Article Text

Abstract
Objective To evaluate the safety and effectiveness of e-cigarettes, by comparing users of only e-cigarettes, smokers of only tobacco cigarettes and dual users.
Design Prospective cohort study. We update previous 12-month findings and report the results of the 24-month follow-up.
Data sources Direct contact and questionnaires by phone or via internet.
Methods Adults (30–75 years) were classified as: (1) tobacco smokers, if they smoked ≥1 tobacco cigarette/day, (2) e-cigarette users, if they inhaled ≥50 puffs/week of any type of e-cigarette and (3) dual users, if they smoked tobacco cigarettes and also used e-cigarettes. Carbon monoxide levels were tested in 50% of those declaring tobacco smoking abstinence. Hospital discharge data were used to validate possibly related serious adverse events in 46.0% of the sample.
Main outcome measures Sustained abstinence from tobacco cigarettes and/or e-cigarettes after 24 months, the difference in the number of tobacco cigarettes smoked daily between baseline and 24 months, possibly related serious adverse events.
Results Data at 24 months were available for 229 e-cigarette users, 480 tobacco smokers and 223 dual users (overall response rate 68.8%). Of the e-cigarette users, 61.1% remained abstinent from tobacco (while 23.1% and 26.0% of tobacco-only smokers and dual users achieved tobacco abstinence). The rate (18.8%) of stopping use of either product (tobacco and/or e-cigarettes) was not higher for e-cigarette users compared with tobacco smokers or dual users. Self-rated health and adverse events were similar between all groups. Among those continuing to smoke, there were no differences in the proportion of participants reducing tobacco cigarette consumption by 50% or more, the average daily number of cigarettes and the average self-rated health by baseline group. Most dual users at baseline abandoned e-cigarettes and continued to smoke tobacco. Those who continued dual using or converted from tobacco smoking to dual use during follow-up experienced significant improvements in the 3 outcomes compared with those who continued or switched to only smoking tobacco (p<0.001).
Conclusions E-cigarette use alone might support tobacco quitters remaining abstinent from smoking. However, dual use did not improve the likelihood of quitting tobacco or e-cigarette use, but may be helpful to reduce tobacco consumption. Adverse event data were scarce and must be considered preliminary.
Trial registration number NCT01785537.
- Electronic nicotine delivery devices
- Cessation
- Harm Reduction
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Despite their potential public health relevance, the current evidence on the safety and efficacy/effectiveness of e-cigarettes is scarce, and long-term data are urgently needed.1–7 The published prospective evidence on the efficacy/effectiveness for healthy participants consists of 2 randomised trials,8 ,9 2 single-arm small trials10–12 and 11 observational studies.13–23 However, these studies mostly included users of both tobacco and e-cigarettes followed for ≤12 months, used various assessment methods, and did not directly compare e-cigarette users and tobacco smokers.4 ,6 ,7 ,24 ,25 Moreover, the entire evidence on e-cigarette safety—at 6 months—is limited to 122 healthy participants, most of whom were also smoking tobacco for most of the follow-up.8 ,9 ,11 We previously reported the 12-month follow-up results26 of our 5-year study aimed at evaluating the long-term effects of e-cigarette use.27 We report the results of the 24-month follow-up, and include hospital discharge data.
Methods
The protocol and 12-month results of this prospective cohort study are reported elsewhere,26 ,27 and registered in Clinicaltrials.gov (NCT01785537). In brief, we recruited adults (30–75 years) who were: (1) tobacco smokers of ≥1 tobacco cigarette daily for ≥6 months; (2) e-cigarette users of any type of e-cigarette for ≥6 months (3) dual users of tobacco and e-cigarettes for ≥6 months, via general practitioners, e-cigarette shops, internet advertisements and social networks.
Data were collected through a structured questionnaire, administered through phone interview and/or by internet, and follow-up will continue up to 60 months. Two investigators (MEF and LM) tested carbon monoxide levels in expired breath (Smokerlyzer piCO+, Bedfont Scientific) in a random sample of those declaring tobacco smoking abstinence (25% and 50% at 12 and 24 months, respectively).
