Article Text

Abstract
Objective: An analysis of airborne nicotine measurements collected in 49 low-income, multi-unit residences across the Greater Boston Area.
Methods: Nicotine concentrations were determined using passive monitors placed in homes over a one-week sampling period and air exchange rates (AER) were sampled using the perfluorocarbon tracer technique. Residents were surveyed through a questionnaire about smoking behaviour and a visual inspection was conducted to collect information on housing characteristics contributing to secondhand smoke (SHS) exposure. Using a mass balance model to account for the air exchange rate, volume of the home and sorption and re-emission of nicotine on indoor surfaces, the effective smoking rate (SReff) was determined for each residence.
Results: Nicotine levels ranged from the limit of detection to 26.92 μg/m3, with a mean of 2.20 μg/m3 and median of 0.13 μg/m3. Nicotine measurements were significantly associated with the number of smokers in the household and the number of cigarettes smoked in the home. The results of this study suggest that questionnaire reports can provide a valid estimate of residential exposure to tobacco smoke. In addition, this study found evidence that tobacco smoke contamination in low-income housing developments is not limited to homes with smokers (either residing in the home or visiting). The frequent report of tobacco smoke odour coming from other apartments or hallways resulted in increased levels of nicotine concentrations and SReff in non-smoking homes, suggestive of SHS infiltration from neighbouring units.
Conclusion: These findings have important implications for smoking regulations in multi-unit homes and highlight the need to reduce involuntary exposure to tobacco smoke among low-income housing residents.
Statistics from Altmetric.com
Numerous epidemiological studies have documented the link between secondhand smoke (SHS) exposure and increased morbidity and mortality.1 Over the past two decades, authoritative reviews of the scientific, engineering and medical literature have established a wide range of adverse health effects from SHS including cardiovascular disease, lung, breast and nasal sinus cancer, asthma and other respiratory illnesses (particularly in children), and low birth weight and sudden infant death syndrome (SIDS) in newborns.1 2 3 4 Recent findings published by the US Surgeon General have determined that “there is no safe level of exposure to secondhand smoke and even brief exposure can affect both children and adults”.1 Despite the increased awareness of health impacts and substantial progress in tobacco control, SHS remains a widespread and unavoidable health hazard for millions of children and non-smoking adults.
Smoking in residential settings presents serious and substantial health hazards, as well as significant challenges in protecting the health and wellbeing of residents. The home is the primary source of SHS exposure for children, and along with the workplace, a predominant location of exposure for adults.1 It is estimated that 60% of children aged 3–11, or approximately 22 million children in the United States are exposed to SHS in their home.1 Parental smoking accounts for almost 90% of the exposure in the home, followed by grandparents and other relatives that live in the residence.5 For residents of multi-unit housing, the source of this problem can extend beyond their residence. SHS can enter a smoke-free residence in a multi-unit housing complex from shared air spaces, ventilation systems, windows, elevator shafts, hallways and holes in walls, pipes and electric outlets.6 In older buildings, about half to two-thirds of the air in a multi-unit residence can infiltrate from neighbouring apartments.7 While eliminating smoking in indoor spaces protects non-smokers from SHS contaminants,8 other approaches such as separating smokers from non-smokers, using air cleaning devices or ventilation technology may reduce, but does not eliminate exposure.9
Few studies have investigated SHS exposure in low-income, multi-unit housing; however, residents may be exposed to elevated levels owing to higher smoking rates and building factors such as smaller units, poor ventilation and infiltration between units.10 In addition, studies have shown that low-income, and underserved racial/ethnic minorities suffer disproportionately from tobacco-related morbidity and mortality, as well as increased incidence of asthma, heart disease and cancer.11 12 13 14
The objective of this study was to characterise SHS exposure in low-income housing developments in urban neighbourhoods surrounding Boston, Massachusetts. Specifically, we examined the distribution of airborne nicotine concentrations as a marker of SHS and assessed the factors that contribute to exposure in multi-resident housing. This study applied a mass balance model to examine the relation between indoor nicotine concentrations, air exchange rates, home volume, and the sorption and re-emission of nicotine on indoor surfaces. Using the resulting effective smoking rates (SReff), we estimated the cigarettes per day (cigs/day) equivalence of SHS exposure in each home. We hypothesised that airflows within the building would be associated with elevated levels of SHS exposure.
