Article Text

Abstract
Aims To determine the most prominent individual and interpersonal triggers to quit smoking in China and their associations with sociodemographic characteristics.
Methods Data come from Waves 1–3 (2006–2009) of the International Tobacco Control (ITC) China Survey, analysed cross-sectionally as person-waves (N=14 358). Measures included sociodemographic and smoking characteristics. Those who quit between waves (4.3%) were asked about triggers that ‘very much’ led them to stop smoking, and continuing smokers about triggers that ‘very much’ made them think about quitting. Triggers covered individual (personal health concerns, cigarette price, smoking restrictions, advertisements, warning labels) and interpersonal factors (family/societal disapproval of smoking, setting an example to children, concerns about secondhand smoke).
Results Over a third of respondents (34.9%) endorsed at least one trigger strongly; quitters were more likely than smokers to mention any trigger. While similar proportions of smokers endorsed individual (24.4%) and interpersonal triggers (24.0%), quitters endorsed more individual (61.1%) than interpersonal (48.3%) triggers. However, the most common triggers (personal health concerns; setting an example to children) were the same, endorsed by two-thirds of quitters and a quarter of smokers, as were the least common triggers (warning labels; cigarette price), endorsed by 1 in 10 quitters and 1 in 20 smokers. Lower dependence among smokers and greater education among all respondents were associated with endorsing any trigger.
Conclusions Individual rather than interpersonal triggers appear more important for quitters. Major opportunities to motivate quit attempts are missed in China, particularly with regard to taxation and risk communication. Interventions need to focus on more dependent and less-educated smokers.
- Public policy
- Low/Middle income country
- Taxation
- Price
- Packaging and Labelling
Statistics from Altmetric.com
Introduction
As the largest tobacco producer and consumer in the world, China has been severely hit by the tobacco epidemic. It accounts for approximately 40% of the world's cigarette production and one-third of the world's cigarette consumption. 1 Chinese smokers constitute one-third of the world's smoking population.2 Smoking prevalence has remained high in China, with male smoking prevalence standing at 52.9%.3 As a consequence, 1.4 million deaths are attributable to tobacco in China each year, and this is projected to rise to about 3 million deaths by 2050.4
Cultural and institutional barriers remain the major challenge in tobacco control faced by China, where smoking has a positive social meaning and knowledge of smoking risks is poor among the public.5 ,6 This is attributable to the weak support of tobacco control policies in China, a country which has yet to meet the recommended WHO Framework Convention on Tobacco Control (FCTC) guidelines. Although 13 cities revised or formulated local smoke-free regulations in accordance with the FCTC Article 8 Guidelines, which were adopted in 2008, there is no national smoke-free law in China which could avert 100 000 deaths attributed to secondhand smoking annually.7 Poor coverage of tobacco advertising bans leaves loopholes for tobacco advertising activities through sponsorship, points of sale and online advertising. Text-only health warning labels occupying only 30% of the display area of Chinese cigarette packages are yet to meet the Article 11 Guidelines, which were also adopted in 2008, which call for pictorial labels covering at least 50% of the display area.8 Moreover, an increase in excise tax on cigarettes at the producer level in 2009 in China has had no effect on the retail price of cigarettes, thus failing to meet the Article 6 Guidelines, which were adopted in 2014.9 ,10
Identifying the most influential factors that motivate quit attempts among smokers and increase abstinence in China could help to prioritise tobacco control efforts. While such factors can be thought of as motives, reasons or micro indicators for quitting,11 and notwithstanding considerable overlap in these concepts, we refer to these factors in this paper as ‘triggers’, a term that is in line with previous research,12 given that we refer to factors that represent specific concerns that are known to be related to quitting.