The work was approved by Chieti University Ethics Committee; all participants provided written informed consent.
Outcome variables and data analysis
The primary outcome was the percentage of sustained (30 days) abstinence from tobacco smoking at 24 months. Other outcomes were the proportion of participants abstinent from both tobacco smoking and e-cigarette use, the number of tobacco cigarettes smoked per day (and the proportion of participants reducing tobacco cigarette consumption by 50% or more between baseline and 24 months), self-reported health (assessed through the final item of the Italian version of the EuroQol EQ-D5L28) and possibly related serious adverse events. Adverse events were both self-reported and gathered from data obtained from the regional hospital discharge administrative database (Italian Scheda di Dimissione Ospedaliera) for the residents in the Abruzzo Region (46.0% of the sample); and only self-reported for the rest of the sample. The details of the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes used to extract adverse events are reported in the protocol27 and in the online supplementary material.
Supplemental material
The differences by baseline cigarette use were evaluated using Kruskal-Wallis or one-way analysis of variance with Sidak correction for continuous variables, and χ2 test for categorical variables. For the latter, when more than two categories were compared (such as for cigarette use), separate comparisons were made for one group versus the others, and different p values were computed. The difference in continuous variables (ie, number of cigarettes smoked per day) within groups between baseline and end of follow-up was evaluated through Wilcoxon matched-pairs signed-rank test.
Multivariable random-effect linear and logistic regressions, with geographical region as the cluster unit, were used to investigate potential predictors of continuous and categorical outcomes, respectively. We set eight multivariable models for the following outcomes: (A) tobacco smoking abstinence at 24 months; (B) abstinence from both tobacco smoking and e-cigarette use at 24 months; (C) possibly related serious adverse events at 24 months; (D) reduction by ≥50% of tobacco cigarette consumption from baseline to 24 months, by baseline cigarette use group (this model was fitted into two versions: the first included the whole sample of tobacco and dual users at baseline; the second included only the subsample of continuing smokers, excluding those who had quit and whose cigarette consumption was zero at follow-up); (E) reduction by ≥50% of tobacco cigarette consumption from baseline to 24 months, by 24-month cigarette use group (as most dual users switched to another group, this model and model G were needed to further investigate the potential predictors of tobacco smoking reduction among the switchers); (F) difference in the daily number of tobacco cigarettes smoked per day at 24 months compared with baseline, by baseline cigarette use group (this model was fitted into two versions: the first included the whole sample of tobacco and dual users at baseline; the second included only the subsample of continuing smokers, excluding those who had quit and whose cigarette consumption was zero at follow-up); (G) difference in the daily number of tobacco cigarettes smoked per day at 24 months compared with baseline, by 24-month cigarette use group and (H) difference in the self-rated health at 24 months compared with baseline. The users of e-cigarettes only at baseline were excluded from models D, E, F and G.
With the exceptions of models C, E and G, which included a limited number of successes and had to be fitted with a restricted set of covariates, for all other models the number of successes of categorical outcomes (excluding adverse events) approximated 10 successes for each recorded variable (thus avoiding overfitting requirements).29 It was thus decided a priori to include all recorded variables into all final models regardless of significance, unless inclusion would create multicollinearity or violate other assumptions. Each covariate was tested in its original form or transformed if needed: only the number of cigarettes smoked per day was transformed into its square root; because the results were similar to those with the covariate included in its untransformed version, it was thus kept in the model in its original form. Models A, B, D, F and H were adjusted for the following baseline characteristics: age, gender, body mass index, marital status, educational level, occupation, alcohol use, hypertension, hypercholesterolaemia, diabetes, self-rated health and years of tobacco smoking (former smoking for e-cigarette-only users). We excluded physical activity from the final multivariate models due to substantial missing data (n=41) and its virtually null effect on any dependent variables. The number of tobacco cigarettes smoked per day was transformed to be included into models A, B, C and H: because no tobacco cigarettes were smoked at baseline by e-cigarette-only users, we recategorised the amount of smoking, using tertiles. Those smoking <10 tobacco cigarettes per day (or <50 puffs per day if e-cigarette-only smokers) at baseline were assigned to the lowest tertile of consumption; smokers of 10–19 tobacco cigarettes (or 50–100 puffs if e-cigarette-only users) per day at baseline were assigned to the intermediate tertile; smokers of 20 or more cigarettes (or 100 or more puffs if e-cigarette-only users) per day at baseline were classified into the highest tertile.