Methods
Study design
This study is part of a comprehensive research project in collaboration with the Harvard School of Public Health (HSPH) and Dana Farber Cancer Institute (DFCI) examining the social and physical determinants of cancer risk-related behaviours among multi-ethnic residents in low-income housing developments. As part of this project, week-long integrated samples of vapour-phase nicotine were collected along with the smoking behaviour of residents. An ethnically diverse sample of residents from 49 units within four low-income housing developments in the Greater Boston Area was randomly selected to take part in the study. Participant eligibility included being between 18 and 64 years of age, speaking English, Haitian Creole or Spanish, and residing in a low-income housing development in Cambridge, Somerville or Chelsea, Massachusetts. Residents were invited to participate in the study through meetings of the tenants’ association, and through the distribution of posters and flyers at each of the selected housing developments. All research protocols were submitted for ethics review and approved by the institutional review board (IRB) at the Harvard School of Public Health.
Three methods were used to assess tobacco smoke exposure. An interviewer-administered questionnaire defined household smoking behaviour. A visual inspection observed evidence of smoking, while collecting information about potential housing characteristics contributing to SHS levels in the home. Week-long airborne nicotine concentrations provided a direct measure of SHS. Air exchange rates were also determined over the same period as the nicotine measurements.
Field operations for this study were conducted between mid-March and mid-June 2006. The study required two home visits. During the first visit, a team of two trained research assistants interviewed the resident, conducted a visual inspection and set up the air sampling monitors. After six to seven days, the research assistants returned for the second home visit to retrieve the sampling equipment. Records from the collection instruments were sent to the HSPH laboratory for analysis.
Questionnaire
A questionnaire was used to obtain information in all 49 residences sampled. Survey questions were derived from the HSPH Healthy Public Housing Initiative (HPHI)15 and a review of relevant published literature on indoor air pollution among urban, minority and low-income populations. The survey was translated into Haitian-Creole and Spanish for non-native English speakers and a translator was provided to conduct the interview when needed. Before each interview, a project summary was reviewed with each prospective participant and a signed consent form was collected. The questionnaire assessed demographic information, residential history, household smoking behaviour and physical housing characteristics.
Visual inspection
A visual inspection observed signs of smoking such as active smoking, tobacco odour and the presence of cigarettes, cigars, empty ashtrays, ashtrays with ashes, matches or lighters. Other parameters recorded included housing disrepairs such as holes or damage in the floors, walls and ceilings, and unsealed pipe penetration. In addition, the number of rooms and volume of each residence was measured.
Analytical methods
Passive air nicotine monitors were used to measure vapour-phase nicotine emissions in each residence. Passive diffusion monitors collected vapour-phase nicotine into a sodium bisulfate treated filter held in a 37-mm polystyrene cassette.16 Each device was placed in the participants’ main living area (living room or family room) during the first home visit and remained in the residence for six to seven days. In the laboratory nicotine was extracted from the filter, desorbed in water and analysed by gas chromatography.16 Field blanks and duplicates were obtained for 5% of the samples. The limit of detection (LOD), based on three times the mean blank values, was calculated at 0.021 μg/m3. All nicotine monitors were analysed at the University of California, Berkeley.
The perfluorocarbon (PFT) technique was used to measure air exchange rates in each residence.17 A non-toxic tracer gas (perfluoromethyl cyclohexane) released at a constant rate, is sampled by diffusion onto an adsorbent in capillary absorption tubes (CAT). The source was placed in the middle of the main living area and the CAT was taped to the opposing wall a distance of six feet away from the source. The PFT was thermally desorbed and quantified by gas chromatography with an electron ion detector. Assuming a well-mixed interior space, air exchange rates are calculated based on a mass balance technique outlined by Dietz et al17 at the Harvard School of Public Health. Field blanks were collected for 5% of all samples.
Data analysis methods
Data were maintained in ACCESS and analysed using Statistical Analysis Software version 9.18 The Kruskal-Wallis one-way analysis of variance (ANOVA) was used to test for differences in group means and exposure measures. Median concentrations were compared across different smoking behaviours and housing characteristics, and Wilcoxon rank sum tests were performed to determine statistical significance at a p value of 0.05.
