Article Text

Abstract
OBJECTIVE Experimental evaluation of comprehensive community wide programme to prevent adolescent tobacco use.
DESIGN Eight pairs of small Oregon communities (population 1700 to 13 500) were randomly assigned to receive a school based prevention programme or the school based programme plus a community programme. Effects were assessed through five annual surveys (time 1–5) of seventh and ninth grade (ages 12–15 years) students.
INTERVENTION The community programme included: (a) media advocacy, (b) youth anti-tobacco activities, (c) family communications about tobacco use, and (d) reduction of youth access to tobacco.
MAIN OUTCOME MEASURE The prevalence of self reported smoking and smokeless tobacco use in the week before assessment.
RESULTS The community programme had significant effects on the prevalence of weekly cigarette use at times 2 and 5 and the effect approached significance at time 4. An effect on the slope of prevalence across time points was evident only when time 2 data points were eliminated from the analysis. The intervention affected the prevalence of smokeless tobacco among grade 9 boys at time 2. There were also significant effects on the slope of alcohol use among ninth graders and the quadratic slope of marijuana for all students.
CONCLUSION The results suggest that comprehensive community wide interventions can improve on the preventive effect of school based tobacco prevention programmes and that effective tobacco prevention may prevent other substance use.
- smokeless tobacco
- primary prevention
- intervention studies
- adolescent behaviour
- community interventions
Statistics from Altmetric.com
This paper presents results of Project SixTeen, a randomised controlled trial of a community intervention to prevent adolescent tobacco use. The project tested whether a comprehensive community wide effort to prevent adolescent tobacco use would have a greater deterrent effect on tobacco use than a school based tobacco prevention programme alone.
School based tobacco prevention programmes appear to have significant, though limited, impact on the prevalence of adolescent tobacco use. In a meta-analysis that controlled for discrepancies between the unit of analysis and the unit of experimental assignment, Rooney and Murray found that the average effect size for school based programmes was only 0.10 standard deviation units.1
The limited efficacy of these programmes is not surprising. Schools are only one channel through which to reach young people, and they cannot be expected to affect all of the influences on adolescent tobacco use.2 They may have a limited impact on peer influences to use tobacco, may have little or no effect on parental efforts to prevent youth tobacco use, and provide only a small counterweight to the steady drumbeat of tobacco company promotion.
We therefore developed and evaluated a comprehensive community intervention to prevent adolescent tobacco use. Its components targeted the key social influences on adolescent tobacco use. “Media advocacy” was designed to make the prevention of tobacco use a higher priority for community members. The “youth anti-tobacco” module consisted of diverse youth activities designed to influence youth not to use tobacco. “Family communications” activities were designed to mobilise parental influences for young people to not use tobacco. The “access” component involved a systematic campaign to reduce illegal sales of tobacco to youth.
There have been several other reports of smoking prevention programmes that involved community interventions. Pentz, Johnson, and colleagues3 4 reported the evaluation of a comprehensive community intervention to affect tobacco and other substance use. They found that combining school based programmes with mass media and programmes aimed at parents and community leaders can have a greater effect on tobacco and other substance use than providing mass media and parent and community organising alone.
Perry and colleagues compared two communities, one of which received the Minnesota Heart Health programme targeting adult cardiovascular health plus a three year classroom based prevention programme that began when students were in grade 6 (age 11–12).5 The other community did not receive any intervention. Students in the intervention community had a significantly lower prevalence of smoking at each year of assessment, through grade 12 (age 17–18).
The North Karelia Project6 was a community wide comprehensive cardiovascular risk reduction programme. In the context of that programme, an intensive classroom based smoking prevention programme was provided to students in two schools. Training and materials were provided to the rest of the schools in the county, but project staff did not provide the intervention in these schools. Changes in smoking in the two target schools and two other schools in the county were compared with changes in two schools in a county that received no intervention. Two years after the initiation of the programme, the two targeted schools had significantly lower increases in smoking prevalence than did students in the schools in the comparison county.
None of these studies employed a true randomised design in which whole communities were randomly assigned to conditions. Moreover, none of the studies tested whether community intervention elements added to the effect of a school based programme alone. Thus, an experimental evaluation of whether a comprehensive community intervention can improve on the effects of school based prevention programmes is needed.
Method
DESIGN
The design of the current study is shown in fig 1. It was a randomised controlled trial in which small Oregon communities were assigned to one of two conditions (see below).
