Article Text

Abstract
Objective The aim of this research was to compare the risk of all-cause mortality and mortality from all cancers combined, lung cancer, respiratory diseases, cardiovascular diseases and diabetes mellitus between normal-weight smokers and overweight or obese ex-smokers.
Methods Data were from 1997 to 2004 National Health Interview Survey (with response rates ranging from 70% to 80%) which were linked to records in the National Death Index. Mortality follow-up was through 31 December 2006. The sample was limited to normal-weight smokers and overweight/obese ex-smokers 25 years of age and older (n=52 819). HR from Cox regression was computed to represent mortality effect.
Results Results showed that in both women and men, normal-weight smokers, relative to overweight or obese ex-smokers, had a higher risk of mortality from all causes combined, all cancers combined, lung cancer, cardiovascular and respiratory diseases. Among women, there was no difference in mortality risk from diabetes mellitus between normal-weight smokers and overweight or obese ex-smokers. Among men, there was some evidence that the risk of mortality was higher in obese ex-smokers than normal-weight smokers.
Conclusions This article concludes that, overall, mortality risk is smaller in overweight or obese ex-smokers than normal-weight smokers. Smoking cessation interventions can tailor messages that highlight the greater reduction in mortality associated with quitting, compared with potential weight gain.
- Smoking Caused Disease
- Prevention
- Priority/special populations
Statistics from Altmetric.com
Introduction
Each year in the USA, smoking causes over 443 000 deaths, primarily from cancer and cardiovascular and respiratory diseases.1 There is also mounting evidence that smoking increases the risk of and mortality from diabetes mellitus.2 ,3 Fortunately, smoking cessation reduces risk of disease4 and mortality from lung cancer, respiratory and cardiovascular diseases.5–9 However, smoking cessation is associated with weight gain.10–13 On average, smokers tend to weigh less than non-smokers12 ,14 and the majority of quitters gain about 3–9 kg within 8 years of quitting,15 ,16 and between 10% and 13% of quitters gain at least 11 kg.11 Most of this weight gain occurs within 3 months of abstinence.17 Only a quarter of smokers maintain a healthy weight after quitting smoking.15 Consequently, postcessation weight gain is commonly cited, especially among women, as the main reason for not trying to quit.18 Similarly, about half of the smokers who have tried to quit but failed report that weight gain was the reason for their relapse.14
Weight gain also puts ex-smokers at risk of diseases that are caused by overweight and obesity. Overweight (defined as body mass index (BMI) of 25–29.9 kg/m2) and obesity (defined as BMI of greater than or equal to 30 kg/m2) are associated with higher risk of mortality from diabetes mellitus, various types of cancer, cardiovascular disease and respiratory diseases.19–23 Thus, the weight gain that results from smoking cessation may increase the risk of some of the same diseases whose risks are reduced by smoking cessation. This raises the question of which is least detrimental to health: to remain a normal-weight smoker or to quit smoking and possibly become an overweight/obese ex-smoker? In a study that examined the combined effect of smoking and BMI on all-cause mortality among older adults, Koster et al24 found that the risk of mortality is higher in normal-weight smokers than overweight or obese ex-smokers. However, in a study of radiological technologists, Freedman et al25 did not find any difference in all-cause, cancer or cardiovascular disease mortality between normal-weight smokers and overweight or obese ex-smokers. To our knowledge, there are no studies based on a nationally representative sample that examine how the risk of morality from all causes combined as well as specific causes is different between normal-weight smokers and overweight/obese ex-smokers. Our aim was to compare the risk of all-cause mortality and mortality from all cancers combined, lung cancer, respiratory diseases, cardiovascular diseases, and diabetes mellitus between normal-weight smokers and overweight/obese ex-smokers using data from the 1997 to 2004 National Health Interview Survey (NHIS) which has been linked to the National Death Index (NDI).
Methods
Data
We employed public use data from the NHIS files for the years 1997–2004 and the corresponding files with the linkage of NHIS and NDI provided by the National Center for Health Statistics (NCHS).26 The NHIS is conducted annually, uses a multistage probability sampling design and is representative of the civilian non-institutional population of the USA. The annual response rate in the years 1997–2004 ranged between 70% and 80%. All data are based on self-reports, including height, weight and smoking status information, and obtained via inhome interviews. Substantive and methodological details of the NHIS are described elsewhere.26 The NCHS has linked the survey participants for the years 1986–2004 to death certificate data from the NDI with follow-ups through 31 December 2006. Mortality ascertainment is based on a probabilistic matching algorithm that links the NHIS and NDI records by an individual's social security number, name and other demographic variables.27 We limited the analysis to individuals who were aged 25 years and older and were either normal-weight smokers or overweight/obese ex-smokers, as defined below, at the time of the interview. The reason we have not included individuals under the age of 25 years is that there were too few deaths among this age group. For example, there were no deaths from lung cancer, respiratory diseases, cardiovascular diseases or diabetes mellitus among men in this age group.