Mass balance model
The effective smoking rate (SReff) was calculated in order to better interpret variability of nicotine concentrations in the residential environment. The SReff accounts for the source strength of the pollutant in each residence based on the nicotine concentration, air exchange rate (AER), volume of the home, and interaction of nicotine on indoor surfaces, such as the gains and losses through sorption and desorption. This method relies on the computation of the mass balance model (equation 1, where SReff is the indoor effective smoking rate (cigarettes/day), Cin is the indoor nicotine concentration (μg/m3), R is the measured air exchange rate (h−1), V is the volume of the home (m3), and EREF is the exposure relevant emission factor (μg/cigarette). Values of Cin, R and V were measured in each home.
Equation 1: Effective smoking rate (SReff)

The mass balance model from Sax et al19 is rearranged to estimate the effective smoking rate (SReff) in each residence through the use of exposure relevant emission factors (EREFs). The EREF accounts for the sorptive uptake and re-emission of SHS constituents representative of smoking rates, ventilation and furnishings in typical residential settings. The use of EREFs are more appropriate to real world scenarios and provide an improved approach to estimating SHS exposure.20 The EREFs for this exposure model were calculated using the measured values from Singer et al,21 for nicotine in a fully furnished room at three ventilation rates (low, moderate and high) representing values in typical residences: 0.3 h−1 (396 (29) μg/cig), 0.6 h−1 (689 (50) μg/cig), and 2 h−1 (1270 (110) μg/cig). Using these data, a linear regression of EREF versus log-transformed AERs was used to estimate EREFs across this range. For AERs below 0.2 h−1, an EREF of 197.3 μg/cig was used, based on the predicted estimate using this regression model.
Results
Demographics
Subject demographics are summarised in table 1 and compared between non-smoking and smoking participants. The study population was predominantly female (96%) with a mean age of 42.5 years (range 26–68). Of the 49 subjects enrolled in the study, 41% were white, 31% were African American, 26% were other race/ethnicity and 2% were Asian; 26% of the study population was of Hispanic or Latino decent. Participants reported spending the majority of time over a typically 24-hour period in their residence, on average 14.2 hours at home, 2.8 hours at work, 2.2 hours shopping and doing errands, 1.9 hours at other locations, 1.8 hours at someone else’s home and 1.1 hours commuting. In addition, respondents reported that a member of the household was home during the day in 65% of the residences. The demographic characteristics of smoking and non-smoking participants did not differ with respect to gender, age or household size. However, the smoking population was predominately white (73%), while the non-smoking population was predominately racial/ethnic minorities.
Population demographics of participants in four low-income housing developments
Nicotine concentrations
Detectable levels of nicotine were measured in 45 (94%) of the 49 residences. Overall, nicotine concentrations ranged from below the limit of detection (LOD) 0.021 μg/m3 to maximum levels of 26.92 μg/m3. The mean nicotine concentration of the study sample was 2.20 μg/m3 and the median concentration was 0.13 μg/m3.
Table 2 presents the summary statistics of the nicotine measurements by the smoking characteristics of the study population. Nicotine concentrations were highly associated with participant smoking status (that is, whether subjects self-identified as smokers or non-smokers) (p<0.0001). Of the subjects enrolled in the study, 69% (n = 33) were non-smoking participants and 31% (n = 15) were smoking participants. The smoking participants smoked an average of 12.5 cigarettes per day (ranging from 2–30). Non-smoking participants had a median concentration of 0.06 μg/m3 ranging from < LOD to 1.81 μg/m3, while smoking participants had a median concentration of 2.93 μg/m3 ranging from 0.09 to 26.92 μg/m3.
Summary statistics of nicotine concentrations by smoking behaviour
The impact of household smoking status (that is, whether there were any smokers, including the study participant, living in the household) was significantly associated with nicotine levels (p<0.0001). The number of household smokers living in the home ranged from none to two, with 48% (n = 23) of the residences having no smokers living in the home, 22% (n = 11) having one smoker and 15% (n = 7) having two smokers. As anticipated, nicotine measurements increased with the number of smokers in the home; households with none, one and two smokers had a median concentration of 0.06 μg/m3, 1.81 μg/m3 and 3.13 μg/m3, respectively.