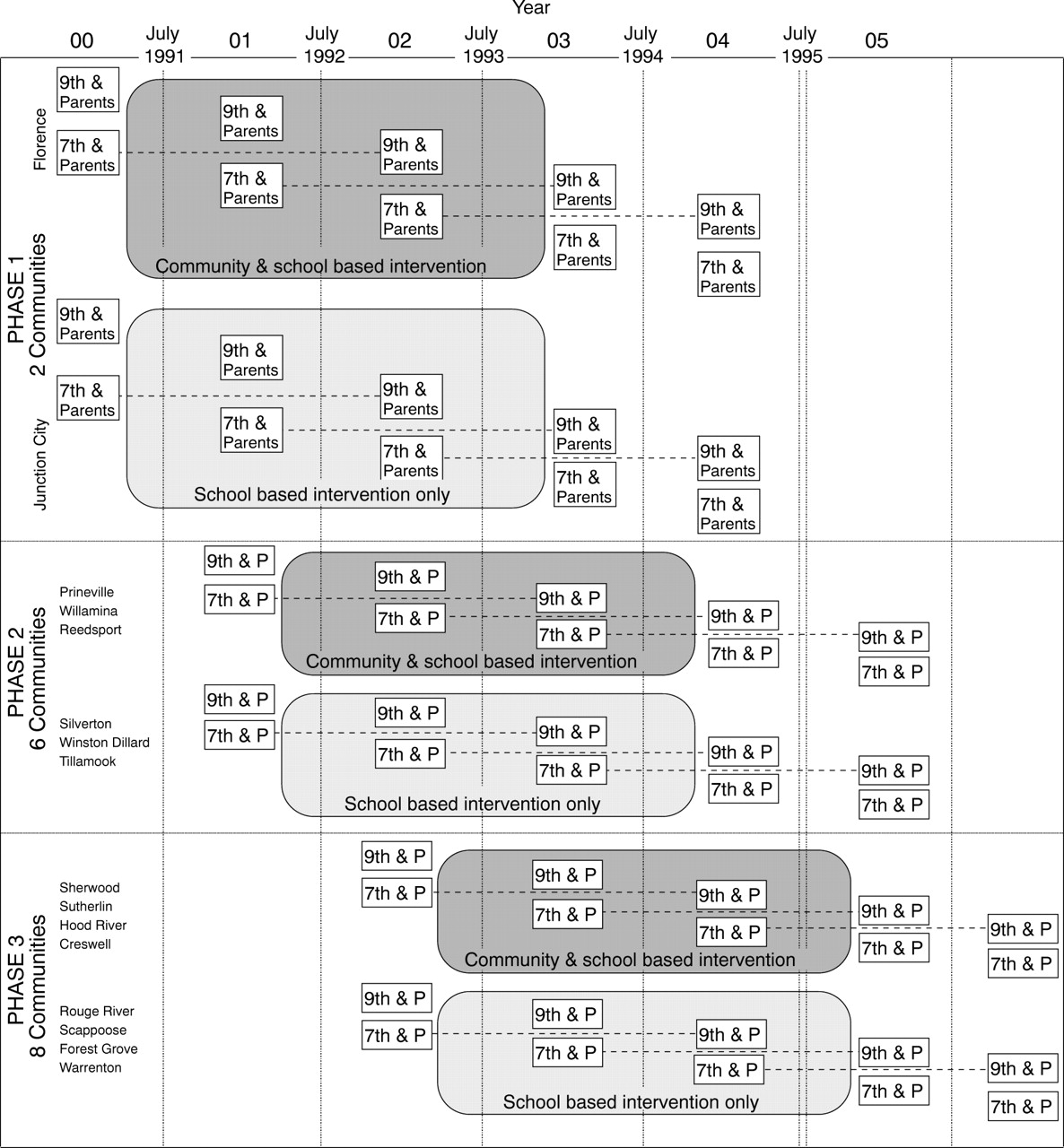
Experimental design for Project SixTeen showing assessment sequence, intervention interval, and study sample cohorts.
The population of these communities ranged from 1700 to 13 500. The principal economic activities are tourism, logging, fishing, and farming. Communities were selected such that the possibility of contamination between communities was minimised. The communities share no common high schools and are at least 20 miles apart. In order to participate, school districts agreed to implement the school based intervention and to permit the in-school assessment sequence shown in fig 1.
Pairs of communities were matched on community socioeconomic status and population. One member of each pair was assigned at random (via the flip of a coin) to receive a school based tobacco and other substance use prevention programme (school based only ( SBO) condition) in grades 6 through to 12. The other member received a community intervention programme in addition to the school based programme (CP condition). Communities in the two conditions did not differ statistically in size, per capita income, median household income, the percent of people below the poverty level, the proportion of minority students, the number of high school students per grade, or the proportion of high school graduates in the population.
Implementation of the design was carried out in three phases to allow refinement and streamlining of intervention procedures and to minimise demands on project personnel.
PARTICIPANTS
The primary method of comparing the effects of the two conditions was through the assessment of successive cross sectional samples of age eligible seventh and ninth graders (ages 12–13 and 14–15, respectively). The first year data (time 1) served as a baseline and data from the second, third, fourth and fifth years (time 2–5) of the study were used to assess the relative effects of the SBO and CP conditions. A passive consent procedure7 was used in which parents were sent letters describing the planned surveys; they could send in a postcard if they did not want their child assessed. Expired air carbon monoxide samples were obtained from all students. In addition to providing a measure of smoking, they have been shown to increase the accuracy of self reports about smoking.8 9 Table 1 presents the proportion of young people from whom we obtained data in each year of the study, broken down by condition and grade. Across all assessments, grades and conditions, 7% were not assessed because parents declined, 2.5% were not assessed because the student declined to participate at the time of the assessment, 4.0% were absent and were not available when absentee assessments were done, 0.2% were missing for unknown reasons, and 0.6% had dropped out of school.