Data from high-income countries (HICs) such as the USA, the UK, France, Australia and Canada suggest that concern for personal health, setting an example for children and cigarette price are among the top three triggers to quit smoking.7 ,12–15 Learning about sociodemographic associations with these factors may also be useful in identifying and tailoring effective tobacco control interventions to particular sociodemographic groups. In terms of sociodemographic associations with triggers to stop, anti-smoking advertisements appear to be most effective in younger smokers, future health concerns are more likely to be cited by higher socioeconomic status (SES) smokers and cost is more likely to be cited by lower SES smokers.12 Further, younger smokers are more likely to consider socialising as a motive to smoke while older smokers are more likely to consider personal enjoyment as the main motive.16
Relatively little is known about the most important triggers prompting quit attempts and smoking cessation in China. It would be inappropriate to generalise findings from HICs to China, an upper middle-income country with a different cultural outlook and at a different stage in the tobacco epidemic.17 For instance, smokers from HICs have a significantly greater knowledge of smoking risks and greater intention to quit smoking than smokers in China.18 Moreover, women and older smokers are more supportive of public smoking bans in China, whereas women in HICs tend to be less supportive of smoking bans in restaurants.19 ,20
This paper therefore aims to identify the most prominent triggers to stop smoking among current smokers and quitters in China. Comparing the relative importance of particular triggers as endorsed by current smokers who have not succeeded in stopping and quitters who have been successful in stopping may help to identify those factors that are most effective in motivating smoking cessation and which interventions to prioritise in China. Moreover, identifying sociodemographic differences in the motivational antecedents of stopping smoking can lead to evidence-based efforts to develop more effective tailored tobacco control interventions. Given that China has a traditional collectivist outlook, which places greater value on social acceptance compared with an individualist outlook, which values personal success,21 this paper also distinguishes between interpersonal, socially oriented triggers and personal, individually oriented triggers. This will allow comparisons between socialising factors and individual factors in terms of their influence on smoking cessation in different sociodemographic groups.
In short, then, this study addressed the following research questions:
What are the most prominent individual and interpersonal triggers to quit smoking reported by quitters and smokers in China?
Which, if any, sociodemographic characteristics are associated with these triggers?
Methods
Study design and sample
The International Tobacco Control (ITC) Project has conducted longitudinal cohort surveys in 22 countries to examine the factors that are associated with tobacco use and cessation. One important objective of the ITC Project is to assess the psychosocial and behavioural impact of WHO FCTC policies.
Data come from the ITC China Surveys, which were conducted by researchers from local and central offices of the Tobacco Control Office, Chinese Center for Disease Control and Prevention, and an international team of researchers of the ITC Project, centred at the University of Waterloo. Four waves of the ITC China Survey were conducted in six cities in Mainland China, which were selected due to their differences in size, location and economic development: Beijing, Changsha, Guangzhou, Shanghai, Shenyang and Yinchuan.
Details of the sampling method and design for the ITC China Survey are presented elsewhere.22 Briefly, respondents were selected using a multistage cluster sampling design to ensure a representative sample of adult smokers and non-smokers in each city. Smokers were defined as those who had smoked at least 100 cigarettes in their lifetime and were currently smoking at least once a week. The demographic characteristics, smoking and smoking-related behaviours, policy-relevant measures related to FCTC domains and psychosocial precursors to smoking and cessation of each respondent were collected using standardised questionnaires through face-to-face interviews.
In each city, a random sample of approximately 800 adult smokers and 200 adult non-smokers were surveyed. At Waves 2 and 3, the cohort was replenished to maintain the sample size by recruiting new respondents from the same sampling frame. Owing to the longitudinal design of the survey, a sample of ex-smokers (quitters) who had been smokers at recruitment was identified; these quitters still participated in the survey, answering questions which reflected the fact that they had quit smoking. The analyses reported in this paper were conducted on data from smokers and quitters surveyed in Waves 1 through 3 (data of Wave 4 were not yet available), excluding respondents recruited as non-smokers.
The sample sizes were: Wave 1 (conducted April–August 2006)=4732 smokers; Wave 2 (October 2007–January 2008)=3709 smokers, 217 quitters and 917 newly recruited smokers (retention rate 83%); Wave 3 (May–October 2009)=3549 smokers, 374 quitters and 860 newly recruited smokers (retention rate 81%). The data set analysed for this paper was a sample of 14 358 person-waves (with each respondent contributing responses from one, two or three survey waves).
Ethics approval was obtained from research ethics boards or institutional review boards at the University of Waterloo (Waterloo, Canada), Roswell Park Cancer Institute (Buffalo, USA), The Cancer Council Victoria (Melbourne, Australia) and the Chinese Center for Disease Control and Prevention (Beijing, China).