Visitor smoking status (that is, whether non-residents, such as relatives, friends, neighbours or babysitters ever smoked in the home) was significantly correlated with nicotine measurements (p<0.0001). While 33% of the subjects (n = 16) reported permitting visitor smoking in the home, 67% (n = 32) restricted visitor smoking. Homes with no-smoking visitors had a median concentration of 0.07 μg/m3 (n = 32), while homes with smoking visitors had a median concentration of 2.17 μg/m3 (n = 16).
The source of smoking (that is, visitor smoking only, resident smoking only and resident and visitor smoking) significantly influenced the nicotine levels in the home (p<0.0001). Smoking in the home was reported as coming from 4% visitors only, 10% residents only and 27% both residents and visitors, with median concentrations increasing from 0.18 μg/m3, 0.69 μg/m3 and 2.93 μg/m3, respectively.
The number of cigarettes smoked per day in each residence was significantly correlated with nicotine levels (p<0.0001). Daily exposure to cigarette smoke in the home was reported by 32% of the study population. The number of cigarettes smoked in the home on a typical day ranged from none (30%), 1–5 cigarettes (10%), 6–10 cigarettes (10%), 11–19 cigarettes (4%), to a pack or more cigarettes per day (8%). Households reporting 0 cigarettes smoked per day had a median nicotine level of 0.11 μg/m3, ranging from 0.03–2.53 μg/m3, while households with 1–5, 6–10 and 11–15 cigarettes smoked per day had increasing median concentrations of 1.19 μg/m3, 1.81 μg/m3and 9.28 μg/m3, respectively. The median concentrations were highest when participants smoked a pack or more cigarettes per day (15.74 μg/m3), suggesting that the household smoking rate is a primary determinant of indoor concentrations.
SHS exposure in non-smoking and smoking homes
In order to compare SHS exposure in non-smoking homes with those in smoking homes, data from two subgroups were compiled. Non-smoking participants who lived in smoke-free homes where neither household members nor visitors smoked in the residence were classified as “non-smoking homes” (NSH). All other residences were considered “smoking homes” (SH), defined by one or more smokers in the household, and/or smoking visitors. Another indicator of smoking homes was whether signs of smoking were observed during the visual inspection such as active smoking, visible cigarettes, cigars, empty ashtrays with ashes, matches or lighters and/or smoking odour. This method was effective in revealing misclassification of home environments as non-smoking homes when noticeable signs were evident. Incongruity between questionnaire reported smoke-free homes and observed tobacco use was detected in two residences. Signs of smoking were also an effective predictor of SHS exposure (p<0.0001). Homes in which no signs were observed had a median nicotine concentration of 0.06 μg/m3, while homes in which one or more signs of smoking were present had a median of 2.53 μg/m3.
Nicotine was detected in 89% (17/19) of non-smoking homes and 95% (21/22) of smoking homes. (It should be noted that the one smoking home where nicotine was not detected was classified as a smoking home due solely to visual signs of smoking in the home. No smoking activity by residents or visitors was reported in this home, and thus, it could have been assigned as a non-smoking home. If this home were re-classified, 100% of smoking homes showed detectable levels of nicotine.) Air nicotine levels in non-smoking homes were low, ranging from the LOD to 0.28 μg/m3, with a median of 0.04 μg/m3 and mean of 0.08 μg/m3. Concentrations were significantly higher in smoking homes, ranging from the LOD to 26.92 μg/m3, with a median of 1.50 μg/m3 and a mean of 4.66 μg/m3 (p<0.0001).