Proportion of students assessed in Project Sixteen schools by time, condition, and grade
To assess intervention effects on parents, we obtained data from a 30% random sample of parents of the seventh and ninth graders we assessed. A questionnaire was mailed to them, with a $10 bill enclosed as compensation for completing the questionnaire. This was followed by two follow up reminder mailings and a reminder phone call. For seventh grade parents, the percent of parents who returned a questionnaire averaged 78.6% across the five years (91%, 81%, 77%, 73%, and 70.9% for times 1–5, respectively). For ninth grade parents, the return rate was 78.4% (84%, 78%, 79%, 73%, and 78% for times 1–5, respectively).
Table 2 presents descriptive data regarding the seventh and ninth grade students who were assessed at each of the five time points reported in the study. It also presents data on the parents of seventh and ninth graders.
Characteristics of participants (n (% of sample))
MEASURES
Data were collected from young people in annual school surveys. A questionnaire asked about tobacco and other substance use, other problem behaviours, associations with deviant peers, and family relations. Items were derived from prior work conducted by Patterson and colleagues at the Oregon Social Learning Center10 and by our own group.11 12
An index of weekly smoking was composed based on answers to questions about smoking. One item was developed for National Cancer Institute (NCI) trials of school based tobacco prevention programmes. It asked the respondent to indicate level of smoking, with 10 choices ranging from “never smoked, not even a puff” to “a few times each month” to “a pack or more each day”. Respondents also were asked how many cigarettes they had in the past month, past week, and past day. In order to produce an index of smoking in the last week, responses to each item were scaled to weekly smoking. The NCI item was scaled to approximately the value each item implied for the rate of weekly smoking following a procedure developed by Pechacek and colleagues.13 Monthly smoking was divided by 4.3 and daily smoking was multiplied by 7. These four items were then averaged to produce an index of weekly smoking. Any participant whose score on this index exceeded 1 was categorised as a smoker.
Similar indices were developed for smokeless tobacco use, alcohol use, and marijuana use. In all three cases, responses to questions about use in the last month and last day were scaled to weekly use and averaged with responses to questions about use in the last week. Participants whose score exceeded 1 on these indices were categorised as users of each substance.
Samples of expired air carbon monoxide were also collected. We created a net carbon monoxide score from the difference between expired air and ambient classroom air.
We obtained data on variables that might mediate the effects of the community intervention on tobacco and other substance use. There were two ratings of adolescents' exposure to the intervention: exposure to information about smoking cessation or prevention and (beginning at time 2) awareness of efforts to reduce illegal sales of tobacco to minors. We also assessed the more proximate impact of the intervention, including adolescents' attitudes toward tobacco use, their intentions to smoke, their intentions to chew (among males only), their friends' smoking, and general deviance of their friends.
We also obtained measures of intervention mediators from parents. Measures of their exposure to the intervention included parent ratings of the extent of community efforts to prevent youth access to tobacco, community support for tobacco access restrictions, community support for tobacco prevention in general, and ratings of how supportive they thought the schools, government leaders, and business had been of tobacco prevention. We asked about perceived support of alcohol and other drug prevention. Since we did not focus explicitly on these issues, this item should not have changed as a function of the intervention. Measures of the impact of the programme on parents included parent reports of whether they had talked about youth tobacco issues with another parent and whether they had joined a network of parents who opposed tobacco use.
INTERVENTIONS
School based only (SBO) intervention
Project Programs to Advance Teen Health (PATH)14 was designed as a school based programme focused on deterring students from using tobacco and other substances. In a randomised controlled trial, there was evidence that the PATH curriculum, when compared to existing standard health education curricula, reduced the rate of cigarette smoking among adolescents who reported cigarette use before the intervention.11
The curriculum consists of nine levels of instruction. The first four levels were developed for use in grades 6 to 9 (ages 11–15). They included materials and videos designed to complement the health education programmes in those grade levels. The other levels, developed for the high school curriculum, were designed to address issues relating to tobacco in health, social studies, biology, and English classes. The basic PATH health curriculum is presented in five sessions over a one week period. Specific curriculum components include: (a) health facts and the effect of smoking; (b) refusal skills training for dealing with the social pressures to smoke, chew, use illegal drugs, or engage in antisocial behaviour; (c) video assisted instruction in presenting key concepts and modelling refusal skills; (d) public commitment activities allowing students to clarify their opinions regarding tobacco use; and (e) peer led discussions and skills practice activities. Teacher training was conducted by project staff in a single session lasting 2–3 hours. Training consisted of reviewing each activity, watching excerpts of the videotapes that are shown to students, and practising or role playing teaching activities.
