Mixed Methods Pilot Study of Sharing Behaviors among Waterpipe Smokers of Rural Lao PDR: Implications for Infectious Disease Transmission


Abstract
:1. Introduction

2. Methods
2.1. Study Population
2.2. Qualitative Methods
2.3. Survey Design
2.4. Statistical Analysis
3. Results
3.1. Qualitative Study
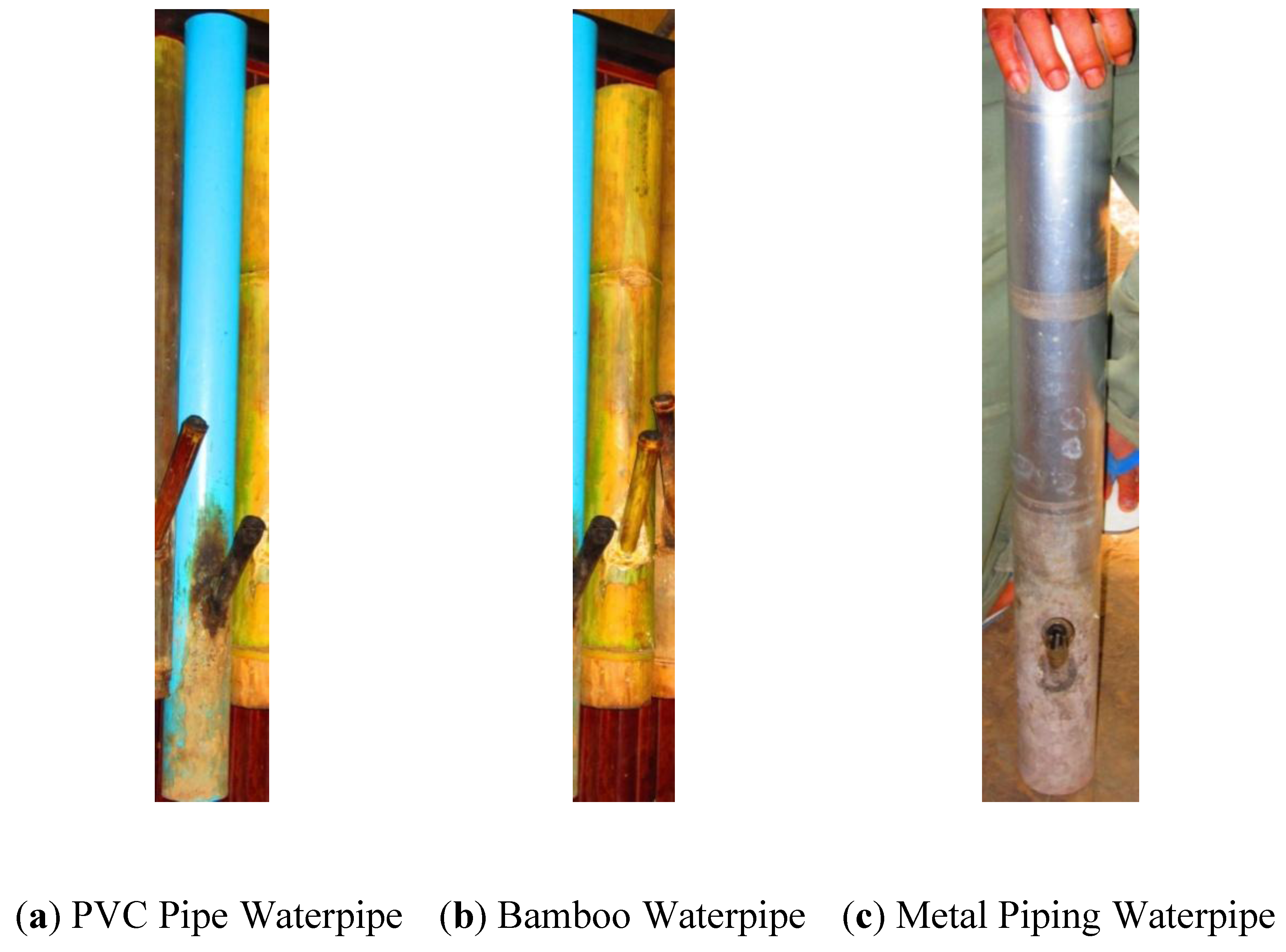
3.1.1. Waterpipe Tobacco Characteristics and Storage
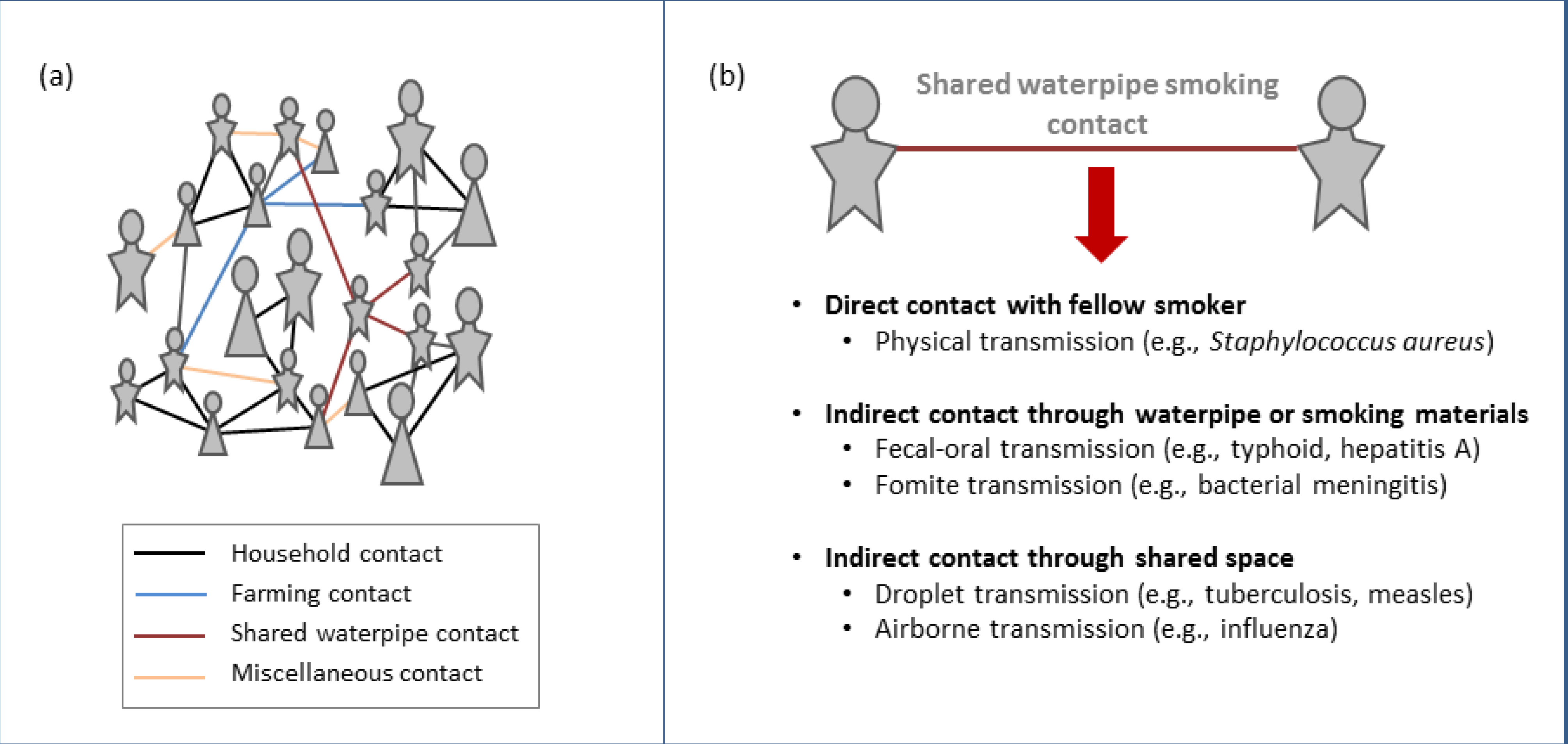
3.1.2. Sharing Behaviors
3.2. Quantitative Study

{kind=link}
{kind=link}
| N (%) | |
|---|---|
| Education | |
| No education | 29 (69.1) |
| Primary school | 12 (28.6) |
| Upper secondary | 1 (2.38) |
| Gender | |
| Male | 39 (90.70) |
| Female | 4 (9.30) |
| Marital Status | |
| Never married | 1 (2.33) |
| Married | 41 (95.35) |
| Divorced/separated | 1 (2.33) |
| Ethnicity | |
| Eui Mien | 24 (55.81) |
| Lane Tane | 3 (6.98) |
| Kouy | 14 (32.56) |
| Lao Hauy | 2 (4.65) |
| Read/Write | |
| Yes | 12 (29.27) |
| No | 29 (70.73) |
| Vocational/Technical School | |
| First level | 3 (25.00) |
| Middle level | 1 (8.33) |
| Other | 1 (8.33) |
| Don’t Know | 7 (58.33) |
| Career | |
| Government | 1 (2.38) |
| Farmer | 33 (78.57) |
| Homemaker | 7 (16.67) |
| None | 1 (2.38) |
| Home Owner | |
| Own | 40 (95.24) |
| Live w/family & pay no rent | 1 (2.38) |
| other | 1 (2.38) |
| Mean ± (sd) | |
| Age | 49 ± (13.79) |
| Type of waterpipe | N (%) |
|---|---|
| Bamboo | 39 (92.86) |
| Metal | 2 (4.76) |
| PVC | 1 (2.38) |
| N (%) | |
|---|---|
| Owner | |
| own & will share | 41 (97.62) |
| own & will not share | 1 (2.38) |
| Mean ± (sd) | |
| Number of persons shared with during last smoking session | 1.21 ± (0.54) |
| Number of persons shared with during last week | 5.24 ± (3.82) |
4. Discussion