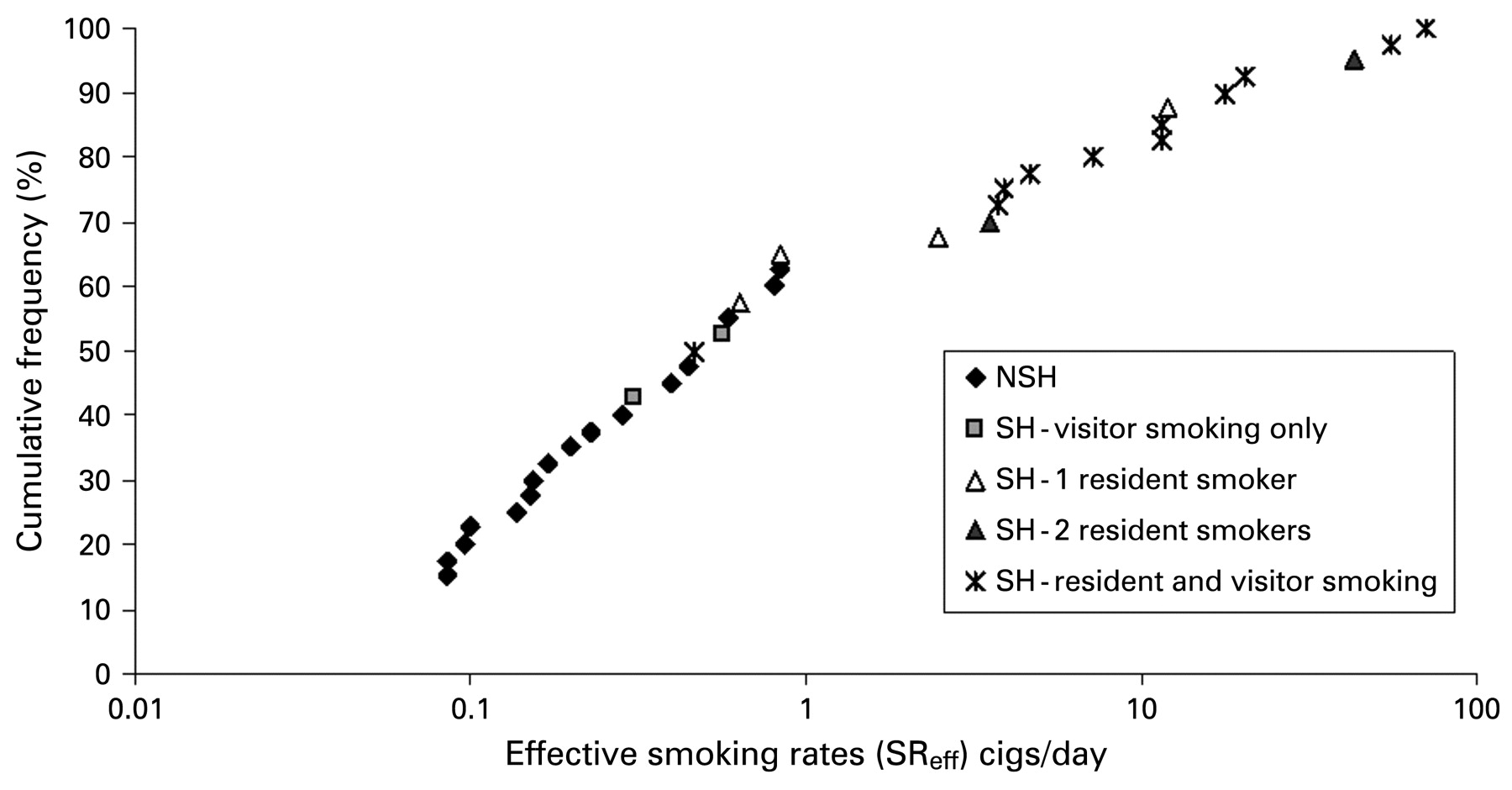
Using the mass balance model, the residence specific effective smoking rate (SReff) was calculated for each residence. Figure 1 presents the cumulative distribution for SReff by smoking status. Smoking homes had a range of 0–70.26 cigs/day, with a median of 3.88 cigs/day and a mean of 12.80 cigs/day (p<0.0001). Homes where two residents smoked, and homes where both residents and visitors smoked were among the highest SReff. However, SHS contamination, as measured by airborne nicotine levels, was not limited to smoking homes. Concentrations in non-smoking homes were equivalent to a range of 0–0.84 cigs/day, with a median value of 0.15 cigs/day and a mean of 0.25 cigs/day. The SReff across non-smoking homes shows that household smoking restrictions do not guarantee a smoke-free residence. Surprisingly, some non-smoking homes were exposed to the equivalent of approximately one cigarette per day smoked in their home.

{kind=link}
Cumulative distribution of effective smoking rates (SReff) by smoking status. aData not available for entire cohort.
Potential infiltration of SHS in residences
The source of SHS exposure in non-smoking homes was further explored by determining the residents’ perception of SHS infiltration from hallways and neighbouring units. Participants were categorised into two groups, those who detected tobacco smoke odour transfer frequently (that is, a few times per week or everyday) and those who detected tobacco smoke odour infrequently (that is, less than once per year, a few times a year, or a few times per month).
