Article Text

Abstract
Background Exposure to the emissions of a tobacco waterpipe is associated with increased health risks among its users as well as those exposed to its secondhand smoke. Waterpipe use is an emerging concern to the tobacco control community, particularly among countries of the Eastern Mediterranean Region. In 2002, Qatar adopted legislation that prohibited cigarette smoking inside public venues, but exempted tobacco waterpipe smoking. To inform the development and enforcement of effective policy, the impact of cigarette and waterpipe use on indoor air quality was monitored in waterpipe cafes in Doha, Qatar.
Methods Particulate matter (PM2.5) levels were measured inside and outside of a sample of 40 waterpipe cafes and 16 smoke-free venues in Doha, Qatar between July and October 2012. In addition, the number of waterpipes being smoked and the number of cigarette smokers were counted within each venue. Non-paired and paired sample t tests were used to assess differences in mean PM2.5 measurements between venue type (waterpipe vs smoke-free) and environment (indoor vs outdoor).
Results The mean PM2.5 level inside waterpipe venues (476 μg/m3) was significantly higher than the mean PM2.5 level inside smoke-free venues (17 μg/m3; p<0.001), and significantly higher than the mean PM2.5 level found immediately outside waterpipe venues (35 μg/m3; p<0.001). In smoke-free venues, the outside mean PM2.5 level (30 μg/m3) did not differ significantly from the mean PM2.5 inside levels inside these venues (p=0.121).
Conclusions Elevated levels of particulate pollution were found in waterpipe cafes in Doha, Qatar, potentially endangering the health of employees and patrons. To protect the public from the dangers of secondhand tobacco smoke, and to change social norms around tobacco use, smoke-free policies that apply to all forms of combusted tobacco products, including the waterpipe, are needed.
- Denormalization
- Public policy
- Secondhand smoke
Statistics from Altmetric.com
Introduction
Morbidity and premature mortality associated with exposure to secondhand tobacco smoke (SHS) represent a major global public health burden, and SHS exposure arising from all sources is responsible for an estimated 600 000 premature deaths.1 The adverse health effects associated with waterpipe (WP) SHS exposure have been less well investigated compared with cigarette SHS.2 Nonetheless, evidence shows that WP SHS contains similar tobacco-related toxicants as cigarette SHS, including more than 60 carcinogens, and fine respirable suspended particles, which can be deposited deep into the lung.2 ,3 Article 8 of the WHO's Framework Convention on Tobacco Control (FCTC) requires party nations, in part, to adopt, implement and actively promote effective legislative or other measures to protect the public from exposure to secondhand smoke in indoor workplaces and public places.4 Accordingly, many nations have enacted comprehensive smoke-free legislation, in which smoking is banned in indoor, public locations.5 Such policies have been shown to dramatically reduce indoor air pollution, and are also associated with reductions in respiratory problems, heart attacks and hospital admission for asthma.6–9 Additional public health gains from smoke-free policies include increased smoking cessation among adults, and reductions in youth smoking initiation.10 ,11
In 2002, Qatar adopted smoke-free legislation that prohibits cigarette smoking inside public venues.12 Although fines ranging between QAR200 and QAR500 (approximately US$55–US$137) may be imposed, the clean indoor air law is seldom enforced in Qatar. A recent analysis of tobacco control policy measures found that Qatar has fared relatively poorly compared with other Eastern Mediterranean Region (EMR) countries in respect of smoke-free policy implementation.13 Qatar received a score of 1 (of a possible 4) for smoke-free policies, and 0 (of a possible 4) for smoke-free policy compliance, as rated by international tobacco control and public health experts using standardised criteria. Furthermore, the Qatari smoking ban law exempts tobacco WP smoking.12 In other EMR countries, smoke-free laws, where they exist, are often exempt or are silent on WP use. However, several EMR countries explicitly ban indoor WP use, including Jordan, Kuwait, Lebanon, Turkey, Saudi Arabia and Syria (although enforcement may be limited).12 ,14
