Article Text

Abstract
Objectives: To evaluate the long-term effectiveness of recent behavioural interventions in the prevention of cigarette use among children and youth and to compare the effectiveness of different school-based, community-based and multisectorial intervention strategies.
Methods: A structured search of databases and a manual search of reference lists was conducted. Randomised controlled trials published in English or German between August 2001 and August 2006 targeting youths up to 18 years of age were assessed independently by two researchers according to predefined inclusion criteria and with regard to methodological quality. Data abstraction was performed and crosschecked by two researchers. Where appropriate, pooled effect estimates were calculated and tested in sensitivity analyses.
Results: Of 3555 articles, 35 studies met the inclusion criteria. The follow-up duration ranged from 12 months to 120 months. Although the overall effectiveness of prevention programs showed considerable heterogeneity, the majority of studies reported some positive long-term effects for behavioural smoking prevention programs. There was evidence that community-based and multisectorial interventions were effective in reducing smoking rates; in contrast, the evidence for school-based programs alone was inconclusive. Regardless of the type of intervention, the reductions observed in smoking rates were only modest.
Conclusions: The present work identified moderate evidence for the effectiveness of behavioural interventions to prevent smoking. Although evidence for the effectiveness of school-based interventions was inconclusive, evidence for the effectiveness of community-based and multisectorial interventions was somewhat stronger. Future research should investigate the effectiveness of specific intervention components and the cost-effectiveness of interventions analysed in methodologically high-quality studies.
Statistics from Altmetric.com
The hazardous health effects of smoking and second-hand smoke are well known and have been confirmed in numerous studies. In industrialised countries, tobacco smoke is the single most common preventable risk factor for many chronic and potentially life-threatening conditions, such as respiratory, cardiovascular and malignant disease.1–5 The World Health organization (WHO) has estimated that, annually, some 5 million deaths worldwide can be attributed to cigarette smoking.6 Despite this knowledge, the number of individuals who smoke, especially among children and adolescents, remains high or has even increased in recent years in most countries.7 8 Because the majority of smokers become addicted during adolescence, behavioural strategies have often aimed at preventing the initiation of smoking among children and youth.9 10 Traditionally, school-based prevention programs have been used as a way to reach as many children and adolescents as possible. However, because the effectiveness of early behavioural prevention strategies has often been limited or has even led to an increase in smoking rates, prevention programs have been continuously revised since their earliest iterations.11 12 Whereas the first programs aimed at providing smoking-.related health information, later programs have pursued strategies based on social competence or social influence.13–17 Despite these ongoing developments, the evidence regarding the long-term effectiveness of school-based smoking prevention strategies remains limited. Many prevention strategies appear to be effective in the short term, but their long-term effectiveness is often disappointing.18–20 To overcome these limitations, school-based prevention programs have become more comprehensive in recent years, combining a variety of approaches.21 22 Moreover, a number of community-based or multisectorial prevention programs (ie, encompassing school-and community-based approaches) have been implemented in recognition of the multifactorial concept of smoking initiation among youth.23–25 The aim of this systematic review is thus to evaluate the long-term effectiveness of recent behavioural interventions in the prevention of cigarette use among children and youth. A further objective is to compare the effectiveness of different school-based, community-based and multisectorial interventions and to identify the effective components within them.
METHODS
Relevant publications were identified through a structured search of the following databases, accessed through the German Institute of Medical Documentation and Information (DIMDI): German Agency for Health Technology Assessment (DAHTA); International Network of Agencies for Health Technology Assessment (INAHTA) (National Health Service (NHS)-Centre for Reviews and Dissemination (CRD)-Health Technology Assessment (HTA)); NHS Economic Evaluation Database (NHSEED); Cochrane Database of Abstracts of Reviews of Effectiveness (CDAR94) (NHS-CRD-Database of Abstracts of Reviews of Effects (DARE)); Cochrane Database of Systematic Reviews (CDSR93); ME00 (Medline); EM00 (EMBASE); CB85 (Allied and Complementary Medicine Database (AMED)); BA90 (BIOSIS Previews); MK77 (MEDIKAT); Cochrane Central Register of Controlled Trials (CCTR93); GA03 (German Medical Science (gms)); SM78 (SozialMedizin (SOMED)); CV72 (Centre for Agriculture and Biosciences (CAB) Abstracts); II78 (Index to Scientific and Technical Proceedings and Books (ISTPB) + Index to Social Sciences and Humanities Proceedings (ISSHP)); ED93 (Ethics in Medicine (ETHMED)); AZ72 (GLOBAL Health); AR 96 (Deutsches Ärzteblatt); ME0A (Medline Alert); EA08 (EMBASE Alert); IS90 (SciSearch); CC00 (CCMed); IN73 (Social SciSearch); KR03 (Karger Publisher Database); KL97 (Kluwer Verlagsdatenbank); SP97 (Springer Verlagsdatenbank); SPPP (Springer Verlagsdatenbank PrePrint); TV01 (Thieme Verlagsdatenbank).