Table 3 illustrates the trend in which the frequent report of tobacco smoke odour coming from other apartments or hallways resulted in increased levels of nicotine concentrations and SReff in non-smoking homes. Residents of non-smoking homes who reported frequent tobacco smoke odour were exposed to higher median nicotine concentrations (0.06 μg/m3) than those who rarely smelled cigarette smoke (0.04 μg/m3), although the p value was not statistically significant. The effective smoking rates further confirmed these relations, as those reporting frequent odour detection (0.20 cigs/day) were higher than those reporting infrequent odour detection (0.14 cigs/day), although the p value of 0.462 was not statistically significant. Surprisingly, smoking participants and smoking homes had an inverse trend. This result may be attributed to the smoking participants’ inability to identify an external source of tobacco smoke odour as well as the non-smoking participants. In addition, smoking homes had a higher mean AER of 0.50 h−1 and median 0.37 h−1 ranging from 0 to 1.45 compared to non-smoking homes with a mean of 0.39 h−1, median of 0.26 h−1, ranging from 0 to 0.99 h−1 (p = 0.357).
Tobacco smoke odour from other apartments and hallways. Comparison of infrequent vs frequent tobacco smoke odour detected†
Discussion
The purpose of this study was to determine residential exposure to SHS in low-income, multi-unit residences across the Greater Boston area. The results of this study were consistent with previous research that measured nicotine concentrations in residential environments using similar methods. Median nicotine levels between 1 μg/m3 and 3 μg/m3 and ranging from 0.1 μg/m3 to 8 μg/m3 were reported in homes of smokers across the United States in several studies.22 23 24 25
Although the median nicotine level for smoking homes (2.17 μg/m3) in this study was comparable to previous studies, the range was notably higher, with measurements up to 26.92 μg/m3. Reported increases in nicotine yield in recent years may partially explain differences between this study and earlier reports. For example, several recent analyses of nicotine yield from major brand name cigarettes sold in Massachusetts from 1997 to 2005 found that manufacturers have steadily increased the levels of nicotine in cigarettes by 11% over this period.26 27 Despite this trend, differences in cohort demographics between studies are likely the dominant source of variability. For example, a study of 291 ethnically diverse low-income families in New England measured elevated nicotine concentrations (reaching 18 μg/m3), much higher than previous studies assessing exposure in middle-income and upper-income families.28
This study examined nicotine levels in relation to household smoking behaviour and assessed the variability of exposure by smoking status. While the prevalence of smoking was high in our cohort (31%), this rate is consistent with reported rates among low-income populations in Boston (34.4%).29 Participant, household, and visitor smoking status were found to be highly predictive of measured nicotine concentrations. In addition, vapour phase nicotine measurements were highly correlated with the number of cigarettes reported being smoked in the home per day. Previous studies on the validity of questionnaire reported smoking have also found associations with air nicotine concentrations and participant reports of smoking in the home.24 30 31 32 The results of this study indicate that the cessation of home smoking will significantly reduce SHS contamination and exposure.
This study found evidence to suggest that SHS contamination is not limited to homes with active smokers. SHS may infiltrate into homes through windows, doors, shared air spaces, holes and ventilation systems if cigarettes are smoked outside or in neighbouring residences. Little is known about the variability of SHS when contamination is generated by smokers from outside the building envelope or from adjoining units. However, this study points to an observed association between elevated nicotine concentrations and effective smoking rates and the increased frequency of smelling cigarette odour from other apartments, hallways or outside the building. These findings suggest that living in a multi-unit dwelling with smoking residents in the building may place non-smokers at risk of SHS exposure. These findings implicate that reducing outside sources of cigarette smoke is an effective strategy for lessening household exposure levels.