The school component was delivered in each year of the intervention in grades 6 to 12. We did not require that the classroom programme be continued after the end of the intervention. However, the materials continued to be available to teachers if they wanted them, and we continued to serve as a resource to teachers upon their request.
Community programme (CP)
The CP intervention was conducted by a paid community coordinator and youth and adult volunteers from the community. The community coordinators were funded to work 1.0 full time equivalent during the first year and 0.75 for the remaining two years.
Each component of the intervention was defined by a written module that provides a menu of activities and instructions on how a particular activity can be implemented. The activities are ones that existing empirical evidence, or prior experience in other communities, suggested would affect a particular facet of the social influences on adolescent tobacco use.
The Media advocacy module was created by the Advocacy Institute for the NCI.15 It provided a set of strategies for publicising the tobacco problem. They were used to influence adults in the community to support efforts to prevent adolescent tobacco use. Activities included newspaper articles and presentations to local civic groups. In seven of the communities, one page bulleted fact sheets about the problem of adolescent tobacco use were mailed to community leaders about once every two months. Other activities included printing of messages on sports programmes (four communities), paid ads or public service announcements on the radio (four communities), billboards at sports fields (two communities), and written messages on local cable access “reader boards” (four communities). The level of these activities in CP communities were monitored through weekly reports from community coordinators. The data were used as a management tool in trying to maintain a high rate of communications to as many adults in the community as possible.
The Youth anti-tobacco module 16 17 was designed to assist community coordinators and youth in developing anti-tobacco activities that are engaging and persuasive to young people. Rather than prescribing activities for the community, the module presents a menu of activities. Community coordinators and youth were encouraged to use specified activities, to adapt them to their situation, or to make up entirely new activities. Thus, over time, the menu of activities grew, as each community modified existing activities or created new ones. The activities can be classified into eight categories: planning, creative (for example, sidewalk art, T shirt design), policy review and revision, trade-ins (tobacco promotion items traded for anti-tobacco items), give aways (for example, T shirts, posters, stickers, balloons), games (for example, a “knock down Joe Camel” booth at a health fair), academic (presentations by community coordinators in classrooms, peer run quizzes), and other (for example, participation in parades). An effort was made to recruit young people who seemed particularly at risk from using tobacco.
The Family communications module 17 18 consisted of activities designed to get parents to communicate to their children that they did not want them to use tobacco. In the first year of intervention, pamphlets were distributed to parents through the schools or civic organisations. The pamphlets advocated preventing tobacco use and suggested rules and consequences for children's tobacco use. In four communities, students in middle schools gave their parents a tobacco quiz that was designed to prompt non-coercive parent–child discussions about not using tobacco. In a fifth community, this activity was conducted among grade 9 students. In two of the communities the parent–child quiz was preceded by a letter signed by numerous prominent local citizens that told about the quiz and gave the answers to each of its questions. It also contained information collected in prior surveys about the degree to which parents in their community were opposed to young people using tobacco. Biglan and colleagues provide a full exposition and experimental evaluation of the youth anti-tobacco and family communication modules.17
The ACCESS module 19 consisted of a five component programme to decrease the proportion of stores selling tobacco to minors. The components are: (a) mobilisation of community support; (b) merchant education; (c) rewards to clerks for not selling and reminders to those who sell; (d) positive publicity about clerks' refusals to sell; and (e) feedback to store owners or managers about the extent of their sales to adolescents. This component of the intervention was typically implemented in the first year of the intervention. Reward and reminder visits occurred every two or three weeks until the rates of illegal sales had been substantially reduced. Their frequency was then curtailed, though they continued over the duration of the intervention. The programme was found to decrease sales notably in the first four CP communities in which it was evaluated,20 and those effects were replicated in the other four CP communities.21
During the course of the study we developed a system for community coordinators to provide weekly reports of their work on each of the youth anti-tobacco, family communications, and access activities. Although these records are not available for the first 6–10 months of the intervention in three of the communities, they provide some sense of the relative effort devoted to each component. The most frequent activities were youth anti-tobacco activities. Across the three years of intervention activity, the community coordinators reported an average of 10.12, 13.63, and 12.12 youth anti-tobacco activities per month. They reported 3.2, 2.9, and 1.9 youth access activities per month. Finally, 3.9, 1.6, and 0.8 family communications activities were reported each month.
Results
OVERVIEW OF ANALYSIS
We began by examining the effect of the intervention on the slope of the prevalence of each dependent variable, using a set of random coefficients analyses for nested cross sectional designs.22 Individual students are nested within the community and effects are measured using community level means as the unit of analysis. This analysis involved examining the prevalence of the behaviour in each community across five time points. In the initial analysis, sex and grade (7 v 9) were included as factors along with time and intervention condition. If tests of the interactions of grade and sex with the time by condition interaction were not significant (indicating that there were not differential intervention effects depending on sex, grade, or their interaction) we dropped the interactions from the analysis. The following individual level covariates were included in the analysis when they accounted for significant variance in the dependent variable: (a) parent separation, (b) number of biological parents lived with, (c) student reported grade point average, (d) self reported frequency of homework completion, (e) educational aspirations, (f) mother's smoking, and (g) father's smoking.