In addition, a manual search of reference lists included in the articles identified as part of the structured database search described above was conducted. The present review includes German and English literature published between August 2001 and August 2006 and targeting youth up to 18 years of age. Randomised controlled trials (RCTs) were included if they were of a duration of at least 12 months and reported the outcome as a measure of smoking behaviour. When a trial was reported in multiple publications, the latest follow-up outcomes were taken into account. The titles, abstracts and full-texts of all identified studies were reviewed independently by two researchers and evaluated with regard to their methodological quality using standardised quality checklists employed by DIMDI. These checklists consider the following aspects: selection process of intervention and control participants, allocation method, comparability of intervention groups, consideration of relevant confounders, blinding (single/double), comparability of circumstances beyond the intervention, validity of outcome assessment, attrition rate/differential attrition, description of statistical methods and intention to treat analysis.
Depending on the risk of bias, studies were subsequently rated as being of high (minimal risk of bias), good (moderate risk of bias), or fair (high risk of bias) methodological quality according to the grading system developed by the Scottish Intercollegiate Guidelines Network Review Group (SIGN).26 For all of the studies included in this review, data were extracted by one researcher and crosschecked by another. Disagreements between researchers in any matter related to the study selection process or data abstraction were resolved in discussion.
Interventions were classified as school-based, community-based or multisectorial, depending on the main components of the intervention. Any intervention performed outside the school environment was considered community-based; in turn, multisectorial interventions were defined as consisting of a school and an out-of-school component. To compare the effectiveness of the interventions, qualitative and quantitative synthesis of study results was performed and based, if possible, on studies with a small to moderate risk of bias. Our meta-analysis included studies only if these reported suitable prevalence data or effect measures. Odds ratios were calculated for dichotomous outcome measures. Pooled effects were subsequently estimated using a generic inverse variance method with random effects, as described in the Cochrane Handbook for Systematic Reviews.27 28 Pooled effect estimates were calculated for reported outcomes of lifetime, 30-day and regular smoking. To avoid double counting of individual studies, pooled estimates across these outcome categories were not calculated.
In the sensitivity analysis, we included fair-quality studies reporting suitable outcome data, excluded outliers and calculated pooled estimates using fixed effect models. In studies lacking suitable outcome data, it was attempted (whenever possible) to derive the number of smokers and non-smokers from the percentages given in these studies. To investigate the possibility of publication bias, a funnel plot diagram was constructed, including previously calculated effect estimates and standard errors of all identified studies and all suitable outcome measures.