Tobacco WP use has recently experienced a marked increase in popularity in Middle Eastern and South Asian countries, where it has been a traditional form of tobacco use since at least the mid-17th century.15 The tobacco WP, also often referred to as ‘shisha’ in Qatar and many Middle Eastern countries and ‘hookah’ in western countries, heats highly flavoured, moist mo'assel tobacco. One factor that may contribute to the popularity of WP use is the perception of lowered risk of WP smoking, compared with cigarette smoking.16–18 Unlike cigarettes, WP tobacco is heated rather than burnt; its smoke is passed through a water receptacle in the base of the WP, and the smoke emissions have a characteristic sweet or fruity scent.15 ,16 However, concerns have been raised recently about the health risks of exposure to WP SHS emissions, which have been demonstrated to contain many of the same toxicants as cigarette SHS, and contribute to unsafe indoor air pollution.19–23 Children and pregnant women are particularly susceptible to SHS harms,1 ,2 and at least one study has reported exposure among children to WP carcinogens and toxicants in the home.24 Patrons of WP bars have been shown to experience elevated carbon monoxide levels.25 Among adults, exposure to WP SHS is associated with increased incidence of respiratory diseases, lung cancer, low birth weight and periodontal disease.26
WP cafes are a popular venue for socialising, and WP use and the resulting emissions are a ubiquitous presence in Qatari communities. The prevalence of current (past 30-day) WP use among adults aged 15 and older is 4.9% for males and 1.6% for females.27 In comparison, the prevalence of current cigarette use is 20.2% for males and 3.1% for females. Despite a belief among 95.1% of the adult Qatari population that SHS exposure causes serious illness in non-smokers, some 12.0% of the population reported exposure to SHS in the workplace and 25.9% reported exposure to SHS in a bar or restaurant in the past 30 days.27
The success of tobacco control measures in Qatar will be strengthened by better compliance with smoke-free laws. However, objective data on indoor air quality in public venues in Qatar have not previously been reported. Air quality measurements in public venues have now been conducted among a substantial number of jurisdictions internationally to help promote smoke-free policy development and assess legislative compliance.28 The purpose of this investigation was to measure respirable suspended particulate matter of 2.5 μ or less (PM2.5), a marker for SHS, in WP cafes in Qatar's largest city, Doha. The small size of PM2.5 emissions, which arise from combusted tobacco, allow them to be easily inhaled and deposited deep within the lungs, contributing to serious respiratory and cardiovascular diseases.2 According to the Centers for Disease Control and Prevention, lowering exposure to PM2.5 emissions will reduce the risk of lung and heart diseases.29 Such data can inform the potential benefit of including WP use under existing clean air laws to policymakers and the general public, and may help to communicate the need for better enforcement of existing clean indoor air policies.
Methods
Venue selection
Indoor PM2.5 was measured in 40 WP cafes and 16 smoke-free venues in Doha, Qatar from July to October 2012. Doha is Qatar's capital and economic centre, and is home to more than 80% of the country's population.30 Venues were selected using a purposive sampling strategy to ensure a diverse mix of WP venues based on size, location and clientele. Logistical factors influenced the selection of venues, including accessibility by the research staff. The 16 control venues were selected based on their voluntary compliance with the smoke-free law, and comprised: restaurants (n=6), hospitals (n=2), retail stores (n=2), a mosque (n=1), a shopping mall (n=1), a university building (n=1), a government building (n=1), a supermarket (n=1) and a hair salon (n=1).
Materials
A TSI SidePak AM510 Personal Aerosol Monitor (TSI Inc, St Paul, Minnesota, USA) was used to measure and record PM2.5 concentration. Air is drawn into the SidePak through a sampling pump and light scattering technology is used to measure the concentration of particles with a mass-median aerodynamic diameter ≤2.5 µm. The device measures PM2.5 levels in real time and was set to record mean PM2.5 levels for 60 s intervals (a 1 min logging). A conservative calibration factor of 0.32, previously validated for cigarette SHS measurement, was applied to all data.31 The internal volume (m3) of each venue was calculated using an AEG UM 15 L Sonic Measure (AEG Elektrowerkzeuge, Winnenden, Germany).
Sampling protocol
An established indoor air quality monitoring protocol was used.31 A minimum of 30 min was spent inside each venue measuring PM2.5. Monitoring was also conducted outside each venue for 5 min, both before and after the completion of indoor monitoring. Sampling in outdoor areas was conducted within approximately 2 m of the main entrance of each venue. Windows were not open at the time of outdoor sampling to minimise the possibility of SHS drift from inside to outside. Air quality measurement was conducted inconspicuously to ensure that data collection did not influence patron and employee behaviour.