If the effects of intervention on the slopes of the dependent variable were not significant, we conducted pair wise analyses of the effects of the intervention from time 1 to times 2, 3, 4, and 5, respectively. The analyses included time, condition, grade, and sex, with individuals nested within communities. As in the analysis of slopes, the non-significant interactions not germane to the effects of the intervention were dropped from the analysis. The covariates were the same as above.
TOBACCO USE
Prevalence of smoking
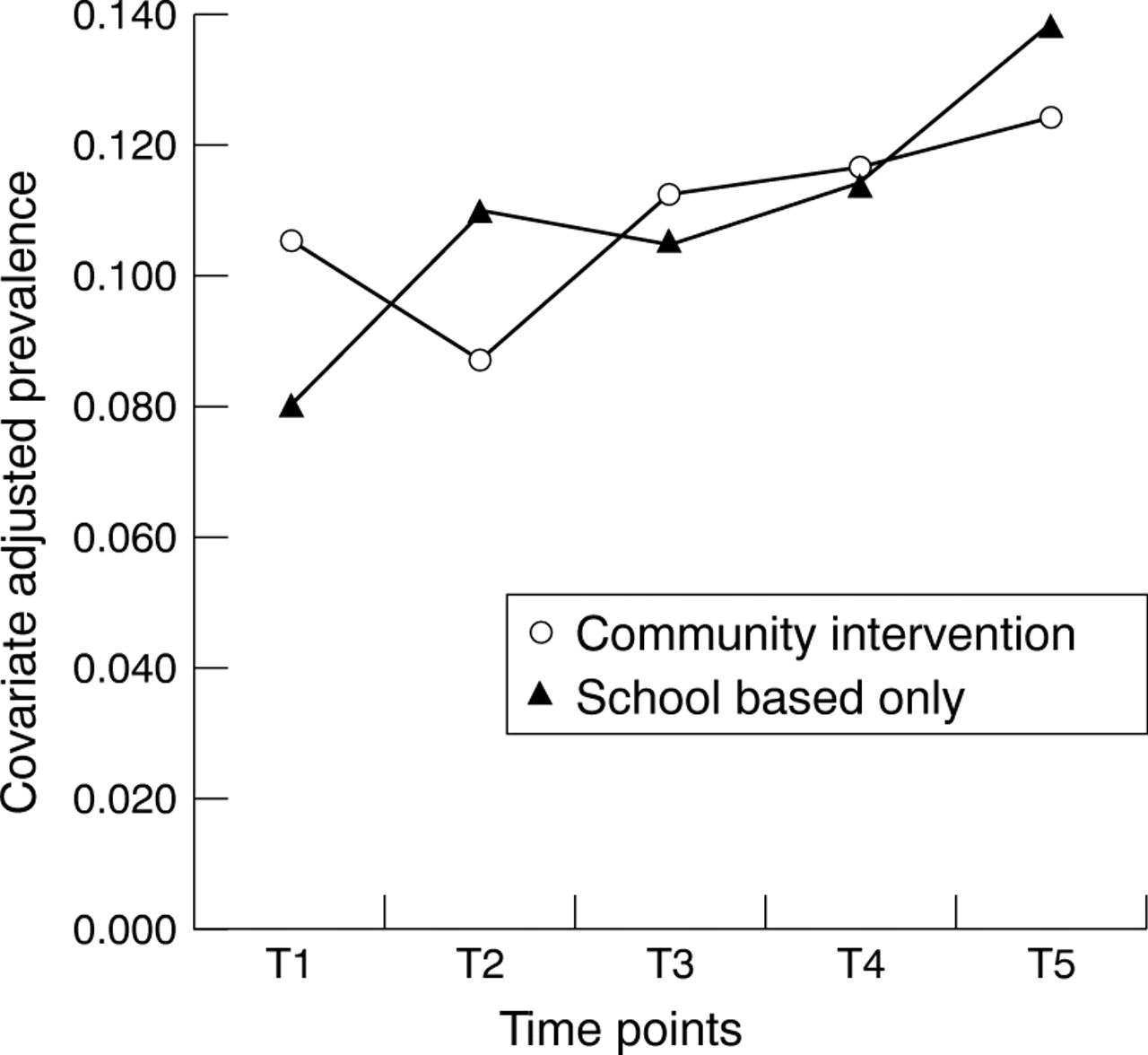
Figure 2 presents the mean prevalence of smoking in the past week in each condition at each time point. The random coefficients analysis for smoking prevalence was not significant. Analyses of the effects of the intervention, however, were significant at times 2 and 5 and approached significance at time 4 (p = 0.077, two tailed test). Table3 presents the effect at each time point. The effect shown is the difference between the change in prevalence from time 1 to the relevant time point for the CP condition minus the same change for the SBO condition. Thus, a positive