Measures
Outcome variables
All smokers and quitters answered a multipart question. For smokers, the question was: “In the past 6 months, have each of the following things led you to think about quitting?”; for quitters, the question was: “Which of the following things led you to quit?”. There were nine items in the list which followed, and these were divided into two different types of variables:
Interpersonal variables were: (A) concern about the effect of secondhand smoke on non-smokers, (B) disapproval of smoking in Chinese society, (C) setting an example for children and (D) disapproval of smoking in the family.
Individual variables were: (A) the price of cigarettes, (B) smoking restrictions in public and workplaces, (C) advertisements or information about the health risks of smoking, (D) health warning labels on cigarette packages and (E) concern for personal health.
Unless where otherwise stated, the variables were dichotomised based on the response to the question, coded ‘yes’ if the smoker or quitter agreed that the particular variable had led them to think about quitting (or had led them to quit) ‘Very Much’, and coded ‘no’ for all other responses (ie, Not at all, Somewhat, Refused or Don't know).
Covariates
Sociodemographic covariates included age, gender, household income, marital status, education and ethnicity. Based on the cut-offs for urban areas from the 2010 China Statistics Yearbook,23 monthly household income was classified into three groups: low (<¥1000), medium (¥1000–¥3000) and high (>¥3000). Education was classified into low (less than high school), medium (high school) and high (more than high school). Ethnicity was classified into Han Chinese and non-Han Chinese. Lastly, nicotine dependence (heaviness of smoking index24) and city were also included as covariates in analysis.
Analysis
Data were analysed using SPSS V.20. The analysis was carried out at the level of person-waves, and thus generalised estimating equation (GEE) models with a logit link function, specifying an unstructured correlation matrix, were conducted to account for the correlated observations. Given the specific survey design, weighted logistic regressions, using complex samples analysis, were used to obtain CIs, and significance values for the point estimates were derived from GEE to assess associations between predictor and outcome variables, controlling for all other variables and covariates. Due to the large number of associations to be tested, the Benjamini-Hochberg procedure25 was used to adjust the significance level for multiple comparisons.