Observational data on WP and cigarette use were collected at each venue. Indoor sampling for smoking venues was conducted in a fixed location as close to the centre of the main room as could be accessed. Sampling in control venues occurred in publicly accessible areas of the premises, such as atria, hallways or dining rooms. The number of WPs in active use was counted on entry into each venue and each successive 15 min interval. A minimum of three such countings were conducted per venue, and the average number of WPs in active use was calculated. If present, the number of cigarette smokers was also counted during the same intervals.
Data analysis
PM2.5 data were averaged over the entire recording period for each venue. Differences in PM2.5 levels between venue type (smoking vs non-smoking) and environment (inside vs outside) were tested using non-paired and paired sample t tests, respectively. The active smoking density (ASD), for both WP and cigarettes, was calculated by dividing the average number of WPs in use, or the average number of cigarette smokers, by venue volume (m3). The linear relationships between PM2.5 and the ASDs for WPs and cigarettes were tested using Pearson's product moment correlation coefficient. Owing to the relatively small sample sizes and the likelihood of non-normal distributions, measures of venue volume, PM2.5 and ASD were log transformed for all statistical analyses. To enhance the interpretability of the data, back-transformed means and SDs are presented both in the Results section and graphically.
Results
Venue description and active smoking
The air quality in 40 WP cafes (smoking venues) was measured for a mean duration of 35.6 min (SD=3.7). The mean internal volume of smoking venues (365.8 m3, range=85–1449) tended to be smaller than that of non-smoking venues (682.1 m3, range=34–3120), although the difference was not statistically significant (t(52) ≤1.0, p=0.90). The smoke-free venues were monitored for a mean duration of 35.4 min (SD=8.5). Active smoking of WPs and cigarettes was observed in all 40 smoking venues with more WP smoking being observed. The mean number of WPs observed in active use was 9.4 (range=0.7–27.3), while the mean number of cigarette smokers observed was 1.5 (range=0.3–4.6). The mean WP ASD (mean=0.035 smokers/m3; SD=0.027) was significantly greater than the cigarette ASD (mean=0.006 smokers/m3; SD=0.005: t(39)=16.0, p<0.001). No active smoking (WP or cigarette) was observed inside the smoke-free venues.
PM2.5 and average smoker density
The mean PM2.5 level inside the 40 WP cafes (mean=476.1 μg/m3; SD=309.6) was significantly higher than the mean PM2.5 level found immediately outside these venues (mean=34.5 μg/m3, SD=11.6; t(39)=25.7, p<0.001). PM2.5 levels inside the smoking venues also were significantly higher than inside the smoke-free venues (mean=16.8 μg/m3, SD=12.1; t(54)=16.9, p<0.001). Mean PM2.5 levels outside the smoke-free venues (mean=30.3 μg/m3, SD=33.4) were significantly higher than the levels observed inside those venues (t(15)=3.4, p=0.003). Figure 1 shows indoor and outdoor air quality data (mean, SE), by smoking and smoke-free venues, after back-transformation from log values.

Mean indoor and outdoor PM2.5 levels, by venue type.
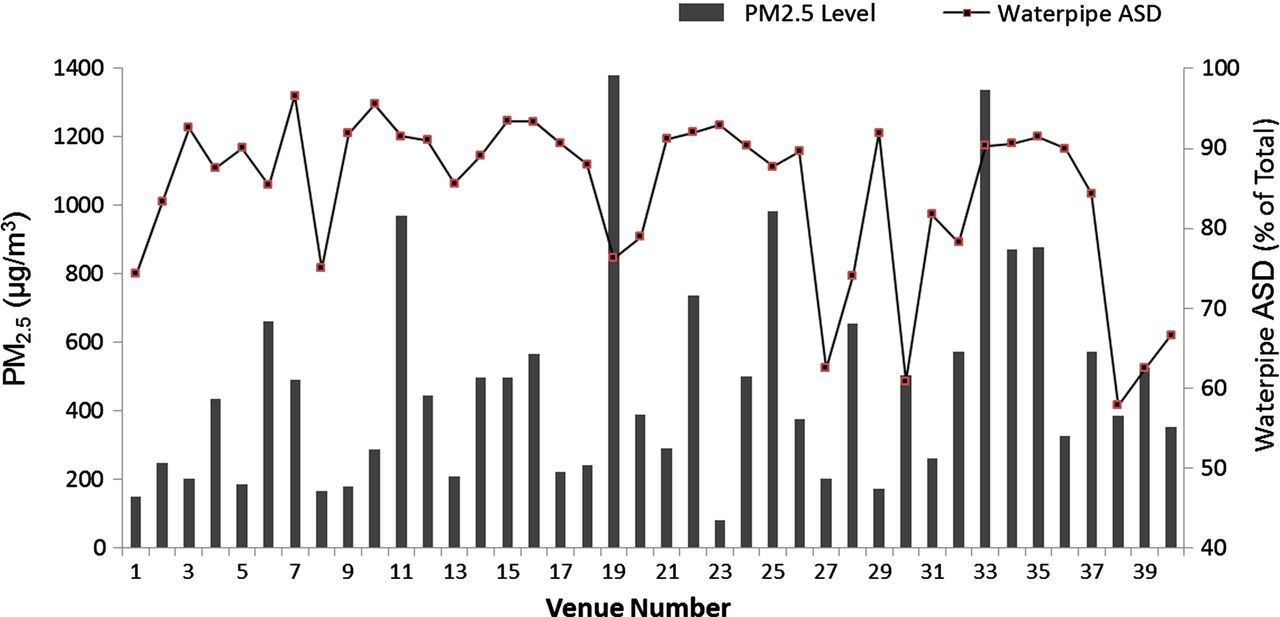
Figure 2 represents the averaged indoor PM2.5 level for each of the 40 smoking venues. Overall, the levels ranged from 81 to 1380 μg/m3. ASD for WPs ranged from 1.67 to 27.3, whereas ASD for cigarettes ranged from 0.33 to 4.67. The proportion of total ASD accounted for by WP use is depicted in the right y-axis of figure 2. This series demonstrates that the proportion of active WP smokers, as a per cent of total smokers (WP + cigarette), ranged from 58% to 97%. There was a significant positive correlation between PM2.5 levels and WP ASD (r=0.38, p=0.015), but not with cigarette ASD (r=0.20, p=0.223). ASD for the non-smoking venues was 0.
{kind=link}
{kind=link}
PM2.5 level and waterpipe active smoking density (% total), by venue.
Discussion
