Article Text

Abstract
Although governments have imposed controls on tobacco company behaviour, they have not yet aligned tobacco industry goals to public health objectives. As a result, tobacco companies have delayed or diminished the impact of imposed public health measures and have not contributed to curbing the epidemic of tobacco use. Over the past decade, several regulatory innovations have been proposed as ways to better align industry actions with public health needs, but none have been put in place. These policy suggestions share the goal of providing a supply-side complement to conventional demand reduction strategies, but they differ in the assumptions they make and in the regulatory and governance approaches they take. Similarly, differing views on ideology and political context within the tobacco control community and between governments may hinder the establishment of a global consensus on the ideal supply-side intervention. A government willing to implement innovative supply-side strategies as part of a tobacco control endgame may not require such consensus if factors specific to their national public health systems or political contexts are supportive.
- End game
- Public policy
- Tobacco industry
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Introduction
If public health is to be the center piece of tobacco control—if our goal is to halt this manmade epidemic—the tobacco industry, as currently configured, needs to be dismantled.1
More than a decade has passed since David Kessler, former Commissioner of the US Food and Drug Administration, reflected on his failed attempt to regulate cigarettes and concluded that ‘small steps are not enough to curtail the power of the tobacco companies, or the damage they do’.1 Since then, no health authority has followed his advice and few in the public health community have encouraged them to do so. The public health consensus has instead been to acknowledge that it is not feasible to dismantle or otherwise change the system, but instead to work together to ‘patch it up and seek progress despite it’.2
Some of the ‘patching up’ efforts of this past decade have been truly impressive. Achievements like the Framework Convention on Tobacco Control (FCTC),3 and requirements for plain packaging,4 show that much can be done that does not require dismantling the industry. They have not, however, refuted Dr Kessler's conclusions that halting the epidemic will require a dismantling of the industry as currently configured.
The misalignment between the goals of public health authorities and the business mandate of the tobacco industry continues to drive industry efforts to delay, defeat or undermine tobacco control measures.2 ,5 The FCTC guidelines acknowledge that ‘there is a fundamental and irreconcilable conflict between the tobacco industry's interests and public health policy interests’.6 A desire to ‘resist the tobacco industry vector’7 and to plan an endgame for tobacco control8 may generate an interest in the fundamental changes to the tobacco industry by the public health authorities. If so, a range of preliminary suggestions is available for consideration. This paper summarises six such proposals and identifies factors that distinguish them from each other and from other endgame ideas.
Six proposals to overcome the tobacco industry
Over the past decade, this journal has published four suggestions on how to better align the motivation of those who supply tobacco products with public health goals. These include proposals for new structures through which tobacco products would be supplied,9 ,10 profit controls on the industry11 and legislated market outcomes.12 A fifth related proposal has been published elsewhere,13 as has a sixth suggestion to abolish commercial tobacco sales.14
The first of these approaches, and arguably the groundwork for subsequent work on structural reform of tobacco supply, is the ‘Regulated Market Model’ (RMM) suggested by Ron Borland in 2003. He suggests the transfer of the marketing and distribution functions of tobacco suppliers to a monopoly that has a mandate to ‘service the existing market, but shape it to minimise harm’. This new agency would operate as a link in the supply chain between free-market tobacco manufacturers and retail outlets. It would use both new regulatory and purchasing–selling powers to exercise authority over those who make cigarettes and those who sell them. It does not set out to dismantle the industry so much as to ‘create a context whereby the forces of competition could be marshalled in the interests of reducing the harmfulness of tobacco products’.10
The second is our 2005 suggestion for the establishment of a ‘non-profit enterprise with public health mandate’ (NPE), which would remove profit-making from the entire tobacco supply system and replace duty to shareholders with an unencumbered responsibility to meet the public health goal of phasing out smoking. This model seeks to transform the market rather than to regulate it and would do so by changing the economic and legal conditions under which tobacco companies operate. In this analysis, a key source of the tobacco epidemic ‘lies in the political choice to allow business corporations to supply cigarettes’.9 ,15
A third proposal, offered in 2005 by Stephen Sugarman16 and described by him more fully in 2009, would redirect the efforts of tobacco companies without creating new administrative structures and without dismantling it, per se. He suggests that the use of performance-based regulations (PBRs) ‘attacks the issue in an altogether different way. It rests on the simple proposition that the tobacco companies themselves should be required to achieve sharply improved public health outcomes’. He suggests that this can be done through the imposition of legal requirements on tobacco companies to reduce the number of people who smoke their products and to impose effective financial penalties on those who fail to do so.13 ,16 A law illustrating such an approach was proposed in US Senate.17
A fourth suggestion was made in 2010 by Anna Gilmore et al11 and involves the creation of an independent regulatory agency, the Office for Smoked Tobacco Regulation (OFSMOKE). This agency would seek to correct the market failure, resulting from an oligopolistic cigarette market and to reduce the market power of tobacco manufacturers. It would do this primarily by imposing price controls at the manufacturers’ level, reducing the financial returns to suppliers. Under this model, the underlying structure of the tobacco market with respect to industry motivation and health regulation would not be changed.