value indicates that there was a more favourable change in prevalence for the CP communities than for the SBO communities. At time 2, the net change in the prevalence of smoking was 4.5%, meaning that smoking prevalence decreased more in CP communities than in SBO communities. At time 4 the effect was 2.4%. At time 5, communities receiving the community programme had a net reduction in smoking prevalence of 3.8%. Inspection of fig 2, and statistical tests comparing time 1 with subsequent time points, indicated that the prevalence of smoking in SBO communities increased significantly from time 1 to each of the subsequent time points:
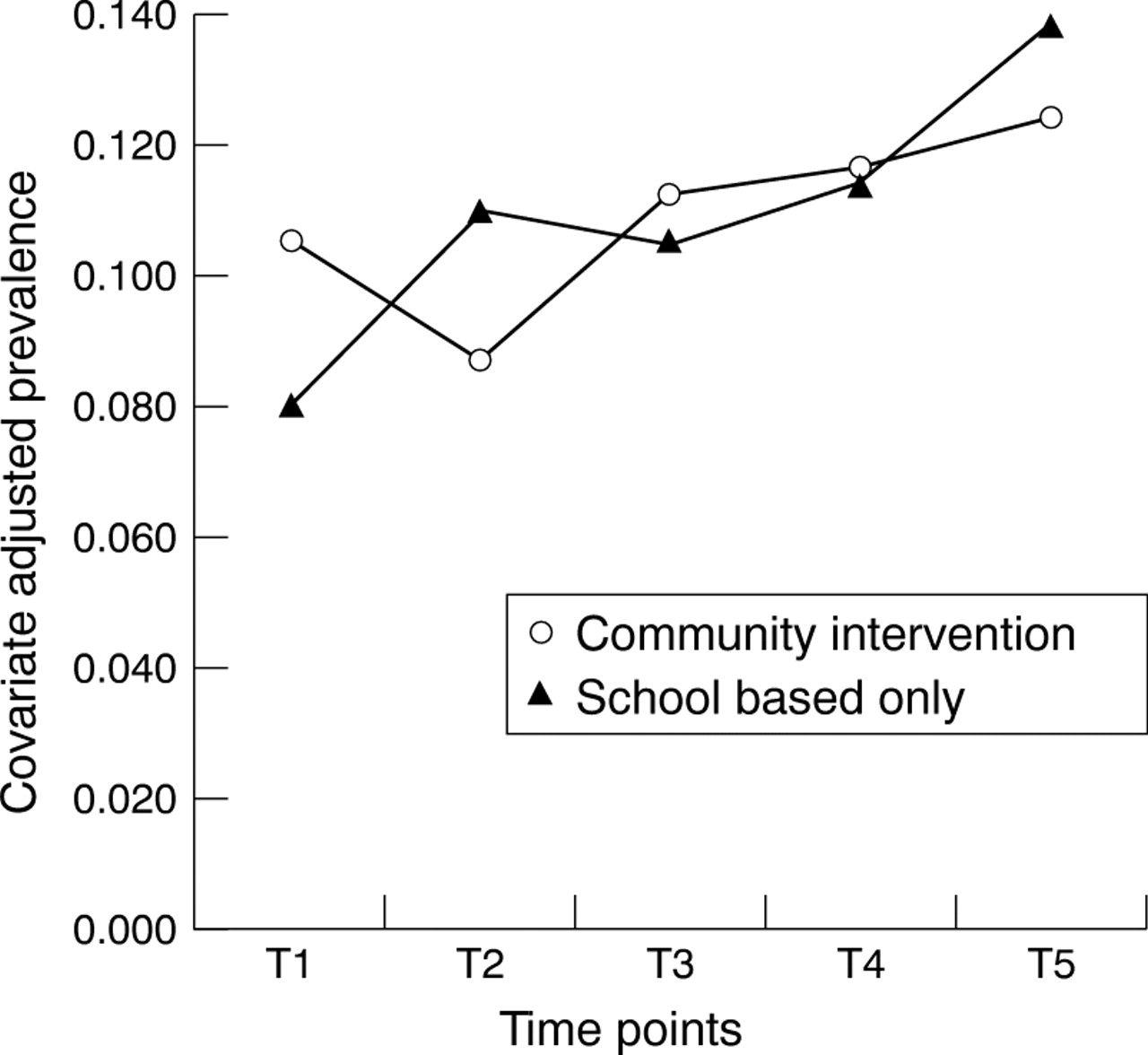
Prevalence of cigarette smoking for grade 7 and grade 9 students across all five time points.
Effects of the community intervention on the prevalence of smoking
t(14) = 2.50, p = 0.026 at time 2; t(14) = 2.64, p = 0.020 at time 3; t(14) = 3.91, p = 0.002 at time 4; t(14) = 5.27, p < 0.001 at time 5.
There was no significant change in smoking prevalence in the CP condition. Thus, the effect of the intervention was to prevent an increase in prevalence.