4.1. Evidence of Infectious Disease Transmission due to Sharing Among Waterpipe Users

4.2. Implications for the Infectious Disease Burden in the Western Pacific Region
4.3. Limitations
5. Conclusions
Conflict of Interests
Acknowledgements
References
- Smoking Statistics; WHO: Geneva, Switzerland, 2002.
- Westermeyer, J. Sex differences in drug and alcohol use among ethnic groups in Laos, 1965–1975. Am. J. Drug Alcohol Abuse 1988, 14, 443–461. [Google Scholar] [CrossRef]
- Global Adult Tobacco Survey (GATS) Viet Nam; Center for Disease Control: Atlanta, GA, USA, 2010.
- Maziak, W.; Rastam, S.; Shihadeh, A.L.; Bazzi, A.; Ibrahim, I.; Zaatari, G.S.; Ward, K.D.; Eissenberg, T. Nicotine exposure in daily waterpipe smokers and its relation to puff topography. Addict. Behav. 2011, 36, 397–399. [Google Scholar] [CrossRef]
- Singh, P.; Yel, D.; Sin, S.; Khieng, S.; Lopez, J.; Job, J.; Ferrye, L.; Knutsen, S. Tobacco use among adults in Cambodia: Evidence for a tobacco epidemic among women. Bull. World Health Organ. 2009, 87, 905–912. [Google Scholar] [CrossRef]
- Knishkowy, B.; Amitai, Y. Water-pipe (narghile) smoking: An emerging health risk behavior. Pediatrics 2005, 116, e113–e119. [Google Scholar] [CrossRef]
- Jabbour, S.; El-Roueiheb, Z.; Sibai, A.M. Narghile (water-pipe) smoking and incident coronary heart disease: A case-control study. Ann. Epidemiol. 2003, 13, 570. [Google Scholar] [CrossRef]
- Akl, E.A.; Gaddam, S.; Gunukula, S.K.; Honeine, R.; Jaoude, P.A.; Irani, J. The effects of waterpipe tobacco smoking on health outcomes: A systematic review. Int. J. Epidemiol. 2010, 39, 834–857. [Google Scholar] [CrossRef]
- El-Hakim, I.E.; Uthman, M.A. Squamous cell carcinoma and keratoacanthoma of the lower lip associated with “Goza” and “Shisha” smoking. Int. J. Dermatol. 1999, 38, 108–110. [Google Scholar] [CrossRef]
