Article Text

Abstract
Introduction Benefit–cost analyses of tobacco regulations include estimates of the informed choice of smokers to continue smoking. Few studies have focused on subjective feelings associated with continued smoking. This study estimates how smoker discontent and regret relate to risk perceptions and health concerns.
Methods We analysed data from a 2015 nationally representative, online survey of 1284 US adult current smokers. Information was collected on regret, intention to quit, perceived addiction, risk perceptions and health concerns. Multivariate logistic regression adjusting for sociodemographics and health status was used to examine factors associated with smoker discontent.
Results More than 80% of current smokers report high (22.5%) or very high (59.8%) discontent due to inability to quit, perceived addiction and regret about having started to smoke. Higher levels of discontent did not vary significantly by sex, age, race/ethnicity, education or income (adjusted odds ratios (AORs) 0.5–1.2). Compared with the smokers expressing low (5.9%) or very low (3.6%) discontent, those expressing higher levels of discontent perceived their health status as fair/poor (AOR=2.3), worried most of the time about lung cancer (AOR=4.6) and felt they were more likely to develop lung cancer in the future (AOR=5.1).
Conclusion The proportion of smokers who might be characterised as having a preference to continue smoking are greatly outnumbered by addicted, discontent and concerned smokers who want to quit and regret ever having started to smoke. These discontent smokers could have a substantial net welfare gain if new regulations helped them escape their concerns about the health effects from continuing smoking.
- economics
- addiction
- public policy
- packaging and labelling
- public opinion
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Tobacco control efforts in the USA continue to advance, and the prevalence of current cigarette smoking among adults and youth are at historic low levels.1–7 Effective implementation of federal regulations of cigarettes and tobacco products under the authority assigned to the Food and Drug Administration (FDA) by the 2009 Family Smoking Prevention and Tobacco Control Act (Tobacco Control Act) is important to sustain this progress.2 8–11 FDA is required as part of the federal rule-making process to conduct an economic benefit–cost analysis of all proposed regulations.12 However, significant questions have been raised about how the benefit–cost analyses of the FDA regulation on tobacco products should be conducted.13–19 A final FDA rule requiring graphic warning labels on cigarette packaging has not been implemented in part due to concerns about the benefit–cost analysis presented in the draft rule.19–22 The benefit–cost analysis was based on widely accepted structural welfare analysis methods to quantify the utility with and without the proposed regulation.18 19 23 24 Significant concerns were noted when this analysis indicated that the potential health benefits of implementing graphic warnings on US cigarette packages should be discounted by 50% or more due to ‘lost pleasure’ (ie, consumer surplus).13–17 Leading health economists were convened by the US Department of Health and Human Services to consider the recommended methods for calculating the economic impact of potential FDA regulatory actions on cigarettes or other tobacco products.13 18 25 Subsequently, Cutler and colleagues offered four possible approaches to the contentious issue of estimating consumer surplus in benefit–cost analyses concerning addictive goods: (1) willingness to pay for cessation, (2) direct measurement of subjective well-being, (3) structural welfare analysis methods (like those used by FDA in the graphic warning labels analysis)19 and (4) rational benchmark. Of these approaches, Cutler and colleagues identified the ‘Rational Benchmark’ approach as the most feasible. The rational benchmark approach uses criterion (such as not showing high nicotine dependence and/or having completed a college degree) to identify smokers who are more likely to be well informed and acting more rationally in making an informed choice to continue smoking.25–27 In a hypothetical regulation example, this approach suggested that the utility offsets to health benefits would be much smaller, in the range of 5%–20% and likely in the lower end of this range.18 However, much uncertainty remained in calculating the economic offset ratio using structural and rational benchmark approaches (eg, with possible offset ratios shown as varying from 0% to 50%).19 25 Therefore, an alternative willingness-to-pay break-even approach was used in the recent final ‘deeming’ rule to assert FDA authority over all additional tobacco products not listed in the 2009 Tobacco Control Act, including cigars, pipe tobacco, waterpipe tobacco, electronic nicotine delivery systems and other novel tobacco products such as certain dissolvable products and gels.28 Thus, the underlying logic of assessing tobacco regulations using methods grounded in rational choice theory still remains a controversial issue.13 14 29–32 Evidence shows that both ‘enjoyment’ and ‘relief from cravings’ are often cited by smokers as the reasons they continue to smoke.33–35 However, as Schelling asserted, individuals effectively divide themselves into two conflicting selves.36 37 The current rational choice theory approach only focuses on ‘lost pleasure’ from being induced to quit by a new regulation, while many, if not almost all, smokers without the inducement would continue to suffer a net welfare loss from their inability to stop smoking: they regret having started to smoke as adolescents and worry about dying prematurely from smoking, but they feel addicted and unable to quit.13–16 29–31 38–44 While some evidence supports this position,32 there is little recent data describing which types of smokers in the USA express regret, nor how intention to quit, perceived addiction and health concerns relate to this regret.