Measurement
The outcomes were all-cause mortality, and morality from all cancers combined, lung cancer, respiratory diseases including chronic obstructive pulmonary disease (COPD), cardiovascular diseases and diabetes mellitus. The causes of death were coded according to the tenth revision of International Classification of Diseases (ICD-10).28 ICD-10 codes for the study outcomes are as follows: all cancers, C00-D48; lung cancer, C33-C34; respiratory disease/COPD, J00-J99; cardiovascular diseases I00-I99; and diabetes mellitus, E10-E14. Follow-up time for individuals who died was measured in number of months from the month/year of the interview to the month/year of death. Because quarter instead of month of death was available, we made the assumption that death occurred in the middle of the recorded quarter, that is, February, May, August or November.
The predictor of interest was normal-weight smoker versus overweight or obese ex-smoker. BMI was computed as the ratio of self-reported weight in kilograms divided by the square of self-reported height in metres. A BMI of greater than or equal to 18.5 and smaller than 25 kg/m2 was considered normal weight; a BMI of equal to or higher than 25 and smaller than 30 kg/m2 was considered overweight; and a BMI of greater than or equal to 30 kg/m2 was considered obese. Smokers who were underweight (BMI <18.5 kg/m2) were excluded from the sample.
Respondents were asked ‘Have you smoked at least 100 cigarettes in your entire life?’ Those who replied affirmatively were then asked ‘Do you now smoke cigarettes every day, some days or not at all?’ Based on these questions, we defined smokers as those who have smoked at least 100 cigarettes in their life and currently smoked every day or some days, and ex-smokers as those who have smoked more than a 100 cigarettes in their life but do not currently smoke. Never-smokers, that is, those who have not smoked more than a 100 cigarettes in their life, were excluded from the analysis.
The sociodemographic predictors in the analyses were as follows: age, grouped into 25–44, 45–64 and 65+ years; marital status, grouped into married, separated/divorced, widowed and single; race/ethnicity, categorised as non-Hispanic white, non-Hispanic black, Hispanic and other; nativity, distinguishing those born in a US state or District of Colombia from others; educational attainment, grouped into 0–11, 12, 13–15 and ≥16 years; family poverty status, measured as the ratio of total family income from all sources before taxes to the poverty threshold for each survey year; homeownership, distinguishing homeowners/purchasers from renters; and region of residence, grouped into Northeast, Midwest, South and West.
Statistical analyses