Results
As shown in Table 1, the sample was mainly male, Han Chinese, married, with at least high school education and medium-level income. Most smokers reported a moderate level of dependence. Across waves, relatively few smokers had stopped since recruitment (4.3%, 95% CI 3.4% to 5.3%) and there were only a few differences between quitters and smokers: quitters were somewhat more affluent and less dependent than smokers (Table 1).
Sample covariates (sociodemographic and smoking characteristics) by smoking status*
The most prevalent individual and interpersonal triggers to quit smoking reported by quitters and current smokers
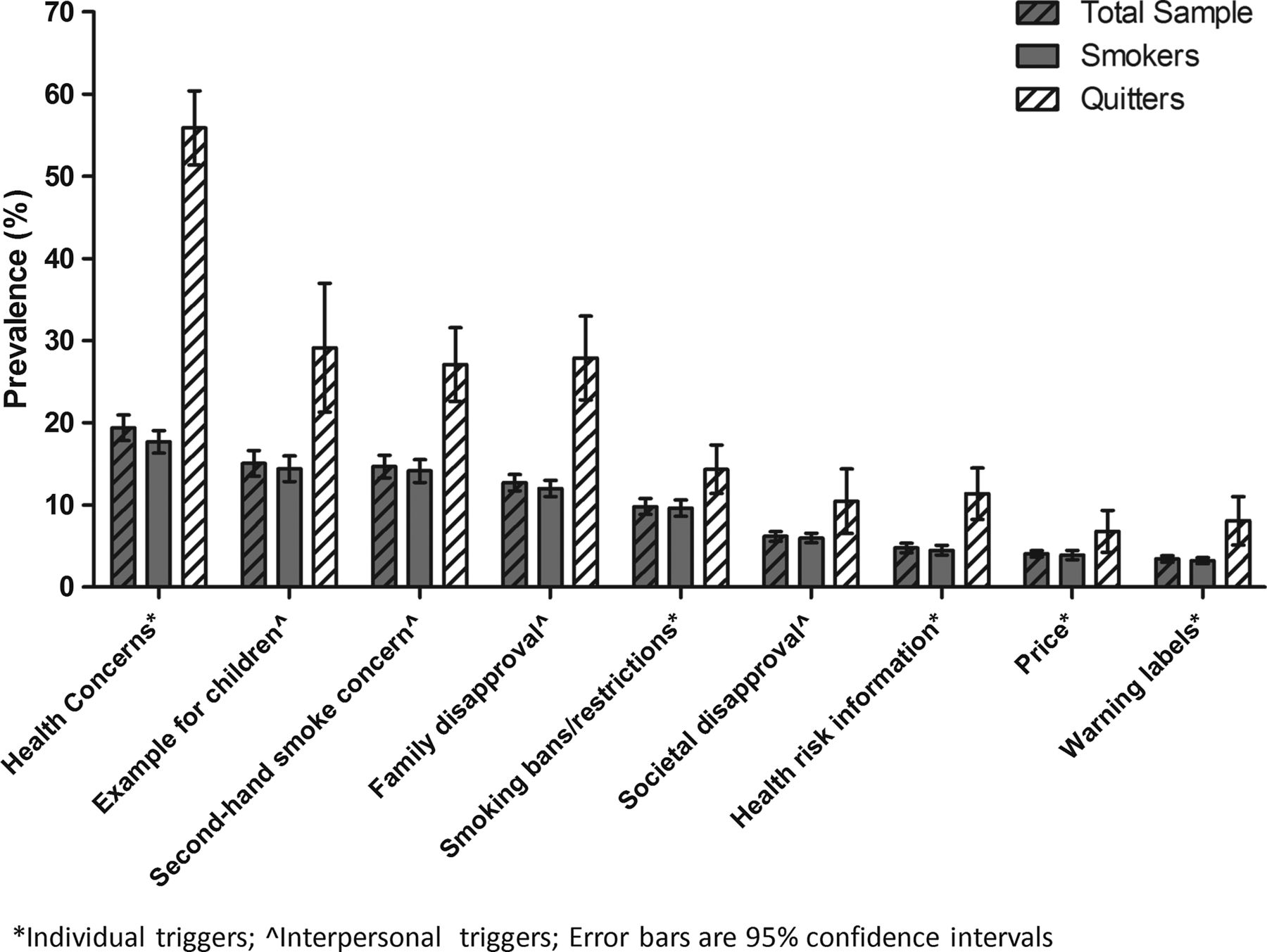
Overall, slightly more than one-third of respondents (34.9%, 95% CI 32.6% to 37.3%) endorsed at least one trigger ‘very much’ and 78.2% (95% CI 76.3% to 80.1%) endorsed one trigger or more at least ‘somewhat’. Similar proportions of respondents ‘very much’ endorsed individual factors (26.1%, 95% CI 24.3% to 27.8%) and interpersonal factors (25.0%, 95% CI 23.1% to 27.0%). As shown in Figure 1, quitters were more likely than smokers to endorse any of the triggers, after adjusting for sociodemographic and covariate characteristics (adjusted odds ratio (AOR) 4.89, 95% CI 3.72 to 6.43). While over two-thirds of quitters had endorsed at least one trigger (71.3%, 95% CI 65.8% to 76.8%), only one-third of smokers had done so (33.3%, 95% CI 31.1% to 35.4%). This difference was much more pronounced for individual triggers, endorsed by 61.1% (95% CI 57.0% to 65.2%) of quitters and 24.4% (95% CI 22.8% to 26.0%) of smokers (AOR 4.55, 95% CI 3.60 to 6.70), than it was for interpersonal triggers, endorsed by 48.3% (95% CI 42.4% to 54.2%) of quitters and 24.0% (95% CI 22.2% to 25.8%) of smokers (AOR 3.07, 95% CI 2.29 to 4.12).
{kind=link}
Prevalence of triggers endorsed as a function of smoking status.
This was mainly due to the disparate endorsement of health concerns by the two groups, which was far more prevalent among quitters than smokers (Figure 1). However, the overall rank order of triggers was very similar for smokers and quitters. Overall, one in five respondents mentioned health concerns as a trigger for quitting or attempting to quit, followed by concerns for children and concerns about the impact of secondhand smoke on non-smokers, mentioned by at least 15% of the total sample. The most uncommon triggers—information about health risks, the price of cigarettes and warning labels—were mentioned by less than 1 in 20 respondents.