RESULTS
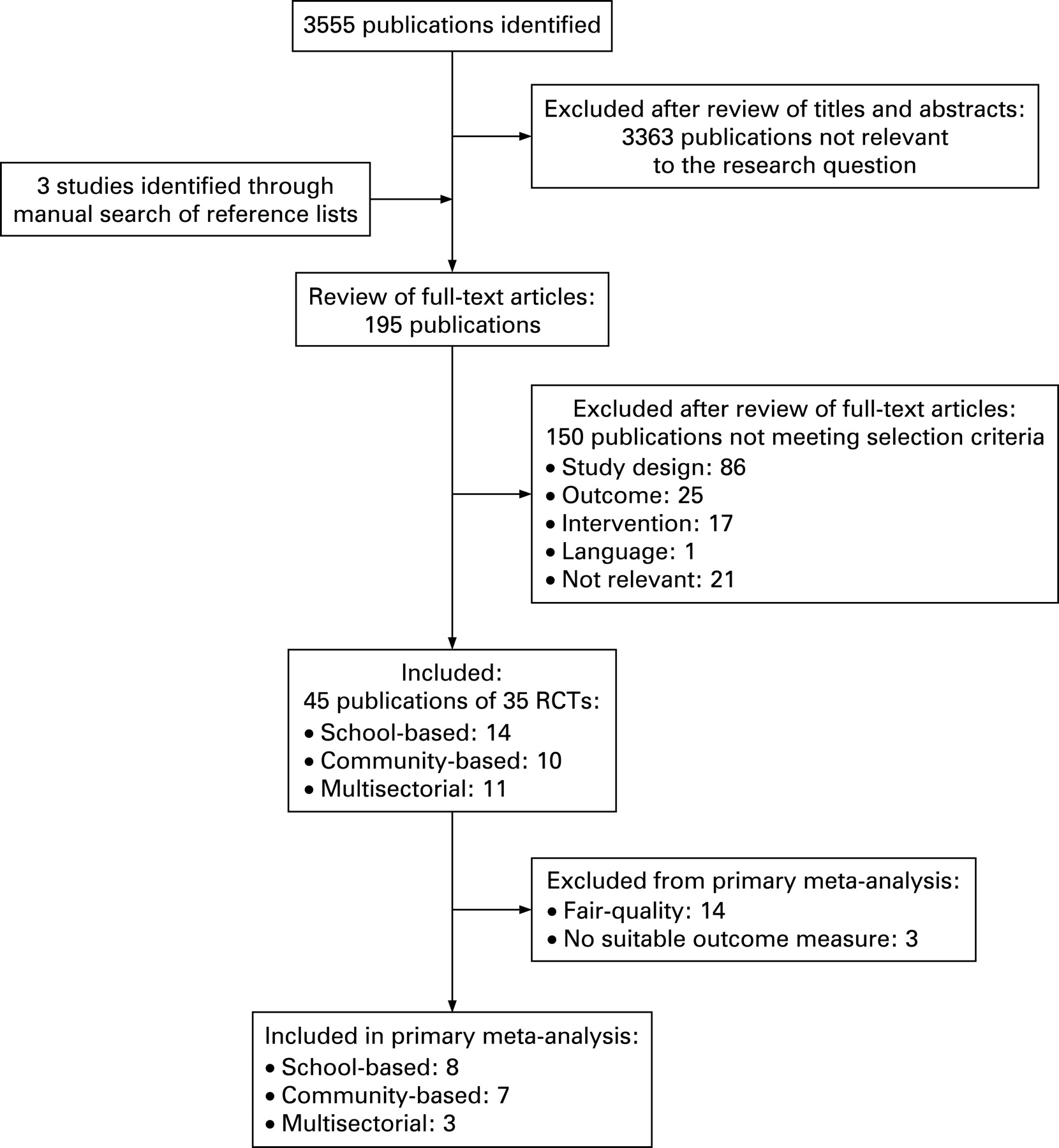
A total of 3555 publications were identified as part of a systematic search. Of these, 45 publications covering a total of 35 studies met the inclusion criteria (fig 1). The majority of studies were large and carefully conducted cluster randomised trials, which consisted of complex and resource intensive intervention strategies. It was therefore possible to rate more than half of these as being of good or high methodological quality. Reasons for limited methodological quality included inadequate descriptions of allocation methods; missing descriptions of baseline characteristics or of statistical analysis; and low follow-up rates. In addition, only a limited number of studies blinded participants or investigators to the intervention, validated outcome measures, or performed an intention-to-treat analysis. Follow-up duration ranged from 12 to 120 months.
The main study characteristics and individual study outcomes are presented in tables 1–3. Although the overall effectiveness of prevention programs showed considerable heterogeneity, the majority of studies reported at least some evidence of a positive intervention effect.
School-based interventions
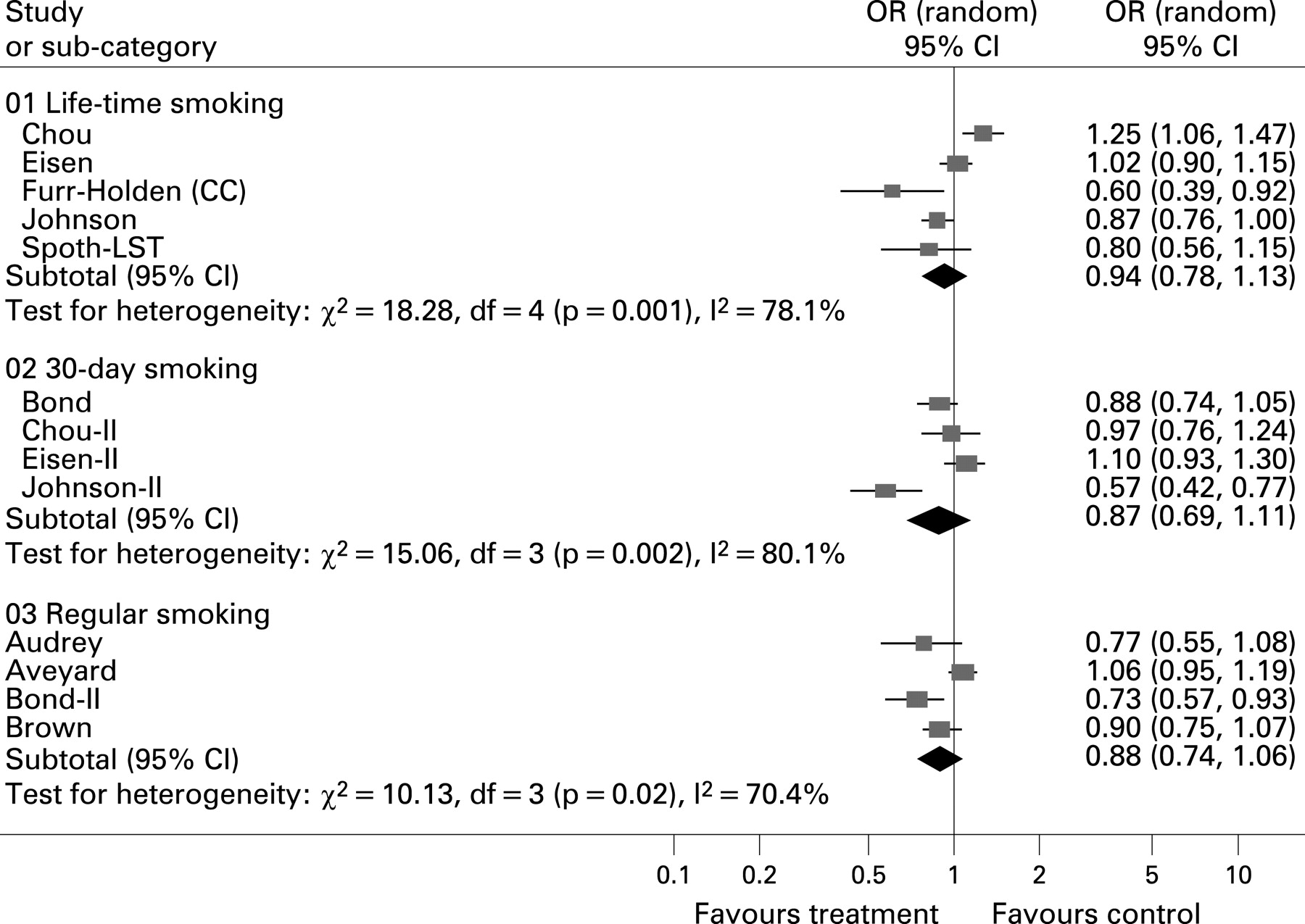