In 2002, Action on Smoking and Health (ASH) based in the UK released a report highlighting that 83% of smokers expressed regret for having started to smoke and described smokers feeling misery, disgust and social stigma from their inability to quit smoking.45 In an editorial, Slovic reported data from an unpublished 2000–2001 survey in the USA indicating that more than 80% of current smokers reported that they would not start smoking if they had it to do over again. When asked ‘why not’, they expressed disgust and misery about their continuing smoking.30 Smoker regret in the USA has been assessed in the Gallup Poll, with 88% of smokers surveyed in 2012 indicating they wished they had never started.46 The most extensive data on regret have been reported by the International Tobacco Control Policy Evaluation Project (ITC), which has tracked a variety of perceptions among smokers in 20 countries (including feeling addicted, intentions to quit and regret over having started to smoke).40 42 43 47 Measurements of US smokers were reported across eight overlapping waves from 2002 to 2010–2011 and indicated that 88%–90% of smokers expressed regret over this period.47 However, there are only a limited number of analyses of these ITC data, with only one detailed analysis of US data from 2002.42 43 Fong and colleagues reported that 91.2% of smokers from the USA agreed or strongly agreed that they regretted having started smoking, which was consistent with the high prevalence of regret reported in the unpublished UK ASH and Slovic estimates.29 40 45 O’Connor and colleagues recently explored the relationships between smokers’ feelings of regret and other characteristics such as delay discounting and worries about future health.48 They reported that among US adult smokers completing a 2010 web-based survey, 84.4% expressed regret and that regret was positively associated with worries about the negative impact of their smoking on health, quality of life and how much they spend on cigarettes.48 Finally, we recently reported that in 2014, 71.5% of US adult smokers expressed regret and that older and non-Hispanic white smokers were most likely to report regret.44
This paper provides data from a 2015 nationally representative sample of US adult smokers that estimates the proportion of smokers who feel addicted, express an intention to quit smoking and regret having started. These three variables are evaluated together as an index of smokers’ discontent with their smoking, and we examine how this index relates to perceived addiction and concerns about the health effects of smoking. This index could be a potential rational benchmark to estimate the proportion of smokers who may experience net welfare loss from implementation of a policy or regulation.
Methods
Data were obtained from the 2015 Tobacco Products and Risk Perceptions Survey (TPRPS), a national, cross-sectional survey of US adults. The TPRPS was administered by the Georgia State University (GSU) Tobacco Center of Regulatory Science, and this study was approved by the GSU Institutional Review Board. A probability sample was drawn from GfK’s KnowledgePanel, yielding a completion rate of 75% (n=6091) after inviting a total of 8135 KnowledgePanel members. An additional 40 respondents were excluded, a priori, because they refused to answer at least 50% of the survey questions, resulting in a final survey sample of 6051 participants. For the present study, we restricted the study sample to only current smokers (n=1284). In order to adjust for sampling and non-sampling error, data were weighted using an iterative proportional fitting (ranking) procedure. Demographic and geographic distributions for sex, age, race/ethnicity, education, household income, census region, metropolitan area and internet access obtained from the March 2015 Current Population Survey were used as benchmarks for the survey weights.
