoking (6%). Over a third, 42%, started both habits at approximately the same time. Figure 1 shows that the proportion starting smoking first was larger than the proportion starting betel quid first for all age groups, but the difference grew rapidly after age 18. If smoking was initiated before or during high school, most started both habits at approximately the same time, but when smoking was started after high school, betel quid use was generally initiated much later than smoking.
Distribution of age at initiation of smoking and betel quid chewing among those with both habits at two year intervals* (n = 1387)

Relative proportions comparing age at initiation among those starting smoking first, starting betel quid first, and starting both habits at the same time.
Mortality risks
The prevalence rate of betel quid chewing in the cohort was 15.1% among smokers (1762/11 647) and 3.7% among non-smokers (302/8072). (This rate of chewers among smokers in late 1980s was approximately half the rate in 2001.) Among betel quid chewers, 85.4% were smokers. The average follow up period was 12.1 years, yielding a total of 239 297 person years of observation.
Table 4 shows a comparison of mortality risks between smokers, with or without betel quid use and non-smokers without betel quid use. The rate ratios presented had been adjusted for age, alcohol use, and education. The number of deaths among betel quid chewers without smoking was too small to estimate meaningful mortality risks. For those with both habits, the RR values for all causes and for all cancer were higher (1.5 and 1.7, respectively) than those with smoking only (1.3 and 1.3, respectively). When smokers used betel quid, the RR nearly tripled for oral cancer, increasing from 2.1 to 5.9. Similar increasing trends were found for several other cancers, including nasopharyngeal cancer (from 1.3 to 4.2), cancer of the oesophagus (from 1.5 to 3.1), liver (from 1.1 to 1.8), and lung (from 2.0 to 2.5). Statistical significance for increased mortality risk was reached among smoking chewers in all cause, all cancers, oral cancer, nasopharyngeal cancer, liver cancer, and lung cancer. Smoking betel quid chewers also had a significantly increased risk of liver cirrhosis (RR 2.5). For cardiovascular diseases as a whole, the additional use of betel quid by smokers did not increase the mortality risks. Smoking without the use of betel quid was associated with a significantly higher stroke mortality risk (RR 1.4), but smoking lost significance when the betel quid habit was added (RR 1.3), most likely due to small sample size.
Age, alcohol and education adjusted rate ratios (RR) by smoking status and betel quid chewing status
The effects of interaction between chewing and intensity of smoking on the oral cancer mortality are shown in fig 2. The age, alcohol use, and education adjusted RR was 2.4 (95% CI 0.3 to 20.0) for light-smoking chewers (10 cigarettes or less a day) when compared to non-smoking non-chewers. This increased to 7.5 (95% CI 2.9 to 19.1) and to 12.2 (95% CI 3.1 to 47.7) for heavier smoking chewers (up to a pack/day and more than a pack/day, respectively). The intercepts between the two regression lines were significantly different, suggestive of an independent risk from betel quid use among smokers, over and above the risk from smoking alone. The RRs increased substantially with increasing smoking intensity at different doses, and the slopes between the two lines were different (p < 0.05, test result for parallelism), indicating that smoking and chewing had a significant interaction.