Among 14 randomised studies investigating school-based interventions, 9 were of good to high methodological quality. Of these, only Botvin et al29 and Johnson et al30 reported clearly positive intervention effects. In part, these effects were restricted to the culturally adapted intervention.30 The results of the seven remaining studies were inconclusive or even indicated that the intervention effects had been unfavourable.31–33 Differences in smoking rates between intervention groups varied considerably across studies, ranging from −3.8% (ie, favouring intervention groups) to 5.4% (ie, favouring control groups) (table 1). The results of our meta-analysis provide no evidence for the long-term effectiveness of school-based interventions (fig 2). These findings were similar for lifetime, 30-day and regular smoking. In our sensitivity analysis, the positive effects reached borderline significance when including fair-quality studies (table 4).
Community-based interventions
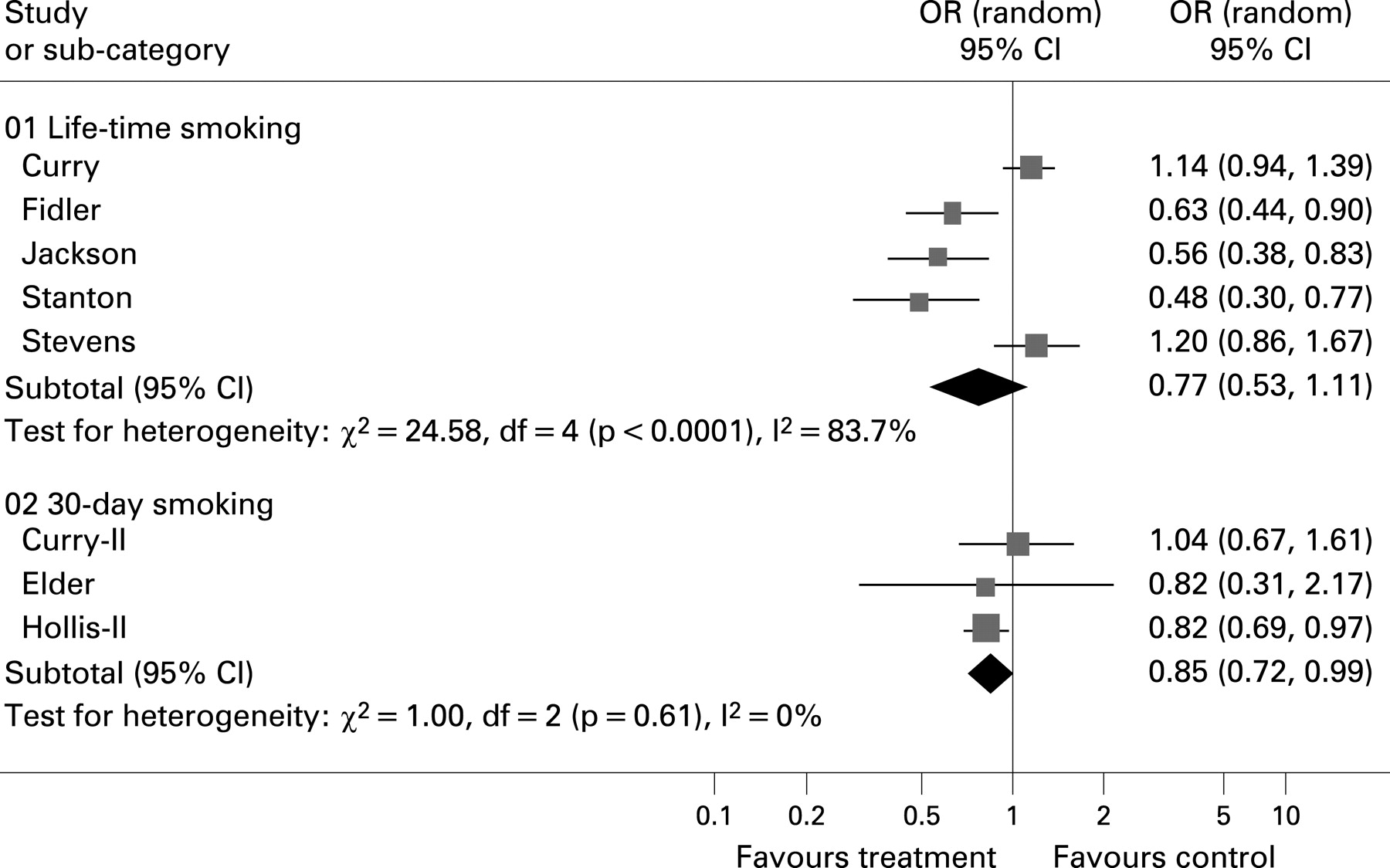
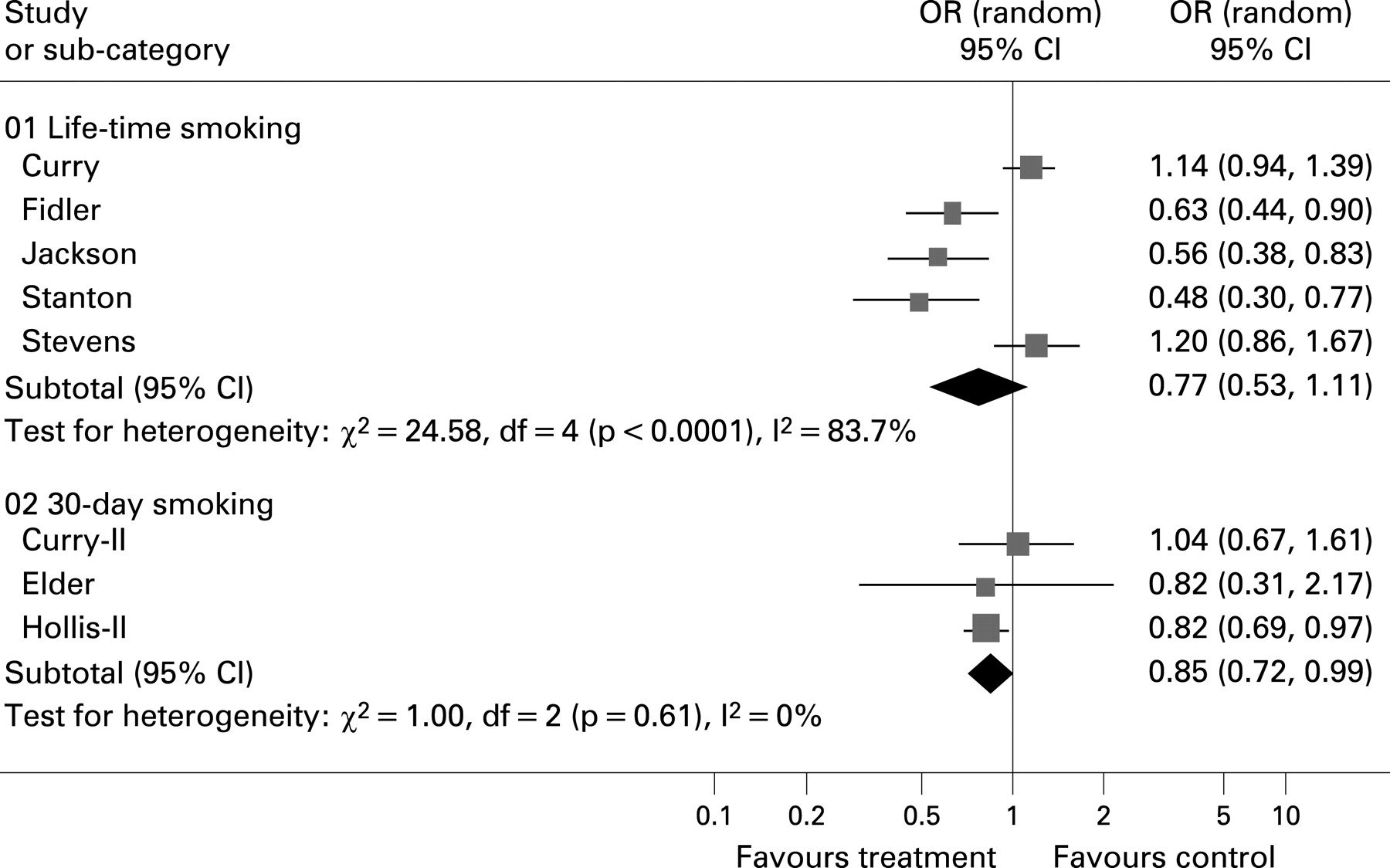
Among 10 studies investigating community-based interventions, 7 were of good to high methodological quality. Of these, Hollis et al,34 Jackson et al,35 Fidler et al36 and Stanton et al37 reported strong evidence of intervention effectiveness, as demonstrated by reductions in smoking rates of up to 10.6%. Conversely, Curry et al25 and Stevens et al38 reported a trend towards unfavourable intervention effects, reflecting an increase in smoking rates of up to 1.5% within the intervention group (table 2). Qualitative data synthesis was consistent with the results of our meta-analysis. Estimated pooled effects provided some evidence for the long-term effectiveness of community-based interventions (fig 3). The pooled effects were robust to sensitivity analysis, as presented in table 4.