Potential interactions with the dependent variable and/or quadratic/cubic terms were investigated for all covariates. In logistic regression analyses, the outlier analysis was based on Pearson calculation and standardised residuals, the change in Pearson χ2, and Dbeta influence statistics and leverage (hat diagonal matrix). The validity of the final linear regression models was assessed as follows. The assumption of constant error variance was checked graphically, plotting Pearson residuals versus fitted values, and formally, using the Cook-Weisberg test for heteroscedasticity. High leverage observations were identified by computing Pearson, standardised and studentised residuals, Cook's D influence, Welsch distance and the hat diagonal matrix (LC Hamilton. Statistics with Stata: Version 12, Eighth Edition. Boston: Cengage 2013). We found <30 influential or high-leverage observations in all models. In all cases, we repeated the analyses excluding these observations, with no substantial changes, and we thus kept all observations in the models.
We had very few missing data for all outcome variables (<5) except self-rated health, which was not answered by 56 participants at baseline (but only 30 of them were kept in the 24-month assessment), and by 3 participants at the 24-month follow-up. Models A, B, C and H were rerun without self-rated health at baseline (−30 participants), with no appreciable variation, therefore it was retained. Model H was inevitably fitted with 33 missing observations. Given that the participants lost in model H were relatively few (3.5% of the sample) and balanced across baseline groups, no missing data imputation technique was adopted. Finally, the distribution of the difference in self-rated health was relatively skewed (Shapiro-Wilk p<0.01) and model G was set also using its cubic form. However, again the estimates of p values of cigarette use covariates were similar and the dependent variable was maintained in its original form to facilitate results interpretation.
The results of the logistic regression analyses are presented as ORs and the corresponding 95% CIs whereas the results of the linear regression analyses are presented as β-coefficients and 95% CIs. A two-tailed p value of 0.05 was considered significant for all analyses, which were performed using Stata V.13.1 (Stata Corp, College Station, Texas, USA, 2014).
Results
The flow of the participants is shown in figure 1 and baseline characteristics are reported in online supplementary table S1. After 24 months, 61.1% of the 229 baseline e-cigarette-only users were still abstinent from tobacco smoking; 23.1% of the 480 baseline tobacco smokers and 26.0% of the 223 baseline dual users achieved tobacco abstinence (p<0.001 for e-cigarette-only users vs tobacco smokers or dual users; table 1). The proportion of participants who achieved complete abstinence (who were using neither tobacco cigarettes nor e-cigarettes) did not significantly differ by baseline use group: 18.8%, 17.5% and 14.3% among e-cigarette users, tobacco smokers and dual users, respectively (all p>0.05).