Sociodemographic characteristics associated with individual and interpersonal triggers to quit smoking
Higher education (AOR 1.15, 95% CI 1.06 to 1.26) and lower dependence (AOR 0.88, 95% CI 0.85 to 0.91) were the significant predictors of endorsing any triggers among smokers, and higher education (AOR 1.60, 95% CI 1.01 to 2.55) the only significant predictor among quitters, controlling for all other variables. In addition, smokers from Beijing were more likely to endorse any trigger than smokers from Changsha (AOR 0.68, 95% CI 0.52 to 0.90) and Shanghai (AOR 0.54, 95% CI 0.42 to 0.69), but smokers from Yinchuan (AOR 1.39, 95% CI 1.14 to 1.70) were more likely to endorse triggers than those from Beijing. Similarly, quitters from Changsha (AOR 0.33, 95% CI 0.14 to 0.75) and Shanghai (AOR 0.39, 95% CI 0.18 to 0.85) were less likely to endorse any trigger than quitters from Beijing.
When considering associations with endorsement of at least one individual and one interpersonal trigger separately, there were some differences for smokers and quitters. Among quitters, there were no consistent, significant associations with individual triggers and for interpersonal triggers, only geographic associations emerged: quitters from Shanghai (AOR 0.32, 95% CI 0.13 to 0.81) and Changsha (AOR 0.21, 95% CI 0.11 to 0.42) were less likely to endorse any interpersonal triggers than quitters from Beijing. This lack of significance of associations may also reflect the relatively low power to detect such effects.
Among smokers, there were consistent associations of endorsement of individual and interpersonal triggers with both higher education (AOR 1.13, 95% CI 1.01 to 1.25 and AOR 1.20, 95% CI 1.08 to 1.32, respectively) and lower dependence (AOR 0.89, 95% CI 0.85 to 0.93 and AOR 0.85, 95% CI 0.81 to 0.89, respectively). As for quitters, there were some geographic associations. Smokers from Shanghai were less likely (AOR 0.58, 95% CI 0.44 to 0.78) and smokers from Yinchuan more likely (AOR 1.40, 95% CI 1.13 to 1.74) than smokers from Beijing to endorse any individual triggers. Similarly, smokers from Shanghai (AOR 0.53, 95% CI 0.41 to 0.69) or Changsha (AOR 0.58, 95% CI 0.43 to 0.78) were less likely than smokers from Beijing to endorse any interpersonal triggers. However, smokers from Shenyang (AOR 1.43, 95% CI 1.05 to 1.95) or Yinchuan (AOR 1.41, 95% CI 1.1.4 to 1.75) were more likely than smokers from Beijing to endorse at least one interpersonal trigger.
Tables 2 and 3 provide a breakdown of associations with specific individual and interpersonal triggers, respectively. In addition to the above observed predictors of endorsing at least one individual or interpersonal trigger, the results show that male quitters were less likely than female quitters to mention smoking restrictions in public or workplaces as a factor in stopping smoking, and lower income was associated with a greater likelihood of mentioning price of cigarettes as a trigger to stop in smokers (Table 2). Married/cohabiting smokers were more likely than those who were not to cite setting an example to children as a trigger to stop smoking as were younger smokers; older smokers were more likely to endorse societal disapproval as a factor in stopping smoking (Table 3).
Multivariable associations of covariates with individual triggers to stop smoking in current smokers and quitters
Multivariable associations of covariates with interpersonal triggers to stop smoking in current smokers and quitters
Discussion
Overall, one-third of quitters or current smokers in China endorsed at least one prominent trigger to quit smoking ‘very much’. However, quitters were much more likely than smokers to endorse any of the triggers, in particular individual as compared with interpersonal triggers. Nonetheless, the order of importance of triggers was relatively similar in both groups.
As is the case in HICs such as the USA, the UK and France, concern for personal health was the most commonly cited trigger.12 ,14 ,15 However, unlike in these countries where the price of cigarettes is often mentioned as the main reason for stopping smoking,14 ,15 ,26 ,27 price was among the least important triggers to quit smoking in China. ITC studies have shown that cigarettes are highly affordable in China compared with other countries and that the affordability is increasing.28 Chinese smokers engage in cost/price-reducing purchase behaviours such as choosing a cheaper cigarette brand in the lower income group and buying in cartons in the higher income group rather than quitting.29 Health warnings, commonly mentioned as a trigger to quitting,30 ,31 were rarely mentioned by Chinese smokers or quitters, possibly in part due to the non-specific, small, text-only health warnings in China.8 ,32 In addition, few respondents mentioned that receiving health risk information had triggered a quit attempt, consistent with the low level of information campaigns in China on the harms of smoking.33 Moreover, while advice from health professionals is a commonly cited reason for unplanned quit attempts in HICs,34 compared with other countries a relatively large number of medical professionals in China are smokers,35 who may be more resistant to providing stop advice.