Measures
Cigarette smoking status
Respondents who reported not having smoked at least 100 cigarettes in their lives were classified as never smokers. Of the remaining respondents, those who reported having smoked at least 100 cigarettes and reported currently smoking cigarettes ‘every day’ or ‘some days’ were classified as current smokers.
Nicotine dependency and perceptions and beliefs of addictiveness
Smoking level was assessed using an item that assessed how many cigarettes they smoked on an average day that they smoked. The responses were categorised as: 1–5 cigarettes/day, 6–10 cigarettes/day, 11–15 cigarettes/day and more than 15 cigarettes/day.49 Time to first cigarette was measured using ‘How soon after you wake do you use a tobacco or electronic vapor product’ with the following response choices: ‘within 5 min’, ‘6–30 min’, ‘31–60 min’ and ‘after 60 min’.50 For some analyses, responses were dichotomised into ‘equal to or less than 30 min’ and ‘more than 30 min’.51
Participants were asked if they considered themselves addicted to cigarettes, with response options: ‘not at all’, ‘yes, somewhat addicted’, ‘yes, very addicted’ and ‘I don’t know’. The ‘I don’t know’ responses, which were a small number (n=39), were excluded from the analysis. Respondents were also asked, ‘To what extent, if at all, do you agree that nicotine is the main substance in tobacco that makes people become addicted to tobacco products?’ using a 5-point Likert scale (‘strongly disagree’ to ‘strongly agree’) and ‘I don’t know’ as response choices. For this study, we recoded responses as ‘disagree’, ‘neither disagree nor agree’ and ‘agree’ and excluded ‘I don’t know’ (n=120). Finally, we assessed their craving for cigarettes by asking, ‘Do you ever have strong cravings to smoke cigarettes?’. Response options were ‘yes’, ‘no’ and ‘I don’t know’ (excluded from analysis, n=45).
Quit intention
Quit intention was assessed by asking respondents about their plan for quitting smoking cigarettes. Responses of ‘intend to quit in the next 7 days’ and ‘intend to quit in the next month’ were combined into a single group ‘Planning to quit in next 1 month’, ‘intend to quit in the next 6 months’ and ‘intend to quit in the next year’ were combined into a single variable ‘Planning to Quit in next >1 month to a year’, whereas responses of ‘intend to quit someday, but not within the next year’ and ‘never plan to quit’ were maintained as separate categories.
Smoker regret
Regret from continued smoking was assessed by responses to the question, ‘If I had it to do over again, I would not have started smoking cigarettes’, on a 5-point Likert agreement scale (‘strongly disagree’ to ‘strongly agree’). For most analyses in this study, responses were considered in three categories: with ‘strongly disagree’ or ‘disagree’ classified as not having smoker regret, ‘neither disagree or agree’ classified as neutral and ‘agree’ or ‘strongly agree’ classified as smoker regret. Respondents were subsequently asked ‘Why did you answer that way?’ in an open-ended question. To minimise response bias, questions about regret were separated from questions about health risk, quit intentions and addiction.
Perceptions of lung cancer risk
Respondents’ perceptions of lung cancer risk were assessed by three items: (1) ‘How likely do you think it is that you develop lung cancer in the future?’. Response choices were ‘very unlikely’, ‘somewhat unlikely’, ‘neither unlikely nor likely’, ‘somewhat likely’ and ‘very likely’. For analyses, ‘very (un)likely’ and ‘somewhat (un)likely’ were collapsed into unlikely or likely categories, respectively. (2) ‘Imagine the average cigarette smoker. How much higher is that person’s risk of getting lung cancer, compared to those who have never used any tobacco or electronic vapor product?’, and (3) ‘How much higher is your risk of getting lung cancer, compared to those who have never used any tobacco or electronic vapor product?’ These two items were measured using a 7-point response scale ranging from ‘about the same’ (=0) to ‘much higher’ (=6).