The random coefficients analysis did not indicate a significant difference between conditions at time 1. However, since we did additional analyses at individual time points and because the means of the two conditions differed at time 1, we also did a simple comparison of time 1 means. That result was not significant (F = 3.60, df = 14, p = 0.08, though the F value approached significance).
Given that the time 2 prevalence rates for both conditions appeared to deviate from the overall trend of the data, and that the effect at time 2 may partly depend on the larger than average increase in prevalence for SBO communities, we tested whether the slope for prevalence of smoking differed between conditions when time 2 data were not included. We found that the slopes for conditions did differ significantly (t(14) = −2.79, p = 0.014, lower bound = −0.016, upper bound = −0.002). Thus, even if the conditions differed at time 1, the difference in slope suggests that the community intervention did influence trends in the prevalence of smoking. Moreover, the time 2 data provided the strongest evidence of an intervention effect. Their deletion from this analysis could not bias the analysis in favour of finding a stronger intervention effect than if these data points had been included. Rather, the result suggests that our failure to find a difference in slope in the initial analysis was caused by the deviation at time 2 from a straight line and that the intervention effect exists even after excluding the data points that provide the strongest evidence.
Boys' smokeless tobacco use in the prior month
The random coefficients analysis of the effect of condition on boys' smokeless tobacco prevalence was not significant. There was a significant interaction, however, between grade and condition on smokeless tobacco prevalence at time 2 (t(14) = −2.27, p = 0.040). There was a significant intervention effect in grade 9 (t(14) = −2.50, p = 0.026), but not in grade 7. Prevalence decreased significantly in CP communities from 13.8% to 9.7% (t(14) = −2.26, p = 0.040), but did not change significantly in the SBO condition (11.4% at time 1 and 13.6% at time 2). Thus, the net effect on prevalence was 6.3%.
Carbon monoxide
There was no evidence that the CP and SBO communities differed on expired air carbon monoxide at any time points.
EFFECTS ON OTHER BEHAVIOUR
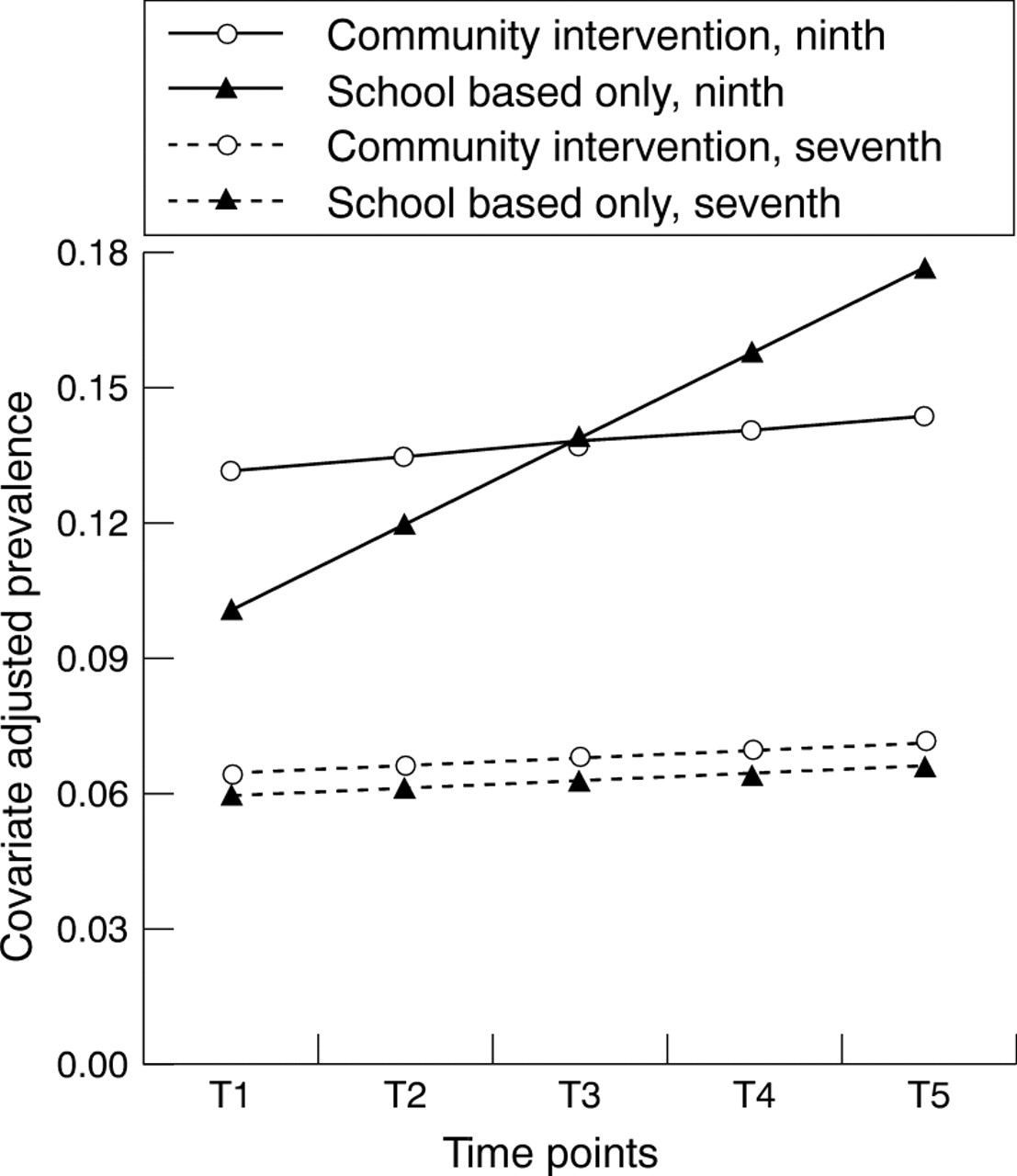
Figure 3 shows the prevalence of weekly alcohol use over five years in each condition. The random coefficients analysis for the prevalence of alcohol use indicated that there was an interaction between grade and condition (t(14) = 2.68, p = 0.018). For grade 9 students there was a significantly greater increase in the prevalence of weekly alcohol use in the SBO communities than in the CP communities (t(14) = 3.77, p = 0.002), with a significantly increasing slope for the SBO communities (t(14) = 6.79, p < 0.001) and a slope in the CP condition that was not different from zero.