The data for all the survey years, that is, 1997–2004, along with information about mortality outcomes were pooled into one dataset. We computed age-standardised mortality rates per 100 000 person years by sex among normal-weight smokers and overweight/obese ex-smokers for all-cause mortality and each of the specific causes of death that are the focus of the study. We used the direct method of age-standardisation based on the age distribution of the 2000 US Standard Population and employing the age categories 25–44, 45–64 and 65+.29
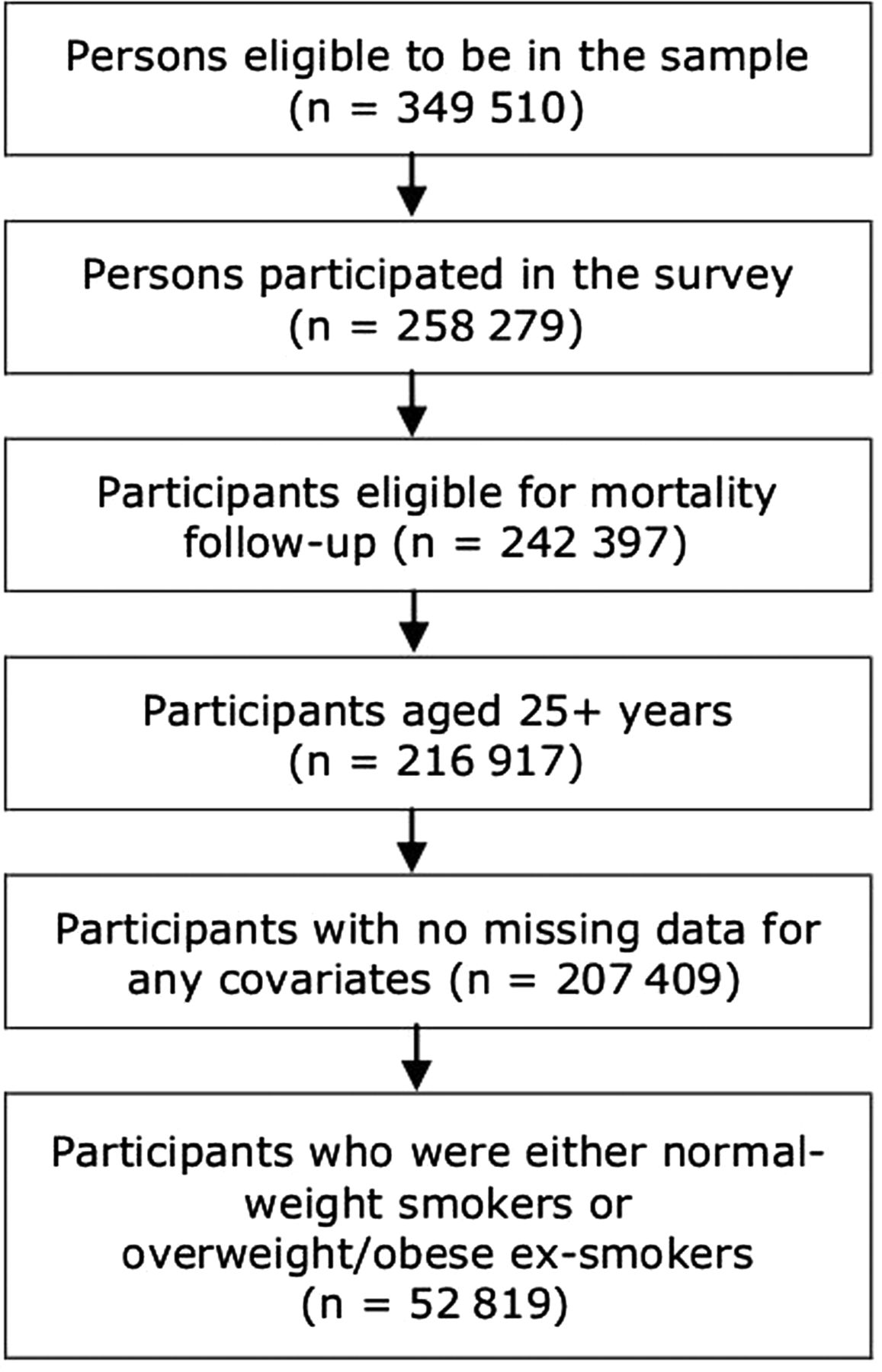
Cox proportional hazards regression was used to model time to death as a function of normal-weight smoker versus overweight/obese ex-smoker and sociodemographic predictors. We constructed survival curves based on covariate-adjusted regression results. In the analysis for a given cause of death, individuals who did not die of that cause as well as those surviving at the end of the follow-up were right-censored. Because we found strong evidence (p<0.001) of an interaction between sex and normal-weight smoker versus overweight/obese ex-smoker, we stratified the regression models by sex. In all analyses, we adjusted for the complex sampling design of the NHIS by taking into account sampling weights provided in the NHIS–NDI linked mortality files, stratification and primary sampling units in computations. We adjusted the sampling weights by dividing them by 8, the number of survey years used in the analysis.26 In addition, although our sample is restricted to the subpopulation of normal-weight smokers and overweight/obese ex-smokers, we have taken into account the full complex design of the sample in computing SEs. Thus, information on all clusters and strata, which is necessary for correct variance estimation, was included in the computations. Cases with missing values for any of the study variables (ie, 0.8% of the sample), except poverty status, were excluded from the analysis. Missing values for poverty status (18.9%) were included as a distinct category. In addition, cases with insufficient data for linking NHIS and NDI records (6.2%) were not included in the analysis. The final sample size for the analysis was 52 819 (see figure 1). Stata SE V.12 was used in all analyses.30

Flow diagram describing the final analysis sample size.
Results
In the pooled sample of individuals 25 years of age and older, 9.3% were normal-weight smokers with an average BMI of 22.3 kg/m2, 9.6% were overweight ex-smokers with an average BMI of 27.3 kg/m2 and 6.3% were obese ex-smokers with an average BMI of 34.6 kg/m2. Table 1 shows the distribution of sociodemographic variables by sex among normal-weight smokers, overweight ex-smokers and obese ex-smokers. Among both men and women, normal-weight smokers were more likely than overweight/obese ex-smokers to be younger, unmarried, less educated, impoverished and to live in rented housing (p<0.001 for all associations). Among both women and men, obese ex-smokers were more likely to be native to the USA than normal-weight smokers or overweight ex-smokers (p=0.004 in women and p<0.001 in men).