Respondent worry about lung cancer was assessed with, ‘How often do you worry about getting lung cancer?’. Response options were ‘rarely or never’, ‘sometimes’, ‘often’ and ‘all the time.’ Respondent knowledge about the cure rate for lung cancer was assessed with, ‘Overall, how many people who develop lung cancer do you think are cured?’. Response options were ‘less than one quarter’, ‘about one quarter’, ‘about half’, ‘about three quarters’ and ‘nearly all’.
Perceived health risks from smoking
To assess respondents’ perceptions of the health risks of smoking, they were asked to ‘Imagine that you just began smoking cigarettes [every day or only once in a while, say at parties or with friends]. What do you think your chances are of having each of the following happen to you if you continue to smoke cigarettes [every day or only once in a while]?’. For each of every day or once in a while, they rated their perceived chances of ‘lung cancer’, ‘lung disease other than lung cancer (such as COPD and emphysema)’, ‘heart disease’, ‘become addicted’ and ‘early/premature death’ on a 7-point response scale ranging from ‘no chance’ (=0) to ‘very good chance’ (=6). Responses of ‘I don’t know’ were excluded from the analyses. In order to minimise possible bias due to question order, the order of these questions was randomised. Additionally, questions about behaviours were positioned early before attitudes and beliefs were assessed.
Index of smokers’ discontent
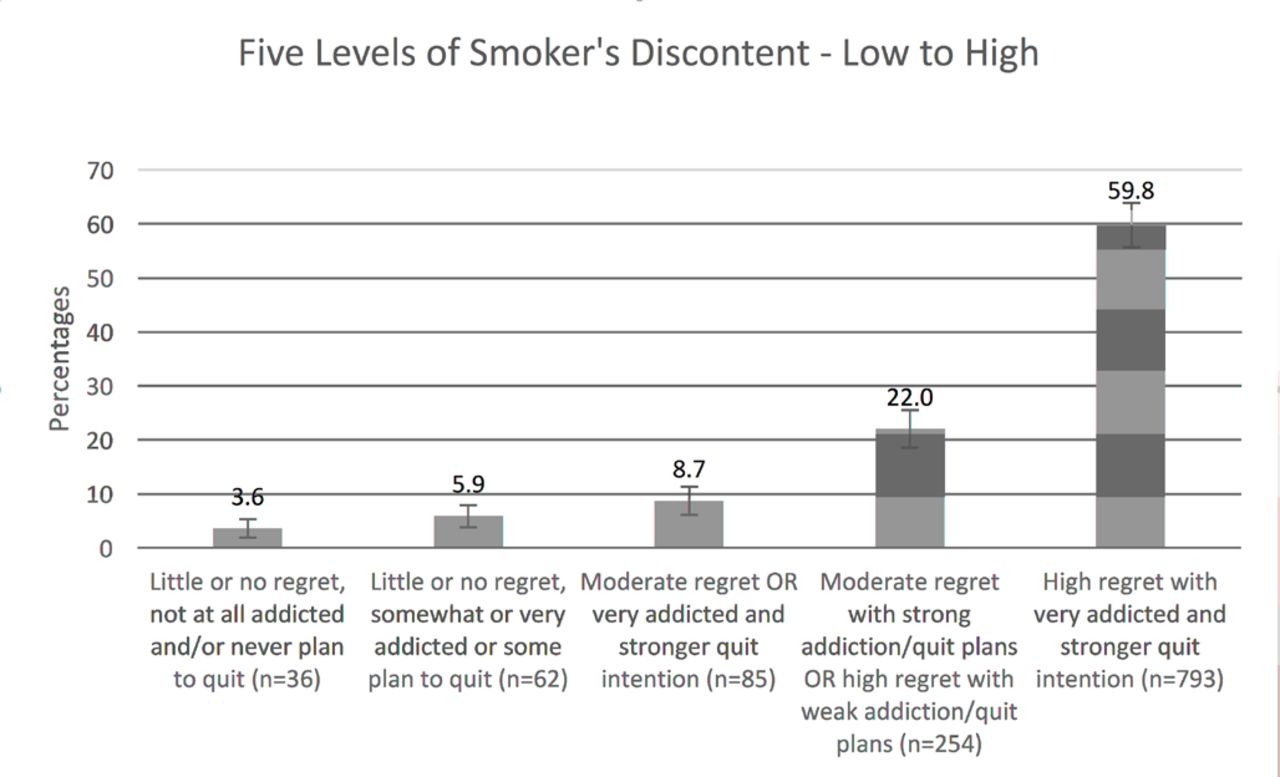
For figure 1, the responses from items smoker regret, perceived addiction and intention to quit were used to create a classification grid to assign a score from 1=low discontent to 5=high discontent (see online supplementary figure S1). Smokers who reported not having smoker regret, never plan to quit and not at all addicted or somewhat addicted, or not at all addicted and plan to quit someday were classified as low discontent. Smokers who reported smoker regret and somewhat or very addicted and planned to quit in the next year or less were classified as high discontent. The three levels of perceived addiction (1=not at all, 2=yes, somewhat addicted and 3=yes, very addicted) were combined