Main outcomes at 24 months

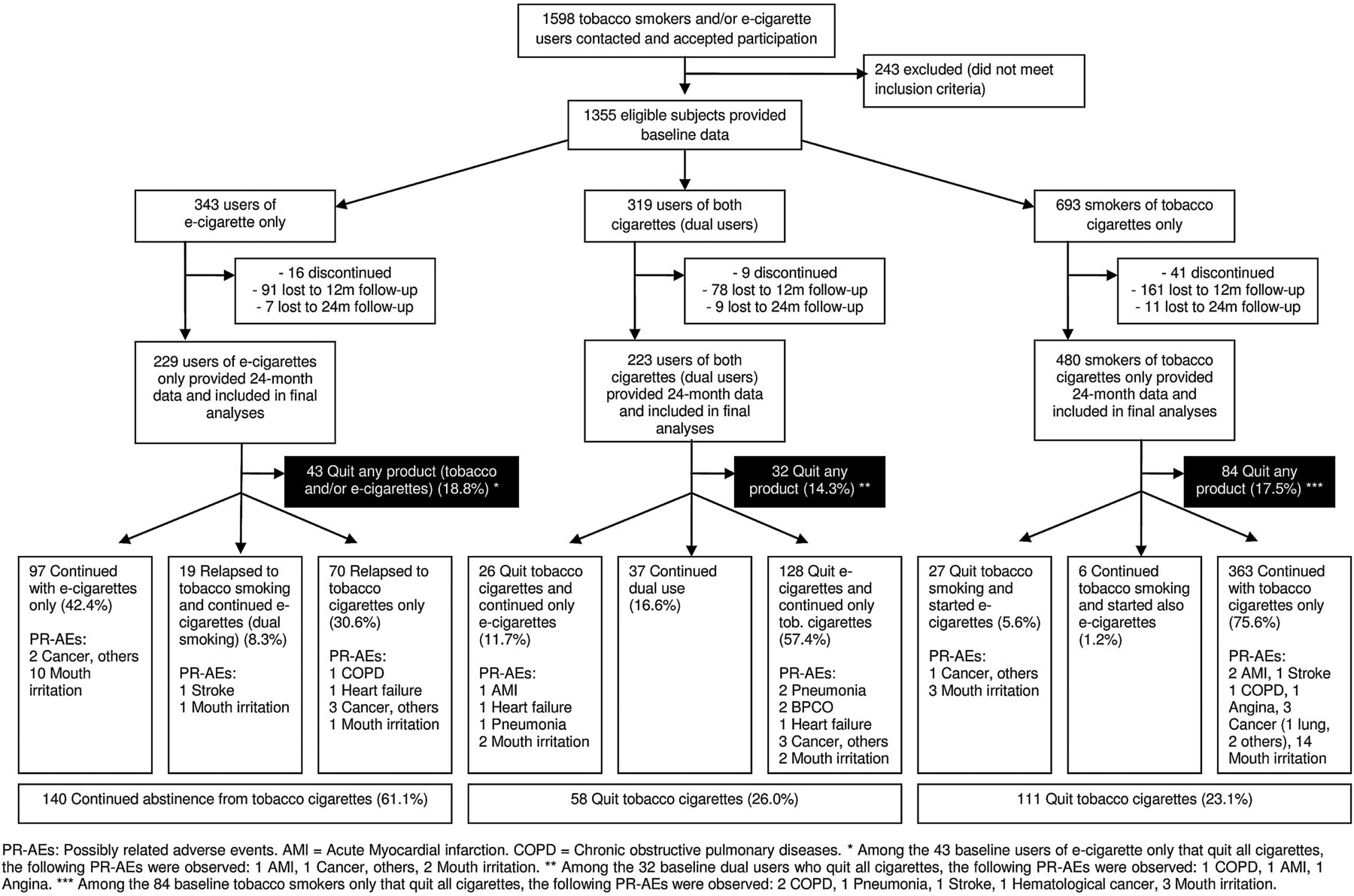{kind=link}
Flow of the participants, number of quitters and possibly related serious adverse events.
The proportion of participants reducing tobacco cigarette consumption by 50% or more, or by ≥5 tobacco cigarettes per day, and the average daily number of cigarettes, did not change by baseline group (table 1; all p>0.05). Importantly, the majority (83.4%) of dual users at baseline abandoned e-cigarettes and continued to smoke only tobacco (57.4%), or quit tobacco (11.7%) or both tobacco cigarettes and e-cigarettes (14.3%) during follow-up (table 1). Therefore, a second analysis was conducted stratifying by baseline and 24-month cigarette use, in order to assess the variation of the pattern of consumption among the switchers as well. Among the 603 tobacco-only smokers or dual users at baseline, 21 of the 40 (52.5%) participants who started or continued dual use during the follow-up reduced tobacco cigarette consumption by ≥50%, while only 67 of the 489 (13.7%) participants who started or continued only tobacco smoking showed a ≥50% cigarette reduction (p<0.001, table 1).