A fifth suggestion, with elements common to Sugarman's, is the ‘Sinking Lid’ proposal made in 2010 by George Thomson et al12. It seeks to end tobacco use through the imposition of progressive limits on the amount of commercial tobacco released for legal sale, and the use of auction to license suppliers for the remaining portion. Using a biannual reduction of 5% of the initial volume, the authors foresee a phasing out of commercial tobacco within two decades. The capped market would be complemented by and would facilitate the expansion of demand-side measures, like plain packaging and increased consumer prices, but would be the ‘key overarching mechanism’ to prompt changed behaviour by suppliers.12
A sixth proposal is Robert Proctor's appeal for ‘Abolition’ of commercial tobacco. He proposes to ban the sale and manufacture of cigarettes, and to permit the smokers to grow their own tobacco. Instead of seeking to better regulate the market, transform it or impose performance requirements on it, Proctor seeks to collapse the organised supply. ‘This is the simplest way to approach disease prevention and would obviate the need for most other solutions commonly proposed’.14
Two dimensions of difference
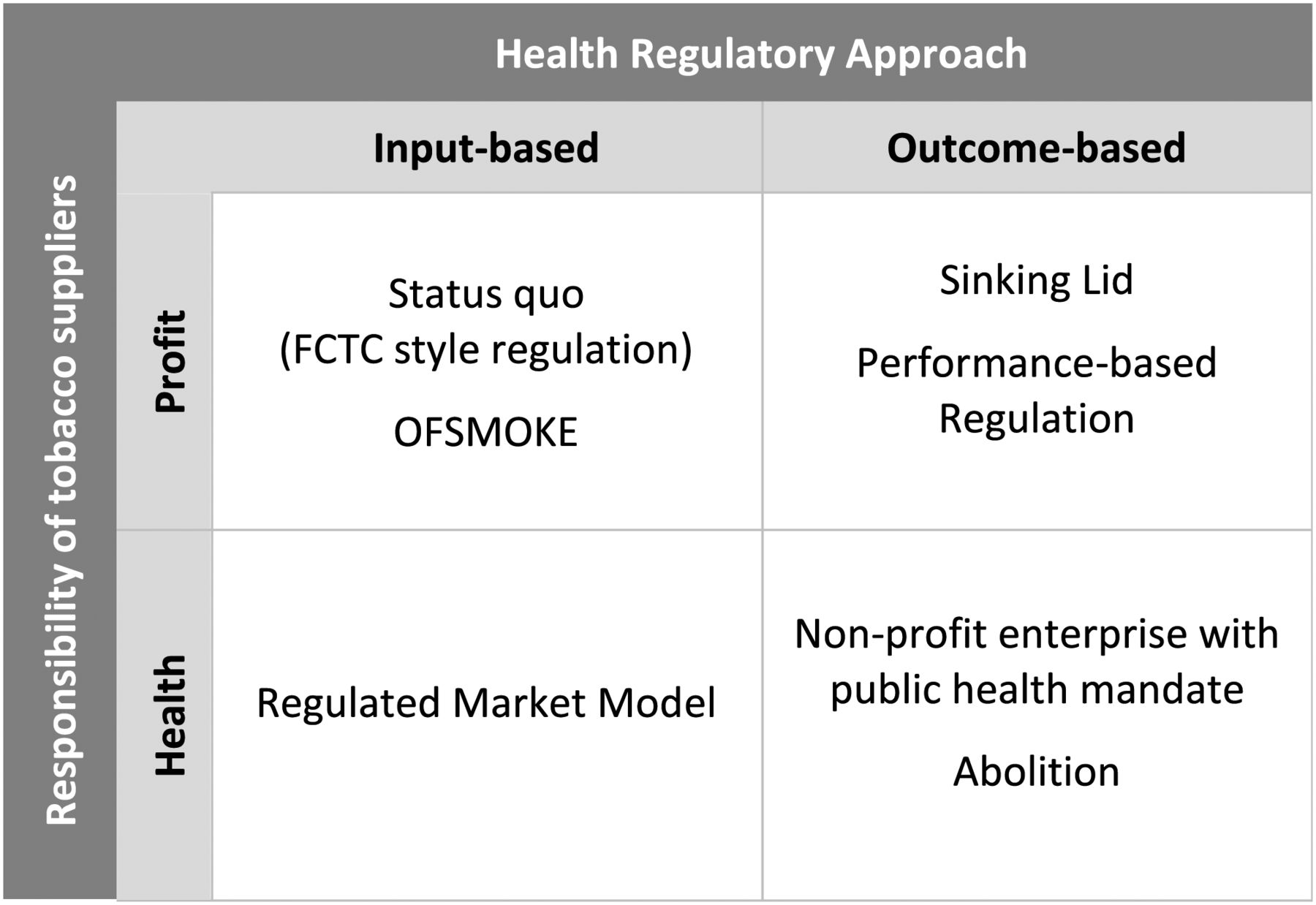
These six models exhibit a number of conceptual differences. Although they mostly share a core rationale (the ‘why’), the proposed legal changes (the ‘how’) differ on at least two dimensions (Figure 1).
One difference is whether those who supply tobacco should be held accountable primarily for their achievement of financial or health goals. The OFSMOKE, Sinking Lid and PBRs would all retain tobacco suppliers as they are currently configured, including their obligations to the best interests of their shareholders. The RMM would impose a health-oriented intermediary in the tobacco supply system, which would be oriented towards health goals, but much of the supply system would rely on ‘free enterprise’ and competition for financial rewards. The NPE and Abolition approaches are conceptualised on removing tobacco supply from the profit sector.