- El-Setouhy, M.; Loffredo, C.A.; Radwan, G.; Abdel Rahman, R.; Mahfouz, E.; Israel, E.; Mohamed, M.K.; Ayyad, S.B. Genotoxic effects of waterpipe smoking on the buccal mucosa cells. Mut. Res. 2008, 655, 36–40. [Google Scholar] [CrossRef]
- Nuwayhid, I.A.; Yamout, B.; Azar, G.; Kambris, M.A. Narghile (hubble-bubble) smoking, low birth weight, and other pregnancy outcomes. Am. J. Epidemiol. 1998, 148, 375–383. [Google Scholar] [CrossRef]
- Tamim, H.; Yunis, K.A.; Chemaitelly, H.; Alameh, M.; Nassar, A.H. National Collaborative Perinatal Neonatal Network Beirut, Lebanon. Effect of narghile and cigarette smoking on newborn birthweight. BJOG 2008, 115, 91–97. [Google Scholar]
- Bagaitkar, J.; Demuth, D.; Scott, D. Tobacco use increases susceptibility to bacterial infection. Tob. Induc. Dis. 2008, 4, 12. [Google Scholar] [CrossRef]
- El-Barrawy, M.A.; Morad, M.I.; Gaber, M. Role of Helicobacter pylori in the genesis of gastric ulcerations among smokers and nonsmokers. East. Mediterr. Health J. 1997, 3, 316–321. [Google Scholar]
- Dar-Odeh, N.S.; Bakri, F.G.; Al-Omiri, M.K.; Al-Mashni, H.M.; Eimar, H.A.; Khraisat, A.S.; Abu-Hammad, S.M.K.; Dudeen, A.-A.F.; Abdallah, M.N.; Alkilani, S.M.Z.; et al. Narghile (water pipe) smoking among university students in Jordan: Prevalence, pattern and beliefs. Harm Reduct. J. 2010, 7, 10. [Google Scholar] [CrossRef]
- Erbaydar, N.; Bilir, N.; Yildiz, A. Knowledge, behaviors and health hazard perception among Turkish narghile (waterpipe)-smokers related to narghile smoking. Pak. J Med. Sci. 2010, 26, 195–200. [Google Scholar]
- Maziak, W.; Ward, K.D.; Afifi Soweid, R.A.; Eissenberg, T. Tobacco smoking using a waterpipe: A re-emerging strain in a global epidemic. Tob. Control 2004, 13, 327–333. [Google Scholar] [CrossRef]