with the four levels of intention to quit (1=planning to quit in next 1 month, 2=planning to quit in next >1 month to a year, 3=intend to quit someday, but not within the next year and 4=never plan to quit) to create a four-level Quit+Addiction code: 1=(intent to quit=1 and addiction=2 or 3); 1=(intent to quit=2 and addiction=3); 2=(intent to quit=2 and addiction=2); 2=(intent to quit=3 and addiction=2 or 3); 3=(intent to quit=1 or 2 and addiction=1); 3=(intent to quit=4 and addiction=3); 4=(intent to quit=3 or 4 and addiction=1); and 4=(intent to quit=4 and addiction=2).
Supplementary file 1

{kind=link}
Rational benchmark estimates of smoker’s discontent due to smoker regret, perceived addiction and intention to quit smoking. See online supplementary figure S1 for detailed classification of Levels of Discontent Index.
Discontent index was coded as:
1=not having smoker regret (1 and 2) and Quit+Addiction=4.
2=not having smoker regret (1 and 2) and Quit+Addiction=2 or 3.
3=not having smoker regret (1 and 2) and Quit+Addiction=1.
3=neutral smoker regret (3) and Quit+Addiction=3 or 4.
4=neutral smoker regret (3) and Quit+Addiction=1 or 2.
4=having smoker regret (4 and 5) and Quit+Addiction=3 or 4.
5=having smoker regret (4 and 5) and Quit+Addiction=1 or 2.
Sociodemographics
Respondents’ sociodemographic characteristics were obtained from profile surveys administered by GfK52 to all KnowledgePanel panellists and included self-reported sex, age, race/ethnicity, educational attainment, annual household income, region, health status and presence of children under 18 years old.
Statistical analysis
All analyses were performed using the survey procedures within SAS (V,9.3); all results reported are weighted unless otherwise noted. We estimated the weighted proportions for key variables and used the Rao-Scott χ2 test to examine bivariate associations. Weighted survey means were obtained for continuous data. Multivariate logistic regression models were estimated to examine predictors of smoker regret while adjusting for sociodemographic factors, including age, gender, ethnicity, annual income and health status. We performed data analyses with significance at P<0.05 set a priori.