The other dimension on which these proposals differ is the regulatory approach, either in favour of input-based requirements (which codify organisational behaviour) or outcome-based requirements (which codify objectives). Input-based strategies, ‘ordinarily assume that if enterprises make the ordered behavioural changes, then improved public health performances will follow’.13 In such regulatory systems, tobacco suppliers are responsible for adhering to the regulations, but not for the achievement of the goals of those regulations. By contrast, an outcome-based approach would put responsibility on tobacco suppliers to meet the regulatory objectives, such as a reduction in overall tobacco use. Current tobacco control strategies include both input-based regulations, such as advertising bans, and outcome-based regulations, such as ceilings on tar emissions.
Two of the proposed models are predominantly input based. OFSMOKE would impose a price ceiling in the expectation that this would improve public health, but would not make tobacco suppliers responsible for any such outcomes. The RMM expects a ‘more dynamic and trusting relationship with manufacturers’, but is described in ways that imply the continued use of behavioural regulation.10
The other four proposed approaches are focused on outcome-based improvements to tobacco control. The Sinking Lid and Performance-Based Regulations use performance outcomes as their organising principle, the NPE approach seeks to overcome the failures of input-based regulations by mandating and empowering tobacco suppliers towards health goals and the Abolition approach moves immediately to the performance end point .

{kind=link}
Conceptual differences in proposed tobacco supply models.