{kind=link}
{kind=link}
Age, alcohol, and education adjusted rate ratios for oral cancer (ICD-9: 140–149) of smoking chewers and smoking non-chewers when compared with non-smoking non-chewers (RR 1.0) at different smoking intensities.
DISCUSSION
The strong and intriguing relations between the use of betel quid and cigarettes smoking found in this paper could have profound public health implications. Betel quid has long been treated by the public and by health professionals as an isolated issue, independent from smoking. Our findings indicate that chewing and smoking cannot be separated in Taiwan, either from a behavioural perspective (virtually all chewers were smokers) or from a health perspective (the combined effect of betel quid chewing and smoking). The serious health effects of betel quid chewers in Taiwan came not just from betel quid alone but from the combined effects of both.
Chewers in Taiwan were, by and large, a subset of smokers, representing primarily the lower education, lower income, and blue collar segments of smokers. Such a social status of chewers has contributed to an important, and yet, often neglected fact that betel quid chewers consumed more cigarettes per day than non-chewing smokers. There were more than twice as many heavy smokers among chewers than their counterparts among non-chewers.
An important finding is the observation that most chewers started smoking before chewing. In other words, the vast majority of chewers began using betel quid after having already started smoking, thus smoking appears to be a “gateway” for betel quid chewing. The habit of chewing betel quid was formed in addition to, not as an alternative to, smoking. Adolescent chewers started mostly at age 17–20, immediately after high school, along with smoking. Among adults with both habits, more than half started chewing much later than smoking, while smokers rarely started chewing betel quid first.
Another important finding is that those who have quit smoking had as much as a 75% lower prevalence of betel quid use. The age adjusted rate ratio shows that when a smoker quit, he was 2.2 times more likely to stop chewing betel quid. This finding, along with the information on respective initiation age, has implications for substance abuse policy. Smoking prevention and cessation are both critical strategies to reduce betel quid use.
Parental smoking has been shown to be an important factor in developing the smoking habit of adolescents.33–35 In this national survey, if a father was a smoker or a betel quid user, the likelihood of children chewing betel quid increased by more than twofold. This finding reaffirmed the importance of adult smoking behaviour in influencing the betel quid use by children, and gave further credence to the important implications of smoking cessation in reducing betel quid use.
Between 1981 and 1996, per capita consumption of betel quid increased fivefold.10 The prevalence of betel quid chewing in males reported in this study, 14.4% and 27.5%, among adults and among smokers, respectively, were very much higher than those previously reported. For example, in one study from “southern counties” with a relatively high prevalence, the respective rates were 9.8% and 22.5%.6 In this National Health Interview Survey (NHIS) in 2001, the respective rates became 17.0% and 31.3%, about 73% and 39% higher, respectively. Since previous studies reported data from 10 or more years ago, our results provided further evidence that the betel quid consumption has increased substantially in the last decade. During the 15 year period when per capita consumption quintupled, deaths from oral cancer quadrupled, from 241 deaths (2.57 per 100 000, age standardised mortality rate) in 1981 to 941 deaths (7.58 per 100 000) in 1996.1,36 Another 60% increase was seen in the next six years, with 1501 deaths in 2002. It is now ranked as the fifth most common cancer deaths among males in Taiwan, with the largest number in the 40–49 age group. One in five cancer deaths in this age group was from oral cancer,36 while there was one in 30 deaths in Japan, a country without betel quid.37 The risks of dying from oral cancer among betel quid chewers increased multiplicatively with smoking intensity. Similar results have also been reported.38,39
In 1987, the International Agency Research against Cancer (IARC) classified betel quid without tobacco as a group 3 human carcinogen.40 A recent update re-evaluating the evidence has reclassified betel quid without tobacco as a group 1 carcinogen, based on increased cancer risks of the oral cavity, pharynx, and oesophagus.41 Similar conclusions were reached in this study. First, betel quid chewers, with almost all of them being smokers, had increased risks not only for oral cancer, but also for all causes, all cancers, and cancer of the nasopharynx, oesophagus, liver, and lung. This increase arose, not merely from the effects of betel quid alone but most likely from the combined effects of betel quid chewing and cigarette smoking, due, in part, to the fact that betel quid chewers had proportionately more heavy smokers. Second, there was an independent risk from betel quid chewing per se on oral cancer, over and above the risk from smoking. The risk nearly tripled, from 2.1 to 5.9, when smokers picked up the habit of chewing betel quid. Third, at least on oral cancer, there was a strong synergistic effect between cigarette smoking and betel quid chewing, indicating that chewing betel quid progressively aggravated smoking risks at increasing levels of smoking intensity. While hepatitis B and C were associated with liver cancer, betel quid and smoking potentiated that relation also.42–46 It is noteworthy that we did not observe any significant increase in risk for cardiovascular diseases, even though betel quid is known to release adrenaline stimulating the heart and blood vessels.3,47,48
One limitation of the mortality analysis came from the rarity of non-smoking betel quid chewers. Due to the sample size problem, we could not identify the independent mortality risk for betel quid chewing. With either the use of a much larger sample size or longer follow up, future research would be needed to resolve this issue. For the moment, however, our public health community should focus on the combined effects of smoking and betel quid chewing, because they represented the vast majority of betel quid problems.
What this paper adds
Betel quid has recently become popular in Taiwan, with one in four blue collar workers being a chewer. After the cigarette market opened in 1987, the use of betel quid, which has increased by fivefold, is now a major public health concern. During the same period, oral cancer mortality increased fourfold. Chewing was not adopted as an alternative to smoking, but in addition to smoking. Smoking appeared to be a “gateway” to chewing, with almost all chewers being smokers. When smoking chewers quit smoking, most would also quit chewing. Reducing cigarette smoking serves as an important first step in reducing betel quid chewing.
Another limitation of the mortality analysis is that the lifestyle information—for example, betel quid chewing—of cohort members were collected at the time of recruitment, and may have changed over time. This may have led to a non-differential misclassification of betel quid chewing. However, all cohort members were adults over 35 years of age, when the chance of a non-chewer becoming a new chewer after that age was small (2%, according to the 2001 NHIS). On the other hand, approximately 5% of betel quid chewers in this segment quit (table 2). Thus, the potential impact of misclassification would likely underestimate mortality risks. The way these data were collected may have introduced recall/reporting bias because betel quid chewing or smoking status came from self reported information. This potential bias cannot be quantified using data collected for this study. In addition, the possible loss of follow up responses due to migration out of Taiwan was not estimated. The impact on mortality risks could be minimal if there was a similar out-migration rate between chewers and non-chewers.
In conclusion, this study uncovers an intriguing relation between smoking and betel quid use. Betel quid chewing should not be considered as an isolated issue, but always coupled with smoking. Effective policies in smoking prevention and smoking cessation would substantially reduce betel quid use. Reducing cigarette smoking serves as an important first step in reducing betel quid chewing, and incorporating betel quid control into tobacco control may provide a new paradigm to slow the drastic increase in betel quid use in Taiwan.

REFERENCES
Footnotes
-
Competing interests: none declared