The mean levels of fine particulate pollution observed among a sample of WP cafes in Doha, Qatar were found to be significantly higher compared with smoke-free venues. Particulate levels were also more than 13-fold greater inside WP cafes, compared with outside these venues. To contextualise the observed PM2.5 levels, the WHO has set an air quality guideline for 24 h exposure of 25 μg/m3.32 While patrons and staff are not likely to experience 24 h exposure, exposure to the levels observed here for just a few hours a day is likely to comprise a serious health risk in the longer term. These data reveal that the exemption for WP cafes in Qatar's smoke-free legislation has resulted in environments that are unsafe for workers and the public. As such, further actions and amendments for the law are needed.
A limited number of recent studies of WP SHS emissions provide an opportunity to compare the current findings. Cobb et al22 measured PM2.5 among 17 WP cafes in Virginia, USA and found very similar levels to those reported here (mean 374 μg/m3). In Toronto, Canada, a mean particulate level of 1419 μg/m3 was found in 12 indoor venues in which WP smoking was observed.33 Moreover, Hammal et al34 observed mean indoor PM2.5 levels of 264 μg/m3 arising from the use of tobacco-free ‘herbal’ WP products. The particulate matter levels detected among WP cafes in Qatar also compare closely with those observed in non-smoke-free public venues (predominantly containing cigarettes) reported elsewhere in the EMR, and throughout the world.21 ,28 ,35 ,36
Smoke-free laws which ignore or explicitly exempt indoor WP use are common throughout the world. For instance, in the UK and the USA, a trend towards the proliferation of new WP cafes, after the implementation of smoke-free legislation exempting WP use, has been documented.37 ,38 As shown in this study, exemptions for WP cafes may limit the potential public health gains that might otherwise be realised with more comprehensive smoke-free legislation. In addition to direct protection from the harmful effect of SHS exposure,7 ,8 clean indoor air laws have also been attributed with decreasing the social acceptability of smoking.39 Social denormalisation, “the programs and actions undertaken to reinforce the fact that tobacco use is not a mainstream or normal activity in our society,’’40 has become a lynchpin of global tobacco control strategies and has helped to achieve sustainable reductions in smoking.15 ,18 ,41 The present data provide further evidence for the need for smoke-free legislation that is comprehensive in its scope. The failure to include WP smoking in the clean indoor air legislation of many countries and jurisdictions may be due to a number of reasons. Compared with cigarette smoking, WP use is perceived as relatively low risk.17 ,18 Such beliefs may also contribute to a perception that WP SHS does not pose health risks. While scant research is available on public attitudes towards WP SHS, one survey of American WP smokers found that a large majority either did not believe or did not know that WP SHS was harmful.17 Indeed, until recently, there have been very little data available to document the negative impact of WP emissions on air quality. In EMR countries, WP use has long-standing cultural and social significance, and lack of public support for bans on indoor WP use may have limited the development of new or amended laws. In western countries, the recent, rapid increase in the popularity of WP use so far may have exceeded the capacity of policymakers and legislators to respond. The present data provide an important evidence base for the implementation of clean indoor air laws that should include WP use. In many EMR countries, such as Qatar, where WP use is a popular social activity, such legislation may help to promote a change in social norms, just as it has helped change public perceptions of cigarette use in western countries.18 ,41