No significant differences in average self-rated health were noted by baseline group (all p>0.05). A substantial improvement, however, was observed for tobacco smokers or dual users who switched to e-cigarettes only (+1.1 or 1.0 in EuroQol mean score, respectively; p<0.05; table 1).
We recorded an identical number of mouth irritations (n=38) and possibly related serious adverse events (n=38; table 1). Potential adverse events were reported by 4.4%, 2.9% and 6.3% of baseline e-cigarette users, tobacco smokers and dual users, respectively (p<0.05 for the comparison of tobacco smokers vs dual users). Mouth irritation rates were 6.1%, 4.2% and 1.8% in the above groups (p<0.05 for the comparison of e-cigarette users vs dual users). The distribution of adverse events by baseline and 24-month group is reported in figure 1. The characteristics of the participants reporting a serious adverse event, and its type, are reported in online supplementary table S2. Also, the cigarette use throughout the follow-up of the 38 participants experiencing a possibly related serious adverse event is shown in online supplementary figure S1. Notably, most tobacco-only smokers at baseline, who experienced an adverse event, remained tobacco-only smokers or quit both tobacco smoking and e-cigarette use. In contrast, most of the e-cigarette-only and dual users at baseline who experienced a serious adverse event (n=24), switched group during the 24-month follow-up: 13 switched to tobacco smoking only, and 5 quit both tobacco cigarettes and e-cigarettes.
Multivariate analyses substantially confirmed univariate results (table 2): when several potential confounders were adjusted for, tobacco smoking abstinence remained significantly more likely among e-cigarette users (adjusted OR 5.56; 95% CI 3.89 to 7.95; p<0.001); the likelihood of abstinence from tobacco smoking and e-cigarette use, as well as self-reported health, did not significantly vary by baseline group (p>0.05); the probability of halving or reducing the average number of daily tobacco cigarettes smoked did not change by baseline group, but tobacco smokers who started dual use or dual users who continued dual using, were significantly more likely to halve their tobacco cigarette consumption and to decrease the average number of cigarettes per day than those who started or continued only smoking tobacco (all p<0.001); dual users at baseline remained significantly more likely to report a serious adverse event than tobacco-only smokers (OR 2.40; 95% CI 1.09 to 5.26; p=0.029).
Tobacco smoking and/or e-cigarette use abstinence or cessation, possibly related adverse events, difference in daily tobacco cigarette consumption and self-reported health: results of the multivariate analyses
Switching or quitting cigarette use
Overall, 435 participants switched (n=276; 29.6%) or stopped (n=159; 17.1%) using either product (tobacco cigarettes or e-cigarettes) during the follow-up (figure 1 and table 3). Very few tobacco cigarette smokers switched to dual use (5.6%) or to e-cigarettes only (1.3%). In contrast, only 16.6% of dual users remained dual users after 24 months, and most of them (57.4%) abandoned e-cigarettes and continued to smoke only tobacco cigarettes. Thirty-nine per cent of e-cigarette-only users switched to tobacco smoking, while 42.4% continued with e-cigarettes only or stopped using either tobacco cigarettes or e-cigarettes.
Quitting and switching cigarette use during follow-up
Of the 159 participants who quit using either product at 24 months, 91 had quit at the 12-month follow-up (57.2%). Of the 131 participants who quit using either product at 12 months, 6 were lost to follow-up, 91 remained abstinent and 34 relapsed (27.2%): 29 to tobacco smoking only, 4 to e-cigarettes only and 1 to dual use. Similar results were observed for quitting tobacco cigarettes (table 3).
Other secondary findings on CO levels, the other predictors of tobacco smoking, and abstinence from tobacco cigarettes and e-cigarettes, and adverse events, are reported in the online supplementary material.
Discussion
To date, this is the only study to directly compare smokers of tobacco cigarettes only with users of e-cigarettes only, and to provide safety data on e-cigarette-only users for >12 months. With respect to the first year of follow-up, the analyses after the second year provided some important confirmations and some new insights.