Conceptual differences in proposed tobacco supply models
Related but distinct proposals
The ideas summarised earlier are qualitatively different from the proposals to prohibit the sale of some or all categories of tobacco products, such as those made by Hall and West18 and Daynard.19 Under their approach, the sale of less harmful forms of nicotine would be permitted and the industry would not be dismantled. The converse situation currently exists in Australia, where there is a ban on the sale of smokeless tobacco, but combustible cigarette sales are permitted.20
Other proposals to curtail the legal right of the individuals to smoke tobacco products21 ,22 have the effect of prohibition. They seek, however, to modify the behaviour of consumers and not the producers. As demand-side interventions they are qualitatively different concepts from the ideas summarised earlier which focus on changing the behaviour of producers.
Discussion
Governments have made choices about the way tobacco companies are governed and the rights and obligations imposed on them. In most developed countries, these obligations include the responsibility to maximise financial returns to shareholders and to be accountable only to shareholders and the legal rights, including those given to real human beings (such as the right to freedom of expression) and beyond human reach (such as immortality).8 Even when these companies are owned or effectively controlled by government, such as in China and Japan, the choice has been to direct these companies towards monetary and not towards health objectives. From a public health perspective, these choices are not optimal and reflect incoherence or incompleteness in health policy.
Like governments, tobacco control advocates have also made choices about the tobacco supply models that they are willing to support or oppose. At the moment, many have chosen to oppose supply-side change partially because of ‘the animosity that influential sections of the movement have exhibited towards these efforts’.2 The research community has similarly voted with its feet to focus on smokers and cigarettes, but not on the industrial vector of disease.23 The policy consensus reflected in the international standard setting for demand reduction measures under the FCTC24 has not yet emerged for supply-side endgame policies.8 ,25
Even among those proposing supply-side change, there are obvious differences in political philosophy or assessment of policy context. For instance, Borland considers that ‘regulation needs to be compatible with the free enterprise system’,10 which contrasts with our assessment that ‘industry obligations to their owners’ will inherently undermine health goals.9 We consider it likely because expropriating the industry is a good public health investment,26 but Gilmore et al11 think it ‘impractical’ to consider this option. Sugarman13 thinks those ‘who think firms are more nimble than regulators as well as those who want firms to take more responsibility’ will find his proposal has ‘political cachet’, and Thomson et al12 find local public support for ‘relatively simple to communicate’ proposals.12
It is possible that agreement on how best to supply tobacco will not emerge among nations or within the public health community just as it has not emerged for the supply of other goods and services. Around the world, governments have chosen to supply healthcare services, educational facilities, alcohol supply, water, sanitation, communications and transportation under very different systems of control and with differing blends of private and public sector involvement.
The importance of local conditions to government policy on commerce may mean that global consensus on tobacco supply is not possible, needed or even desirable. Differing national political economies (the ‘where’) offer differing opportunities and constraints. In France, for example, where tobacco retailing is under state monopoly control and where corporations are prohibited from being licensed to sell tobacco,27 it may be administratively easier to adopt Ron Borland's RMM than a system where there are existing licensees to expropriate.
Policy contexts shift over time and may create new windows of opportunity (the ‘when’). The ideological orientation of governments28 and the views of ‘bureaucrats, politicians and professionals’ within regulatory systems29 influence tobacco control decisions but are mutable. Crisis provokes change. Litigation against tobacco companies, for example, may create ‘a tipping point, when the problems faced by an industry become potentially unmanageable, raising questions about its continued existence’.5 If shares in tobacco companies become ‘declining assets’ as a result of falling revenues from tobacco sales, then shifts in ownership structure30 may provoke or facilitate policy change.
Based on the previous experience, the industry can be expected to forcibly resist measures that will reduce their profits, including all of the suggestions reviewed earlier. The political will required to overcome industry attempts to defeat such measures may require active support from civil society and health researchers. Fortunately, our understanding of past tobacco industry behaviour1 ,9 ,14 can help guide strategies to neutralise tobacco industry interference to such policies.
Health authorities who wish to follow Dr Kessler's advice now have several conceptual approaches to draw on and the generation of new ideas can be anticipated. The search for endgame measures may present a moment when changing tobacco supply can be included as a policy option.
Acknowledgments
Appreciation to Ken Warner for convening a meeting on endgame ideas, at which these and other ideas were discussed, and to those supporting the development of endgame and other policy innovations.
References
Footnotes
-
Contributors The ideas were jointly developed by CDC and NEC and CDC put pen to paper.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Open Access This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/