Given the relative importance of traditional family values and the Chinese perception of cigarettes as a social connection builder,36 ,37 some of these disparities may arise from cultural differences. Chinese smokers residing within a largely collectivist society may have different attitudes than smokers from HICs, as social disapproval of smoking is a more significant predictor of regret of smoking in Asian countries than in Western HICs.38 Interestingly, however, in China, as elsewhere, individual factors seemed to be more important than interpersonal factors for smoking cessation. Individual triggers were endorsed more than interpersonal triggers among those who had successfully quit. The fact that interpersonal factors such as societal disapproval did not feature highly among triggers to stop smoking may reflect the tobacco-friendly atmosphere in Chinese society, where societal pressures are supportive of, rather than detrimental to, smoking. This, of course, is not immutable and it is interesting to note that some consistent geographic associations were observed for both individual and interpersonal triggers to stop. These associations largely map on to local smoke-free policy, that is, smokers from cities with weaker policies at the time of the survey (Shanghai, Changsha) were generally less likely to endorse triggers than smokers from cities where smoking bans (Beijing, Shenyang, Yinchuan), had been implemented.
Across waves, the quit rate was low with few sociodemographic differences between smokers and quitters. The only factor associated with stopping smoking successfully was income: quitters tended to be more affluent, which is consistent with findings in HICs which show that higher SES smokers are more likely to quit successfully.39 In addition, smokers and quitters with higher education and smokers with lower dependence were generally more likely to endorse triggers. This finding is in agreement with studies from other countries which show that people with a higher education background have a lower probability of relapse,40 whereas smokers with lower nicotine dependence are more successful in staying abstinent,41 ,42 and smokers with a lower education background have higher nicotine dependence and lower intention to quit smoking.43
Our results have a number of implications. First, the findings suggest the need to focus tobacco control interventions on less-educated but more nicotine-dependent smokers, who may be especially susceptible to misperceptions about smoking.44 This could be done by tailoring health messages to be as simple and comprehensible as possible to overcome such misleading myths.6
Second, though the current Chinese government has prohibited Chinese officials from exchanging cigarettes as gifts,45 the findings demonstrate the need for further education campaigns to dispel the general, long-standing positive perception held by the Chinese population towards smoking as indicated by the low levels of perceived societal disapproval of smoking.46 As has been done in other public health campaigns,47 one way to influence the public attitude towards smoking could be to utilise famous, respected Chinese public figures such as the First Lady of China, Peng Liyuan, and the basketball star, Yao Ming, to promote anti-smoking messages.48 ,49 Traditional family values can also be a potential tool in tobacco control. Although there may be a danger that children may rebel against parents, as Chinese teenagers are taught to listen to their parents and elders in order to show respect and maintain family harmony, parents and grandparents can be a powerful and effective medium to transmit anti-smoking messages by expressing disapproval of smoking to their children.37 This should, however, be combined with encouraging parents to stop smoking by emphasising the need to set an example for children in the family. Health education campaigns should be designed to convey a message of family disapproval of smoking as well as setting an example for children, consistent with the finding that this was among the commonly cited triggers.