This confirms that complete switching to e-cigarettes may help tobacco quitters remain abstinent from smoking: after 24 months the rate of relapse to tobacco smoking remained relatively low (38.9%), if compared with the 60–90% relapse rates of tobacco cigarette smokers observed in population-based studies.30 It should be kept in mind that all e-cigarette users in our sample were former tobacco smokers at baseline, with a mean time of 8 months since switching to e-cigarettes. Notably, the analysis of those who had quit tobacco smoking at 12 months showed that the relapse rates to tobacco smoking at 24 months were also relatively low for tobacco-only smokers (30.3%; table 3). With regard to safety, the rate of adverse events was not lower in e-cigarette-only users than in tobacco smokers, which was expected in this phase of the study, given that the excess risk of tobacco smoking takes 1–5 years to substantially decrease.31 ,32
The results also confirmed that the use of e-cigarettes in addition to tobacco smoking (dual use) does not seem to encourage tobacco smokers to quit tobacco. Further, dual users at baseline did not differ from tobacco-only smokers in tobacco cigarette consumption and self-rated health. However, the vast majority of dual users switched to another use status during the follow-up, which suggests that dual use is generally a transient phase rather than a long-term pattern of use. Further, the analyses stratified by baseline status may provide limited information on dual users. However, when baseline and 24-month use data were considered together, we found that tobacco-only smokers who started dual use or dual users who continued dual use were significantly more likely to reduce the average number of daily cigarettes, to reduce their consumption by 50% or more, and showed a significant increase in self-rated health at 24 months compared with those who returned to or continued smoking only tobacco. Similarly, while baseline dual users showed a significantly higher probability of a serious adverse event, all these events occurred in participants who switched group during the 24-month follow-up: six stopped smoking (two of whom continued using e-cigarettes) and eight returned to only smoking cigarettes. Moreover, it cannot be excluded that, particularly for those who returned to only smoking tobacco, the previous years of exposure to smoking (23 years on average in our sample) played a greater role in developing an adverse health outcome beyond the 1-year (n=4) or 2-year (n=4) periods of dual use.
Our findings on smoking cessation and reduction rates are comparable to some previous studies,10 ,14 ,16 ,18 ,20 ,33 but different from others.11 ,13 ,15 ,17 ,18 ,33 As a potential explanation, three of the latter studies may have had less motivated samples,9 ,11 ,17 and another included some countries with an e-cigarette ban, which could affect use patterns.13 Our relapse rate to tobacco smoking among e-cigarette users doubled the estimate by Etter and Bullen16 (whose sample, however, may have been highly motivated to maintain abstinence from smoking as they were recruited from smoking cessation websites), but was much lower than the ≅94% relapse rate in the randomised controlled trial by Bullen et al.8 However, our observational study included e-cigarette users who were already abstinent from tobacco smoking for many months prior to recruitment, did not control for type of e-cigarette used and had broader inclusion criteria than some other studies (eg, included smokers of <10 cigarettes per day).
Some of our study limitations have already been reported in detail elsewhere.26 In brief, smoking cessation was partially self-reported. However, we tested CO levels in 50% of the sample in the 24-month follow-up, finding false declarations were sporadic (n=1 among e-cigarette users; n=2 among tobacco smokers). Second, we had no 24-month follow-up data for 31.2% of baseline participants. However, the loss rate is still lower than those in most previous prospective studies,9 ,11 ,14 ,16–18 and non-responders were similar to responders for most baseline variables.26 Third, we did not distinguish between different types of e-cigarettes used, and could not reliably assess frequency of use. These factors (product type and frequency of use) appear to be important characteristics predicting change in smoking behaviour.14 ,19 ,20 Finally, it has been suggested that dual users are frequently ‘quitting failures’ and thus biased against cessation.6 However, in our sample, the proportion of those who tried quitting before was quite similar between tobacco smokers (33.7%) and dual users (35.9%).