The use of the questionnaire to evaluate the respondents’ exposure to SHS presented limitations that should be considered. Misclassification of exposure may result from the respondents’ lack of awareness of cigarette exposure, inadequate recall, or possible deception in reporting smoking status. However, the visual inspection tool, when used in conjunction with a questionnaire, was helpful to validate the smoking information provided by the respondents. In addition, this study did not control for the location of smoking in the residence in relation to the sampling area. Additional information on the smoking locale (that is, kitchen, bedroom, patio, etc) may improve the observed relation between nicotine levels and the source strength in the home. More research is needed to determine whether SHS exposure is best characterised by the nicotine level in the main living area, bedroom, highest level in the home or an average of all of the rooms.33
Recent studies have also highlighted the potential for deposited or adsorbed particulates or gases to contribute to household exposure to toxic compounds originating from smoking (“third-hand smoke exposure”).34 Owing to the complicated behaviour of many semivolatile compounds, including nicotine, in indoor environments,35 it will be critical to develop mechanistic models to correctly identify dominant exposure pathways and estimate health risks from these exposures.
Although policy efforts continue to address appropriate boundaries of smoking in the public and private sector, restriction of smoking in multi-unit homes has not received the same degree of attention. Public health policies to limit SHS exposure in public spaces and encourage the elimination of smoking in the home are critical. Since contaminated indoor environments may present health risks to unsuspecting non-smokers, regulations may need to require the disclosure of the smoking status of previous tenants and neighbouring apartments. Approaches for addressing the issue of smoke infiltration in low-income housing include educating landlords and property managers to implement voluntary smoke-free policies, creating rules to restrict smoking in common spaces such as entrances, elevators and laundry rooms within the housing complex and changing building design and operation to control infiltration of contaminated air.36 Local health jurisdictions can work with owners and managers of multi-unit residences to encourage the designation of smoke-free buildings for the health as well as enjoyment of the residents.
What this paper adds
Limited research has investigated secondhand smoke (SHS) exposure in low-income, multi-unit housing; however, residents may be exposed to elevated levels of SHS because of higher smoking rates and building factors such as smaller units, poor ventilation and infiltration between units.
This study examines the relation between indoor nicotine concentrations, air exchange rates, home volume and sorption and re-emission of nicotine on indoor surfaces, in order to determine the prevalence of SHS exposure in low-income, multi-unit residences. The results of this analysis indicate that SHS is not limited to residences with smokers (either residing in the home or visiting). The frequent report of tobacco smoke odour coming from other apartments or hallways resulted in increased levels of nicotine concentrations in non-smoking homes, suggestive of SHS infiltration from neighbouring units.
The study also demonstrates that effective smoking rates may be an important and valid measure that can be used to improve our understanding of the variability of nicotine concentrations in the residential environment.
These findings have important implications for smoking regulations in multi-unit homes and highlight the need to reduce involuntary exposure to tobacco smoke among low-income housing residents.
In addition to policy restrictions on smoking, efforts to educate the public about the risks associated with SHS exposure at home may be an effective means of reducing exposure. Healthcare providers and public health advocates need to play a stronger part in informing the public about the health effects of SHS exposure, and the positive impact that smoking restrictions can have on household members. Interventions to motivate smokers to consider cessation through the awareness of the benefits of exposure reduction should be implemented in low-income housing developments. Given the relatively serious health consequences associated with exposure to SHS, this study highlights the importance of continued efforts to develop and evaluate effective exposure assessments targeting racial/ethnic minorities and low-income housing populations. Such efforts would provide much needed information and education about this very common public health problem and give residents of multi-unit homes the tools to protect their families from the detrimental health effects of secondhand smoke.
Acknowledgments
The authors would like to acknowledge the administrative and field staff at the Harvard School of Public Health, Dana Farber Cancer Institute and the Harvard Extension School, and the study participants for their contributions to this project. They also thank Beatriz Vinas and Jose Vallarino at the Harvard School of Public Health, Brett Singer at the Lawrence Berkeley National Laboratory and Amy Harley, Lorraine Wallace, Marty Alvarez-Reeves, Ruth Lederman, Mike Massagli, Anne Stoddard, Roberta Goldman and Glorian Sorensen (PI) at the Dana Farber Cancer Institute for their contributions to the overall study design and implementation.
REFERENCES
Footnotes
Funding This research was supported by the Harvard School of Public Health and Dana Farber Cancer Institute, with funding provided by the National Cancer Institute, (grant No 1 R01 CA111310-01A1). Principal investigator: Glorian Sorensen.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Attributable departments/institutions: Department of Environmental Health, Harvard School of Public Health, Landmark Center West, 401 Park Drive, Boston, MA 02215, USA.