Results
The smoking prevalence estimates by sex, age, race/ethnicity, US region of residence, perceived health status and presence of children under 18 years in the home are shown in online supplementary table S1A. Estimates from our surveys have been shown to agree with other nationally representative data.52
Table 1 provides estimates of smokers’ perceived addiction to cigarettes by sex, age, education, race/ethnicity, US region of residence, perceived health status and presence of children under 18 years in the home. Over 80% of smokers perceive themselves as somewhat or very addicted to cigarettes. Female, older, white non-Hispanic smokers who reported poorer health status and from households without children under age 18 years perceived themselves as more addicted to cigarettes.
Demographic characteristics by smoker’s perceived addiction to cigarettes
Table 2 provides estimates of smokers’ intention to quit smoking by sex, age, race/ethnicity, US region of residence, perceived health status and presence of children under 18 years in the home. Intentions to quit were high across the demographic categories, with about 34% (95% CI 29.8 to 37.3) planning to quit at some time, and 35% planning to quit in the next year (95% CI 31.5 to 39.0). Intentions to quit were higher among smokers with more education and higher incomes.
Demographic characteristics of current smoker by their intention to quit status
Table 3 presents the weighted percentage of respondent characteristics by smokers’ regret status measured as ‘If you had it to do over again, you would not have started smoking’. More than 70% of smokers expressed regret about having started to smoke. Smokers’ regret was high among all demographic groups and was higher among females, older and white non-Hispanic respondents and was highest among those reported a fair/poor perceived health status. Smokers self-reporting that they felt very addicted also expressed more regret (see online supplementary figure S2). Examples of open-ended responses to question about regret, ‘Why did you answer that way?’ are shown in online supplementary figure S3.
Demographic and other characteristics by smokers regret status, 2015 (n=1276)
Figure 1 displays estimates for a possible ‘rational benchmark’ groups of smokers: namely, those that might be classified as making the choice to continue smoking (ie, lack of regret, perceiving to be not addicted to cigarettes and never planning to quit) versus the discontent smokers (ie, having regret, feeling addicted and wanting to quit in the next year or less). This latter group is very large (59.8%), while those smokers who might be classified as having no regret and no plan to quit smoking is considerably smaller (3.6%).
Table 4 presents demographics, perceived nicotine dependency and perceived lung cancer risk and worry by discontent level. Respondents classified as having ‘low discontent’ (rated 1 or 2) were compared with those with ‘moderate’ (rated 3) or ‘high’ (rated 4 or 5) discontent. Adjusted ORs (AORs) were computed by multivariable logistic regression, adjusting for gender, age, race/ethnicity, household income and perceived health status. Respondents reporting having their first smoke after 30 min compared with those who smoke within 30 min are less likely to report having high discontent level (AOR=0.4, 95% CI 0.2 to 0.9). Smokers who are more likely to perceive that they will develop lung cancer in the future compared with those who perceive themselves less likely had higher odds for experiencing high discontent (AOR 5.1, 95% CI 2.2 to 12.0). Online supplementary figure S2 provides additional perceived risk for other smoking-related health conditions by discontent index. Smokers experiencing high discontent also felt they had a higher chance of early or premature death if they continued to smoke every day.