Multisectorial interventions
Among 11 studies investigating multisectorial interventions, 6 were of good to high methodological quality. The studies by Ellickson et al,39 Furr-Holden et al,40 Reddy et al41 and Simons-Morten et al42 reported strong evidence of long-term effectiveness, and Perry et al43 and Spoth et al44 reported positive intervention effects for only some groups. One study reported different outcome measures for smoking behaviour, indicating similar intervention effects,39 and none of the studies identified found any association between the intervention strategies and unfavourable effects on smoking rates. The difference in smoking rates between intervention and control groups was as high as 6.1%, favouring the intervention group in all cases (table 3). A total of three studies did not report smoking prevalence or effect estimates as an outcome measure. Consequently, our meta-analysis was restricted to a limited number of studies. The results of the pooled effect estimates, however, provide strong evidence of the effectiveness of the intervention and were therefore consistent with the qualitative synthesis of data (fig 4). The estimated pooled effects were also robust to sensitivity analysis, being less strong only when studies with less reliable methodology were taken into consideration. The differences between intervention and control groups remained, however, statistically significant (table 4).

Few studies specifically tested different intervention strategies against each other. Spoth et al44 observed a greater reduction in smoking rates when school-based life skills training and an additional family-strengthening intervention were used. This difference did not reach statistical significance, however. Similarly, Perry et al43 observed substantial intervention effects associated with the DARE-Plus intervention compared to the DARE intervention, although only among boys. Conversely, Furr-Holden et al40 demonstrated that, compared to control, a classroom-centred intervention had greater intervention effects than did a family–school partnership; however, these two interventions were not formally tested against one another.
Intervention components
Few studies investigated the individual components of interventions. In the context of community-based and multisectorial programs, family interventions were frequently used. These pursued a variety of strategies, such as informing parents, improving parent–child communication, or strengthening the parent–school partnership. Whereas Stanton et al37 and Furr-Holden et al40 reported reductions in smoking rates associated with parental interventions, Schinke et al45 reported no additional benefits. Spoth et al44 also pointed to some additional effects for the family-strengthening intervention. The difference between intervention groups did not reach statistical significance, however. Although substantial reductions in smoking rates were also reported by Jackson et al,35 these investigators did not explore the additional effect beyond interventions focused on children. This all being said, only one study reported a trend towards unfavourable outcomes associated with family interventions.25 Although a number of additional studies that included family components also reported evidence of long-term effectiveness, it is impossible to distinguish the family component from the overall intervention effect.39 41–43 46 47
Only the study by Stanton et al37 examined the additional effectiveness of booster strategies to maintain intervention effects over time. They found no further reductions in smoking rates associated with this strategy. Nonetheless, with two exceptions33 47 several additional studies using booster strategies or continuing intervention sessions over the study duration reported reductions in smoking rates associated with the intervention.33 35 36 38–40 42 44 47 50 However, the effectiveness of these maintenance strategies was not examined specifically in any of these studies.
Three identified community-based studies investigated the effectiveness of primary care interventions compared to no-intervention control groups.34 36 38 The studies by Hollis et al34 and Fidler et al36 reported strong evidence of intervention effectiveness, whereas Stevens et al38 reported a trend towards an increase in smoking rates associated with the prevention program.