Third, this study demonstrates that important opportunities—in particular regarding cigarette price and graphic warning labels—may be missed in China. Cost is a major factor in smoking cessation globally and warning labels have been shown to increase knowledge and quit attempts at no cost.16 ,27 Even though cigarettes are highly affordable in China, the fact that price was a trigger to consider stopping smoking among the less affluent smokers in this study suggests that raising the tax on tobacco products at the retail end instead of the producer end could be effective, especially for low-income smokers.50 In addition, using effective risk communication is important, for example, by imposing graphic warning labels, which are easier to understand for less educated smokers, with at least 50% at the top of the front and back of cigarette packages as recommended by the FCTC Article 11 Guidelines. The observation that local changes in tobacco control policy are associated with greater endorsement of triggers to stop also underscores the real effect that these changes can have on attitudes towards smoking. Indeed, implementing FCTC guidelines, in particular price and tax measures (Article 6) and education, communication, training and public awareness (Article 12), has been estimated to potentially reduce smoking prevalence by up to 41% by 2050, saving millions of lives in China.51
This study has a number of limitations. Although the observational nature of the study precludes any causal interpretation, the main purpose of the paper was descriptive and likely confounders were controlled for in analysis. The best way to assess any causal associations between triggers and behaviour is in an experimental design. The assessment of triggers to quit among ex-smokers was retrospective and ideally this would be assessed in real time, for example, using ecological momentary assessment. However, this would not have been practical given the sample size, and it is difficult to see how the retrospective analysis would have introduced biases compared with other similar studies on triggers. While there was no biochemical verification of smoking status, self-report is common practice and largely reliable.52 Lastly, though the sample used in the study was not a truly national sample, the selected cities covered a geographically wide and diverse area of China. Within the chosen cities, weights were used to ensure representativeness.
In conclusion, this study is among the first to consider explicitly not only the relative importance of different triggers to stop on smoking behaviour but also the impact of sociodemographic characteristics on quitting attitude and triggers to stop in China. This paper highlights the need to target tobacco control interventions at the less-educated and more nicotine-dependent smokers in China by working on health education, tobacco tax and warning labels on cigarette packages.8 ,9 More generally, in addition to maximising the effectiveness of tobacco control interventions by targeting particular audience groups, these results underline the urgent need to implement FCTC guidelines in order to reduce smoking prevalence, regardless of sociodemographic characteristics, to provide sufficient help and information to encourage smoking cessation. Given the low endorsement of triggers among smokers in China, there is scope for future research to investigate if there are other main triggers specific to this country.
What this paper adds
This is the first study to identify individual and interpersonal triggers and compare their relative importance for stopping smoking in a Chinese sample of adult urban smokers and recent quitters.
Individual rather than interpersonal triggers are more important for quitters but not smokers. Similar to Western samples, ‘personal health concerns’ are the most commonly cited trigger to quit in the Chinese population; however, in contrast to high-income countries, the price of cigarettes and health risk information are not important triggers for quitting smoking.
Acknowledgments
LS and AM are part of the UK Centre for Tobacco and Alcohol Studies.
References
Footnotes
Contributors PKI, MET, GTF and LS designed the study. GTF and YJ collected the data. PKI and LS conducted the data analysis. AM, MET and GTF contributed to data interpretation. PKI wrote the first draft. AM, MET, GTF, SX, ACKQ and LS revised the draft. The final version of this paper has been reviewed and approved by all coauthors.
Funding The ITC China Project was supported by grants from the US National Cancer Institute (R01 CA125116 and P01 CA138389), the Roswell Park Transdisciplinary Tobacco Use Research Center (P50 CA111236), the Robert Wood Johnson Foundation (045734); the Canadian Institutes of Health Research (57897, 79551 and 115016), and the Chinese Center for Disease Control and Prevention. Additional support was provided to Geoffrey T Fong from a Senior Investigator Award from the Ontario Institute for Cancer Research and a Prevention Scientist Award from the Canadian Cancer Society Research Institute.
Competing interests LS reports personal fees from pharmaceutical companies that make smoking cessation products, outside the submitted work.
Patient consent Obtained.
Ethics approval Ethics approval was obtained from the research ethics board or the institutional review board at the University of Waterloo (Waterloo, Canada), Roswell Park Cancer Institute (Buffalo, USA), The Cancer Council Victoria (Melbourne, Australia) and the Chinese Center for Disease Control and Prevention (Beijing, China).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from the International Tobacco Control Policy Evaluation (ITC) Project are available to approved researchers 2 years after the date of issuance of cleaned data sets by the ITC Data Management Centre. Researchers interested in using ITC data are required to apply for approval by submitting an International Tobacco Control Data Repository (ITCDR) request application and subsequently to sign an ITCDR Data Usage Agreement. To avoid any real, potential, or perceived conflict of interest between researchers using ITC data and tobacco-related entities, no ITCDR data will be provided directly or indirectly to any researcher, institution, or consultant that is in current receipt of any grant monies or in-kind contribution from any tobacco manufacturer, distributor, or other tobacco-related entity. The criteria for data usage approval and the contents of the Data Usage Agreement are described online (http://www.itcproject.org).