Conclusions
Overall, the first 2 years of the study confirm that switching completely to e-cigarettes might help tobacco smokers remain abstinent from smoking. The findings on dual use of e-cigarettes and tobacco smoking remain controversial: dual use did not improve the likelihood of quitting tobacco or use of e-cigarettes, but it may facilitate the reduction of tobacco cigarette consumption and improve self-rated health. Dual use also did not appear to reduce smoking quit rates compared with those of smokers not using e-cigarettes. Adverse events were still scarce, and the next years of follow-up will help clarify safety concerns, which remain the most important issue to support policies on e-cigarettes use.
What this paper adds
Despite the potential public health relevance, the current evidence on long-term safety and efficacy/effectiveness of e-cigarettes is scarce and conflicting.
After 24 months of a prospective follow-up, most users of e-cigarettes alone were able to remain abstinent from tobacco smoking.
Dual use of e-cigarettes with tobacco cigarettes did not encourage quitting tobacco or e-cigarette use, but may be helpful to reduce tobacco consumption.
Acknowledgments
Although their contribution has been substantial, some of the authors have been listed as ISLESE (Italian Study on Long-term E-cigarette Safety and Efficacy) Working Group, including Maria Rosaria Gualano (University of Turin, Italy), Giancarlo Cicolini (Local Health Unit of Lanciano-Vasto-Chieti, Italy), Giorgia Fragassi (University of Chieti, Italy), Giorgio Liguori (University Parthenope of Naples) and Stefania Boccia (Università Cattolica del Sacro Cuore, Rome). The investigators are also grateful to Dr Serena Di Sante, Giorgia Di Sante, the students of the Faculty of Medicine of Catania and general practitioners from Abruzzo (Francesco Di Silvestro, Luciano Giacci, Marino Mincone, Gabriella Salladini, Giuliano Salvio, Renato Seller, Lucio Zinni) for their help during recruitment.
References
Footnotes
LM and MEF equally contributed to the present study.
Collaborators Maria Rosaria Gualano (Department of Public Health Sciences, University of Turin, Turin, Italy); Giancarlo Cicolini (Local Health Unit of Lanciano-Vasto-Chieti, Chieti, Italy); Giorgia Fragassi (Department of Medicine and Aging Sciences, University of Chieti, Chieti, Italy); Giorgio Liguori (Department of Movement Sciences and Wellbeing, University Parthenope of Neaples, Neaples, Italy); Stefania Boccia (Institute of Public Health, Università Cattolica del Sacro Cuore, Rome, Italy).
Contributors All the authors and the collaborators participated in the design, analysis and interpretation of the study. LM, MEF, CLV, RS, WR, MFi and PV were involved in all phases of the study. MFe and CM collected baseline and follow-up data, and participated in data-analysis. LM and MEF tested CO levels, linked hospital admissions and wrote the manuscript. LM is the guarantor for all data.
Funding The first 2 years of the study were unfunded. The next 3 years of follow-up are going to be funded through crowdfunding (Kickstarter project titled ‘E-cigarette long-term efficacy & safety: a study to complete’). Besides seven authors (MEF, RS, MRG, GL, MFi, PV, CM) and seven anonymous contributors, who donated a total of €515 and €80, respectively, all other contributors are private citizens. The authors are indebted to all of them: Mattia Brescianini, Necdet Yucel, Giuseppe Prosperini, Giancarlo Cicolini, Ludovica Rotunno, Annalisa Esposito, Cristina Naccarato, Phuong Pham, Giorgia Fragassi, Giorgio Salvatore, Maria Grazia D’Agati, Giacomo Manzoli, Eliseo Torrez, Cheng Kin Phang, Ryan White, Placido D’Agati, Fabrizio Bert, Macz Yaemmaneechai, Felice Iossa, Lu Gedge, Carol Long, Patrick Murphy, Jeff Mundine, Lucia Manzoli, Martin Smith, Julien Malfroy, Taylor Darsey, Sam Lewis, Jeff George and Alexander van der Wal.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics Committee of the University of Chieti.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The raw data set is available from the corresponding author on request.