- Shihadeh, A.; Saleh, R. Polycyclic aromatic hydrocarbons, carbon monoxide, “tar”, and nicotine in the mainstream smoke aerosol of the narghile water pipe. Food Chem. Toxicol. 2005, 43, 655–661. [Google Scholar] [CrossRef]
- Jani, S.R. Hookah and College Students: The Lack of Medical Guidance, a Public Policy Review, and a Campaign to Change the Trend; Drexel University: Philadelphia, PA, USA, 2009. [Google Scholar]
- Natto, S.; Baljoon, M.; Bergström, J. Tobacco smoking and periodontal health in a Saudi Arabian population. J. Periodontol. 2005, 76, 1919–1926. [Google Scholar]
- Munckhof, W.J.; Konstantinos, A.; Wamsley, M.; Mortlock, M.; Gilpin, C. A cluster of tuberculosis associated with use of a marijuana water pipe. Int. J. Tuberc. Lung Dis. 2003, 7, 860–865. [Google Scholar]
- Gajalakshmi, V.; Peto, R.; Kanaka, T.S.; Jha, P. Smoking and mortality from tuberculosis and other diseases in India: Retrospective study of 43,000 adult male deaths and 35,000 controls. Lancet 2003, 362, 507–515. [Google Scholar] [CrossRef]
- Ferry, L.H.; Job, J.; Knutsen, S.; Montgomery, S.; Petersen, F.; Rudatsikira, E.; Singh, P. Mentoring Cambodian and Lao health professionals in tobacco control leadership and research skills. Tob. Control 2006, 15 (Suppl. 1), i42–i47. [Google Scholar]
- Lao Reproductive Health Survey 2005; Committee for Planning and Investment (CPI), National Statistics Center (NSC): Vientiane Capital, Lao PDR, 2005.
- Assessing Community Needs and Resources. Windshield and Walking Surveys. The Community Toolbox; University of Kansas: Lawrence, KS, USA, 2013. Chapter 3, Section 21. Available online: http://ctb.ku.edu/en/tablecontents/index.aspx (accessed on 15 May 2013).