Table 2 shows the number of deaths and age-adjusted mortality rates per 100 000 person-years by subgroup. The total number of deaths was 5135. All mortality rates were substantially larger in normal-weight smokers than overweight or obese ex-smokers, except in the case of diabetes mellitus where there was little evidence to suggest a difference in the mortality rates. Among women, the overall age-adjusted mortality rate for normal-weight smokers was 1668 (95% CI 1552 to 1783), for overweight ex-smokers was 1093 (95% CI 1009 to 1179) and for obese ex-smokers was 1222 (95% CI 1118 to 1327) per 100 000 person-years. Similarly, among men, the overall age-adjusted mortality rate for normal-weight smokers was 2809 (95% CI 2627 to 2991), for overweight ex-smokers the rate was 1346 (95% CI 1274 to 1417) and for obese ex-smokers the rate was 1523 (95% CI 1411 to 1634) per 100 000 person-years.
Tables 3 and 4 present age-adjusted and covariate-adjusted HRs for normal-weight smokers relative to overweight and obese ex-smokers from Cox proportional hazards regression models for women and men, respectively. Among women, the overall mortality risk was 26% lower in overweight and obese ex-smokers than normal-weight smokers (p<0.001). Among women, compared with normal-weight smokers, the risk of mortality from all cancers combined was 29% and 46% lower in overweight and obese ex-smokers, respectively (p<0.001). A similar pattern of risk difference existed in the case of lung cancer (59% and 79%, p<0.001), respiratory diseases (44% and 36%, p<0.001) and cardiovascular diseases (26% and 21%, p=0.013). Among men, compared with normal-weight smokers, the overall mortality risk was 41% and 37% lower in overweight and obese ex-smokers, respectively (p<0.001). A similar pattern of risk difference existed in the case of all cancers combined (31% and 33%, p<0.001), lung cancer (70% and 75%, p<0.001), respiratory diseases (65% and 65%, p<0.001) and cardiovascular diseases (25% and 15%, p=0.009). Compared with normal-weight smokers, the risk of mortality from diabetes mellitus was 4% and 98% higher in overweight and obese ex-smokers, respectively (p=0.011). We note that the observed effects on mortality were stronger for men than women, except in the case of mortality from cardiovascular diseases. We also note that we examined the change in the coefficients and their SEs in the main predictor, normal-weight smoker versus overweight ex-smoker versus obese ex-smoker, before and after other covariates were added to the models. We have found no evidence of a drastic change to suggest multicollinearity is a problem in the current analysis.
Weighted sample characteristics (%) by sex among normal-weight smokers and overweight ex-smokers and obese ex-smokers (n=52 819)
Figures 2 and 3 show survival curves for each cause of death for women and men, respectively. Consistent with the findings presented above, these curves clearly indicate a survival advantage for overweight and obese ex-smokers for all-cause mortality and mortality from selected causes. The survival curves for diabetes mellitus among women are not shown, as the regression results did not indicate a mortality difference between normal-weight smokers and overweight or obese ex-smokers.

Survival curves for women by cause of death. COPD, chronic obstructive pulmonary disease.

{kind=link}
{kind=link}
{kind=link}
Survival curves for men by cause of death. COPD, chronic obstructive pulmonary disease.
In supplementary analyses not shown, we found that the covariate-adjusted risk of mortality from all causes combined and from specific causes (except diabetes mellitus) was greater in normal-weight smokers than overweight never-smokers or obese never-smokers. There was no difference in risk of mortality from diabetes mellitus. In additional supplementary analyses for each specific disease, we excluded the baseline respondents who had indicated they had been diagnosed with that disease. The only notable difference from the results reported above was that there was no effect of the exposure on mortality from diabetes mellitus among men.
Discussion
This nationally representative study provided strong evidence that the risk of mortality from all causes combined, all cancers combined, lung cancer, respiratory diseases and cardiovascular diseases is higher in normal-weight smokers than overweight/obese ex-smokers. It is important to note that the magnitude of this increased risk was larger among men than women for all-cause mortality and mortality from all cancers combined, lung cancer and respiratory disease. In contrast, the magnitude of the increased risk was larger among women in the case of mortality from cardiovascular diseases.