DISCUSSION
To our knowledge, the present work is the first to include and compare school-based, community-based and multisectorial behavioural interventions in the prevention of cigarette smoking among children and youth. As was expected, marked heterogeneity in intervention strategies, study methodology and intervention effectiveness were observed. Although reported effectiveness of investigated interventions varied between studies, the majority of studies provided at least some evidence for the effectiveness of behavioural interventions in the prevention of smoking. Frequently, studies reported different outcome measures of smoking behaviour. However, for the most part, the intervention effects appeared to remain consistent across these reported outcomes. With regard to different age groups, only two methodologically reliable studies targeted children between 5 and 10 years. These studies found strong evidence of intervention effectiveness. Whether this indicates that smoking prevention strategies have differential effects depending on age will require further investigation.35 40
When comparing different intervention strategies, the present review revealed the evidence for the effectiveness of school-based interventions to be inconclusive, whereas the evidence for the effectiveness of community-based and multisectorial interventions was somewhat stronger. These findings were consistent with the qualitative and quantitative synthesis of study results and were robust, for the most part, to sensitivity analysis.
The present review provides new insight into the debate about the long-term effectiveness of school-based interventions. Although a number of systematic reviews investigating this subject have concluded that school-based interventions can be effective in the long term,19 20 this review does not provide convincing support of these earlier findings. Although only recent school-based interventions were included in this review, clearly positive intervention effects were restricted to two studies.29 30 One of these took a culturally adapted approach and targeted a very specific population group,30 whereas the other29 presented results only as an aggregated outcome measure, thereby limiting comparability. The results of the remaining studies were inconclusive or even showed school-based interventions to be associated with increases in smoking rates. These findings were consistent with our meta-analysis, which was also unable to provide evidence for the effectiveness of school-based interventions. The findings of the present review thus confirm the conclusions drawn in a Cochrane review by Thomas et al,48 which did not find convincing evidence for the long-term effectiveness of school-based interventions. Whereas the conclusions of the Cochrane review were based, in large part, on one of the most sizeable studies investigating the social-influences approach in school-based smoking prevention (ie, the Hutchinson Smoking Prevention Trial), the present review included only recent school-based smoking-prevention strategies. Despite this focus on current prevention strategies, the outcome remained inconclusive.
With regard to the effectiveness of community-based and multisectorial interventions, the present review adds to previous research. Sowden et al23 identified 17 trials, 6 of which were randomised, in a review of community interventions. They reported positive intervention effects for only 2 out of 12 studies compared to a no-intervention control. The majority of studies included in their review investigated combinations of school-based and community-based interventions. Similarly, Thomas et al48 reported inconsistent evidence regarding the effectiveness of multisectorial interventions. By contrast, the majority of studies included in the present review, as well as the pooled effect estimates of studies investigating community-based and multisectorial interventions, found evidence of intervention effectiveness. While these findings indicate that evidence for the long-term effectiveness of community-based and multisectorial interventions is stronger and more consistent than has been shown in previous reviews, it has to be recognised that the study selection criteria and the classification of intervention strategies in the present review differed from those used in previous reviews.
The intervention effects reported for community-based and multisectorial strategies were not only more consistent than those observed for school-based strategies, they also resulted in a larger reduction in smoking rates. Indeed, whereas the greatest reduction in smoking rates among school-based strategies was only 3.6%, community-based and multisectorial interventions reported reductions of up to 10%.
Specific intervention components were investigated only infrequently. However, family-based interventions were used in many community-based and multisectorial intervention strategies. Although it was difficult to identify their specific impact, there seems to be some evidence for the additional effectiveness of this approach. In order to achieve reductions in smoking rates, however, it appears that providing smoking-related information to parents was not sufficient on its own, but rather that the family members needed to be actively involved. Activities targeted at parents who smoke were found to be especially effective. Further research will be necessary to confirm these results and investigate the additional reductions in smoking rates associated with this approach.
In the community, alternatives to family interventions are interventions in the primary health care sector. Although there is evidence that such interventions can effectively reduce smoking rates, the relative effectiveness compared to alternative interventions remains unclear and absolute effect sizes were only modest.
Further, one study found evidence that culturally adapting the approach and materials of an intervention to the needs of specific population groups was more effective than standardised strategies. It would thus seem advisable to pursue the former approach to bring about more substantial reductions in smoking rates in specific populations. However, further research will be necessary to confirm these findings and evaluate the cost-effectiveness of these more resource-intensive approaches.
What this paper adds
This study evaluates and compares the effectiveness of school-based, community-based and multisectorial behavioural smoking prevention strategies.
The review indicates that the evidence for the effectiveness of current school-based smoking prevention strategies alone is inconclusive and that there is more conclusive evidence for the effectiveness of community-based and multisectorial smoking prevention strategies.
However, even current and comprehensive behavioural smoking prevention programs are only associated with a moderate reduction in smoking prevalence and they should be complemented by appropriate environmental strategies to achieve sustainable reductions in smoking rates on a broad population basis.