In 2013, after the completion of data collection for the present study, the Qatari Supreme Council of Health started working on introducing amendments to the smoke-free law of 2002. The amended smoke-free law is intended to provide more comprehensive protections and will prohibit all types of indoor smoking in public places, including WPs, and increase fines for non-compliance. Further, Qatar has succeeded in banning tobacco advertisements and promotions. These actions provide an excellent opportunity to ensure that implementation and enforcement of the new law is performed optimally. Future research should investigate the short-term impact of banning WP smoking on air quality and SHS exposure, and, in the longer term, the potential for changes in social norms and the relationship to the prevalence of use and health outcomes.
Several limitations to these findings should be noted. The use of a convenience sample may limit the generalisability of these results. Second, the method used to measure PM2.5 does not differentiate between sources of particulate matter, and so cannot distinguish WP from cigarette emissions or non-tobacco sources. For instance, cooking and ambient pollution may have contributed to particulate levels. Control venues may have had limited capacity to resolve this problem owing to their fundamentally different use designations: smoking venues often served food prepared on the premises (and thus generate PM2.5 from non-tobacco sources), while control venues usually did not. Finally, in the absence of an established calibration factor specific to WP SHS measurement with the SidePak, a calibration factor of 0.32 was applied to all data, which has been experimentally determined for cigarette SHS.28 ,31 While unpublished research has determined 0.37 to be a suitable calibration factor for WP SHS,42 we elected to use the conservative 0.32 calibration factor, which may have led to an underestimation of PM2.5 levels.
The current investigation adds to the growing literature on the contributions of WP SHS on indoor air quality. Qatar has demonstrated its intent to protect the public from the dangers of SHS by enacting its smoke-free legislation, and by ratifying the FCTC. However, SHS remains a major contributor to elevated levels of PM2.5 in WP cafes. Comprehensive smoke-free legislation, which applies to all venues and for all combusted tobacco products, is a welcome development in the tobacco control policy of Qatar. If implemented and enforced appropriately, the experience of Qatar may serve as an example to the wider EMR.
These data provide further evidence for policymakers that indoor WP use threatens to undermine the potential benefits of tobacco control policies in the Middle Eastern region and other countries in which WP use is a popular practice. Comprehensive indoor smoking bans, which do not exclude WP use, are needed to address a significant flaw in the smoke-free laws of some jurisdictions.
What this paper adds
Data on waterpipe emissions in public places are limited, and no studies have documented waterpipe secondhand tobacco smoke in Qatar. This study reports the first known research on secondhand smoke emissions in public places in Qatar, and the first report of indoor air quality among a sample of waterpipe cafes in Qatar.
This work adds to the limited yet growing body of evidence on the contributions of waterpipe secondhand smoke to unsafe indoor air quality.
The findings of this research have implications for the broadening and enforcement of Qatari smoke-free law, as well as laws in other countries in which waterpipe use is exempted from smoke-free laws.
Acknowledgments
This work was supported by Action on Smoking and Health International, and Hamad Medical Corporation Research Center.
References
Footnotes
Correction notice This article has been corrected since it was published Online First. Hamad Medical Corporation Research Center has been added to the Acknowledgements.
Contributors All authors contributed to the conception, design and interpretation of the data. VWR and ABS conducted data analyses. All authors contributed to the drafting of the article and critical revisions for important intellectual content and also approved the final manuscript.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Research data are available for sharing and will be made available to qualified researchers on application to the corresponding author.