Our finding that normal-weight smokers had a higher risk of all-cause mortality than overweight/obese ex-smokers was in accordance with the report of Koster et al24 on older adults. However, our findings in relation to cause-specific mortality were not consistent with the results of Freedman et al25 that among radiological technologists being a normal-weight smoker versus an overweight/obese ex-smoker does not affect the risk of mortality from cancer or cardiovascular disease. The inconsistency may be due to the Freedman et al sample which was limited to one occupational group, was over 90% white, and thus did not represent the general population.
We found that among men, there is some evidence that the risk of mortality from diabetes mellitus is higher in overweight or obese ex-smokers than normal-weight smokers. However, such an effect was not observed among women. Previous studies have shown that while smoking cessation is associated with a higher risk of diabetes,3 ,31 ,32 the increased risk diminishes with time and disappears after 12 years.3 Furthermore, a prospective study with a follow-up of 8.5 years found that there was an increased risk of diabetes associated with quitting among those women who gained at least 5 kg.33
A major strength of our study was the use of a large, nationally representative sample with high response rates and a data collection based on inperson home interviews. The mortality rates presented in table 2 are reasonably valid as the NHIS–NDI based mortality rates for the general population aged 25+ years compare well with those derived from the national vital statistics mortality rates for the period 1997–2004. For example, in the NHIS–NDI database, the age-adjusted all-cause mortality rate was 1690 per 100 000 population in men and 1200 per 100 000 population in women; the corresponding age-adjusted vital statistics based mortality rates were 1560 in men and 1076 in women.29
Number of deaths and age-adjusted mortality rates per 100 000 person years and 95% CIs by sex among normal-weight smokers and overweight and obese ex-smokers (n=52 819)
Age-adjusted and covariate-adjusted* HRs for overweight and obese smokers relative to normal-weight smokers by cause of death among women (n=24 324)
Age-adjusted and covariate-adjusted* HRs for overweight and obese smokers relative to normal-weight smokers by cause of death among men (n=28 495)
Our study had some possible limitations. We were unable to assess changes in smoking or overweight or obesity status during the follow-up period; thus, the exposure was assumed to be time-invariant. Similarly, we did not have information on duration of abstinence from smoking. Furthermore, smoking status, height and weight were self-reported and not based on objective measurement. However, self-reported smoking status in surveys of the general population has been validated with cotinine34 and the amount of misclassification (ie, proportion of self-reported non-smokers with increased cotinine levels indicative of active smoking) is very low (eg, 0.9%35 and 1.4%36) in most community based studies.37 People who are overweight or obese are more likely than others to underestimate their weight and overestimate their height.38 This suggests that the group of overweight/obese ex-smokers in our study was possibly larger than we estimated and we did not include some ex-smokers at the lower end of the overweight/obesity continuum. This might have resulted in a slight overestimation of the effects reported in this study.
Another limitation of the study was that we were unable to use graded obesity classes as defined by WHO: class I (BMI ≥30.0 and <35), class II (BMI ≥35.0 and <40) and class III (BMI ≥40.0).39 This was because the number of deaths from lung cancer, respiratory diseases and diabetes mellitus were too few among individuals who were classified as class I (5% of the sample) or II (3% of the sample) obese.
Our study suggests that although smoking cessation may result in overweight or obesity, this risk does not outweigh the benefits of smoking cessation in terms of reductions in mortality risks. Smoking cessation interventions can use this information to tailor their messages to negate the fear of weight gain that may be associated with quitting smoking. These interventions should especially target women, given that they present weight gain as a major barrier to smoking cessation.18 In addition, further research on how smoking cessation interventions can best be paired with weigh gain prevention is warranted.40 Healthcare providers, health promotion programmes and public health professionals should advise their clients who smoke that even if they gain weight because of quitting, it is still a healthier option than continuing to smoke.
What this paper adds
-
Our study used a large, nationally representative sample with high response rates to find that although smoking cessation may result in overweight or obesity, this risk does not outweigh the benefits of smoking cessation in terms of reductions in mortality risks.
-
This information can be used by healthcare providers, health promotion programmes and public health professionals to plan and administer effective smoking cessation interventions.
-
This knowledge could be used to tailor the smoking cessation messages to negate the fear of weight gain that may be associated with quitting smoking, especially among women.
References
Footnotes
-
Contributors We assure that all authors included on the paper fulfil the criteria of authorship. All have contributed to the conception and design, analysis and interpretation of data, drafting of the article and revising it critically for important intellectual content, and final approval of the version to be published. In addition, we also assure that there is no one else who fulfils the criteria but has not been included as an author.
-
Competing interests All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare that no support was received from any organisation for the submitted work and that there were no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; we did not have other relationships or activities that could appear to have influenced the submitted work.
-
Provenance and peer review Not commissioned; internally peer reviewed.