This study further indicates, that there is currently a lack of studies investigating specific intervention components, which could help design more effective intervention strategies in the future. In addition, it should be noted that the growing complexity of current smoking prevention programs warrants high-quality cost-effectiveness studies.
The present review also attempted to determine whether the number of intervention sessions was associated with intervention effectiveness. Although the number of sessions varied greatly between minimal interventions and interventions with up to 40 sessions, the majority of studies used between 5 and 15 sessions. None of the studies investigated this issue specifically, however, and studies did not provide evidence that the number of intervention sessions was associated with intervention effectiveness. Similarly, identified studies only provided limited evidence, that booster strategies can improve long-term intervention effectiveness. However, one high-quality, minimal-intensity intervention25 showed a trend towards negative intervention effects, suggesting that a certain minimum amount of contact with participants might be necessary to achieve positive intervention effects.
When interpreting the outcomes of this systematic review and meta-analysis, several limitations should be kept in mind. Firstly, classifying interventions as school-based, community-based, or multisectorial is not unproblematic from a methodological perspective. As can be expected in the broad field of tobacco prevention, these three categories actually include a very diverse set of interventions. Nevertheless, because many of the most recent intervention strategies have drawn upon a variety of theoretical concepts, this approach was considered the most consistent means of classification. In recognition of the drawbacks to this approach, however, the attempt was made to identify specific components within the various interventions. Secondly, because only a minority of studies specifically investigated different smoking prevention programs, our comparison of school-based, community-based and multisectorial interventions is mainly based on an indirect approach. While the few studies that compared different intervention strategies provided some indication that multisectorial interventions were more effective, the differences between school-based and multisectorial interventions rarely achieved statistical significance.40 41 43 44 Thirdly, apart from the interventions, studies varied in a number of characteristics which could explain the varying degree of intervention effectiveness, such as country of study origin, methodological study quality, age and cultural background of participants. Also, control groups in community-based interventions were mainly described as “no-intervention controls”. However, standard prevention programs were continued in the majority of control groups in school-based and multisectorial interventions. This might explain some of the greater intervention effects identified for community-based interventions. Fourthly, calculated pooled effect estimates can be sensitive to the number of studies, availability of appropriate outcome measures, the choice of outcomes and other underlying assumptions. In the present review, however, the attempt was made to test for the validity of pooled estimates by performing appropriate sensitivity analyses. These indicated that estimated pooled effects were robust in the majority of cases. It should be noted, however, that pooled effects were frequently associated with high degrees of statistical heterogeneity and should be considered cautiously. Fifthly, the chosen time cut-off for study inclusion could possibly introduce bias. This approach was chosen, however, to put an emphasis on recent literature. Finally, despite the highly sensitive search strategy and exhaustive manual search of reference lists performed in the present review, publication bias is to be expected. The attempt was thus made to investigate publication bias by creating a funnel plot diagram of all included studies (fig 5). The diagram showed some asymmetry, with less precise studies being more likely to report favourable intervention effects. This indicates that publication bias is likely and that the results of the present review may overestimate the true long-term effectiveness of behavioural intervention strategies.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
This systematic review attempted to evaluate the long-term effectiveness of behavioural smoking prevention strategies. It should be pointed out, however, that long-term was defined as a minimum of 12 months. None of the methodologically reliable studies specifically followed adolescents until adulthood. Because smoking rates among youths increase rapidly up to early adulthood, the sustainability of intervention effects is unclear. Saying this, it should be pointed out, that included studies did not indicate decreasing intervention effectiveness with increasing length of study duration. In fact, with one exception38 all studies with a study duration greater than 36 months provided evidence of intervention effectiveness.35 38 40 42 45 46 50 62
In summary, the present review of behavioural interventions for smoking prevention provides moderate evidence for the long-term effectiveness of community-based and multisectorial interventions. For school-based interventions, however, the evidence of effectiveness was less convincing. Indeed, even in studies providing evidence of effectiveness, reductions in smoking rates were only modest. In view of the limited comparability of school-based, community-based and multisectorial strategies, however, it would not be justifiable to discard school-based prevention strategies altogether. On the contrary, it seems essential to facilitate the effectiveness of existing school-based prevention programs by supplementing them with community-based and family-based interventions. In addition, population-wide and environmental smoking prevention strategies should be continued and broadened to achieve meaningful and sustainable reductions in smoking rates among children and youth. There remains a great need for rigorous studies that investigate and identify the specific, effective components of various interventions. Moreover, due to the increasing complexity of recent interventions, high-quality cost-effectiveness analyses are also warranted to identify the most cost-effective ways to reach a wider population.
REFERENCES
Footnotes
Competing interests: None.
Funding: This systematic review was commissioned and funded by the German Institute of Medical Documentation and Information (DIMDI).