- Kheam, T.; Yel, D.; Singh, P.N. 2011 National Adult Tobacco Survey of Cambodia (NATSC, 2011). In Monograph: National Institute of Statistics (Ministry of Planning, Cambodia); WHO Western Pacific Region Periodical: Manila, Phillipines, 2011. [Google Scholar]
- Steentoft, J.; Wittendorf, J.; Andersen, J.R. Tuberculosis and water pipes as source of infection. Ugeskr Laeger 2006, 168, 904–907, in Danish. [Google Scholar]
- Onofre, D. Case Presentation: Hookah Smoking, A Rising Tuberculosis Health Risk Factor. Available online: www.heartlandntbc.org/casestudies/cs10.pdf (accessed on 15 March 2013).
- Hamadeh, R.; Ardehali, A.; Locksley, R.M.; York, M.K. Fatal aspergillosis associated with smoking contaminated marijuana, in a marrow transplant recipient. Chest 1988, 94, 432–433. [Google Scholar] [CrossRef]
- McPartland, J.M. Microbiological contaminants of marijuana. J. Int. Hemp Assoc. 1994, 1, 41–44. [Google Scholar]
- Verweij, P.E.; Kerremans, J.J.; Voss, A.; Meis, J.F. Fungal contamination of tobacco and marijuana. JAMA 2000, 284, 2875. [Google Scholar] [CrossRef]
- Shihadeh, A. Investigation of mainstream smoke aerosol of the argileh water pipe. Food Chem. Toxicol. 2003, 41, 143–152. [Google Scholar] [CrossRef]
- Grekin, E.R.; Ayna, D. Argileh use among college students in the United States: An emerging trend. J. Stud. Alcohol. Drugs 2008, 69, 472–475. [Google Scholar]
- Rothenberg, R.B.; Potterat, J.J.; Woodhouse, D.E.; Muth, S.Q.; Darrow, W.W.; Klovdahl, A.S. Social network dynamics and HIV transmission. AIDS 1998, 12, 1529–1536. [Google Scholar] [CrossRef]
- Klovdahl, A.S.; Graviss, E.A.; Yaganehdoost, A.; Ross, M.W.; Wanger, A.; Adams, G.J.; Musser, J.M. Networks and tuberculosis: An undetected community outbreak involving public places. Soc. Sci. Med. 2001, 52, 681–694. [Google Scholar] [CrossRef]
- Youm, Y.; Laumann, E.O. Social network effects on the transmission of sexually transmitted diseases. Sex. Transm. Dis. 2002, 29, 689–697. [Google Scholar] [CrossRef]
- Bansal, S.; Grenfell, B.T.; Meyers, L.A. When individual behaviour matters: Homogeneous and network models in epidemiology. J. R. Soc. Interface 2007, 4, 879–891. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Martin, R.; Safaee, S.D.; Somsamouth, K.; Mounivong, B.; Sinclair, R.; Bansal, S.; Singh, P.N. Mixed Methods Pilot Study of Sharing Behaviors among Waterpipe Smokers of Rural Lao PDR: Implications for Infectious Disease Transmission. Int. J. Environ. Res. Public Health 2013, 10, 2120-2132. https://doi.org/10.3390/ijerph10062120
Martin R, Safaee SD, Somsamouth K, Mounivong B, Sinclair R, Bansal S, Singh PN. Mixed Methods Pilot Study of Sharing Behaviors among Waterpipe Smokers of Rural Lao PDR: Implications for Infectious Disease Transmission. International Journal of Environmental Research and Public Health. 2013; 10(6):2120-2132. https://doi.org/10.3390/ijerph10062120
Chicago/Turabian StyleMartin, Robyn, Sahar D. Safaee, Khamphithoun Somsamouth, Boualoy Mounivong, Ryan Sinclair, Shweta Bansal, and Pramil N. Singh. 2013. "Mixed Methods Pilot Study of Sharing Behaviors among Waterpipe Smokers of Rural Lao PDR: Implications for Infectious Disease Transmission" International Journal of Environmental Research and Public Health 10, no. 6: 2120-2132. https://doi.org/10.3390/ijerph10062120