Demographic and other characteristics by smokers’ discontent level* (n=1230)
Discussion
Among this nationally representative sample of current adult smokers in the USA, only a very small proportion report they did not plan to quit sometime in the future, did not consider themselves addicted to cigarettes and did not express regret for having started to smoke. Not only do a high proportion of smokers by sex, age, race/ethnicity, education and household income commonly perceive themselves as addicted to cigarettes and express regret for having started to smoke, but these smokers rate their worry and concern as higher for dying from lung cancer and premature death. These perceptions together with the expressed negative feelings about why they regret having started smoking (see reported feelings in online supplementary figure S3) agree with what the ASH survey and Slovic have called a picture of misery.30 45 Thus, within the rational benchmark approach suggested by Cutler and colleagues as the most feasible for estimating the benefit–cost of tobacco regulations,27 the findings shown in figure 1 suggest that the proportion of smokers who might be characterised as having a preference to continue smoking would be greatly outnumbered by the addicted, discontent and concerned smokers who want to quit and regret ever having started to smoke. Furthermore, these findings suggest that the second approach considered by Cutler and colleagues, namely measuring what happens to smokers’ subjective well-being when they quit smoking, should receive greater attention. As noted by Cutler and colleagues and in recent research,27 32 there are limited cohort data showing that subjective well-being increased among smokers who quit53; however, ex-smokers do report being happier.54–59 Concerns about the methodology of quantifying such changes in subjective well-being into monetary values are relevant.60 61 However, if it is accurate, as suggested by our results, then the number of smokers who may be considered as having some net welfare loss from a new regulation is very small. The number of smokers who would have a substantial net welfare gain (even if difficult to quantify) by being helped by the new regulation in escaping the state of misery from continuing smoking is much larger. This suggests that the provisions within Office of Management and Budget Circular A-4 would justify excluding an adjustment for consumer surplus from the benefit–cost analyses of new FDA regulations of cigarettes and/or giving greater emphasis to the social welfare gains of quitting.12 14
Limitations
First, the use of the internet panel may raise concerns about sample representativeness, especially if the panel has been used in prior tobacco research. Mitigating this concern, however, is internal research by GfK that suggests minimal panel conditioning from participation in prior tobacco research.62 Second, the data are based on self-report, and biochemical verification of cigarette smoking and use of other products could not be conducted; however, the validity of self-reported cigarette smoking in surveys has been confirmed.2 63 Third, question order and placement can produce potential response bias in assessment of risk perceptions and regret. To mitigate this concern, the questionnaire was structured to separate regret assessments from other measures of risk and product use.
Conclusion
Among this nationally representative sample of current adult smokers in the USA, only a very small proportion report they did not plan to quit sometime in the future, did not consider themselves addicted to cigarettes and did not express regret for having started to smoke. Thus, these results suggest that a large proportion of smokers could have a substantial net welfare gain with new regulation that enable them to escape the state of misery from continuing smoking. Hence, estimating net welfare gain rather than consumer welfare loss should be emphasised in policy analyses.
What this paper adds
There is significant debate about how the benefit–cost analysis of tobacco regulations in the USA should be conducted.
A ‘rational benchmark’ approach has been recommended to replace the standard structural welfare analysis (eg, estimating consumer surplus or ‘lost pleasure’) grounded in rational choice theory.
Limited data are available to define preference to continue smoking based on subjective feelings of regret about having started to smoke, discontent with inability to quit and perceived risk of disease and premature death caused by continuing to smoke.
Most smokers report feeling addicted, discontent and concerned and therefore want to quit and regret ever having started to smoke. The proportion of smokers reporting no regret about having started to smoke, not feeling addicted and never planning to quit is very small.
The study findings support the inclusion of a reduction in smokers’ discontent and an improvement in subjective well-being in cost and benefit analyses of the economic impact of tobacco regulations.
Acknowledgments
The authors acknowledge the editorial assistance from Amelia Jazwa.
References
Footnotes
Contributors TFP and PN designed the study and conceptualised the data analysis. PN analysed the data. All authors contributed to interpretation. TFP, PN, SRW, PS and JH contributed to writing and reviewing drafts of manuscript. MPE assisted with the design of the parent study, reviewed drafts of the manuscript and providing critically input on design of the figures.
Funding This study was supported by grant number P50DA036128 from the National Institutes of Health, National Institute on Drug Abuse and Food and Drug Administration, Center for Tobacco Products. The author MPE receives funding from Pfizer, and all other authors of this paper report no other financial disclosures.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the Food and Drug Administration.
Competing interests None declared.
Ethics approval The study was approved by the Georgia State University’s Institutional Review Boards (GSU IRB# H14028) and Federal Wide Assurance Number 00000129.
Provenance and peer review Not commissioned; externally peer reviewed.