{kind=link}
{kind=link}
{kind=link}
Alcohol use across all five time points for each grade and condition.
The random coefficients analysis revealed a quadratic effect for the prevalence of marijuana use in the prior week (t(14) = 2.22, p = 0.043). In essence the curve for marijuana prevalence for the SBO condition was concave up and the curve for the CP condition was concave down. Marijuana prevalence started lower in CP communities than SBO communities (1.3% v 2.5%). Prevalence rates were virtually identical by time 3 (4.6%) and had diverged by time 5 such that prevalence was 6.7% for CP communities and 8.5% for SBO communities. The overall increase in marijuana prevalence that these figures show is consistent with the trend toward greater marijuana use that occurred during this period.23
There was no evidence that the intervention affected adolescents' reports of antisocial behaviour.
EFFECTS ON MEDIATORS OF TOBACCO AND OTHER SUBSTANCE USE
We tested whether the community programme affected processes that would plausibly mediate the relation between the intervention and its effects on tobacco and other substance use.
Effects on young people.
Table 4 presents the six youth self report variables on which CP and SBO communities differed significantly. Eight variables were analysed.
Adolescent mediating variables affected by the community program
There were no effects on adolescents' awareness of cessation and prevention activities. Data on awareness of efforts to prevent illegal sales were not obtained at time 1. Still, there was a significantly more positive slope in CP than in SBO communities for this variable for the remaining time points. Indeed the slope was positive for the CP communities (t(14) = 2.04, p = 0.061), but significantly negative for SBO communities (t(14) = −3.19, p = 0.007).
Over the five years of assessments the slope for attitudes toward tobacco use was significantly more negative for CP communities than for SBO communities. Attitudes toward tobacco became more negative over time for CP communities (t(14) = −5.00, p < 0.001), but not significantly so for SBO communities (t(14) = −1.92, p = 0.075).
Adolescents' ratings of their intentions to smoke had a significantly more positive slope in SBO communities than in CP communities, but the effect held only for grade 9 students.
Changes from time 1 to time 2 in males' intentions to chew differed significantly between conditions. Intentions increased significantly in SBO communities (t(14) = 2.63, p = 0.020), but decreased significantly in CP communities (t(14) = −2.32, p = 0.036).
Change in adolescents' reports of their friends' smoking differed significantly between the two conditions at both time 2 and time 5. In SBO communities, the number of friends smoking increased significantly from time 1 to time 2 (t(14) = 5.05, p = 0.001) and from time 1 to time 5 (t(14) = 4.97, p = 0.001). However, it did not change in the CP communities.
At time 2, the conditions differed on changes in adolescents' reports of the general deviance of their peers. In SBO communities, there was a significant increase in peer deviance (t(14) = 2.77, p = 0.015), but peer deviance stayed the same in CP communities.
Effects on parents.
Table 5 presents parent report variables that might have been affected by the community programme. In CP communities, parents reported seeing more community efforts to prevent youth access to tobacco at times 2, 3, and 4, although the effect only approached significance at time 2, where we had data from only eight communities. Parents in CP communities also reported significantly more community support for access restrictions at times 2, 3, and 4.
Parent mediating variables
The intervention also brought about changes in parents' perception of community support for tobacco prevention in general. There were significant linear and quadratic effects. There was a significantly greater linear increase in perceived support in CP communities than in SBO communities, but perceptions of support in CP communities levelled off at time 4.
Parents' ratings of support for prevention by schools and government officials were not influenced by the intervention. However, for perceived support by business leaders there was a significant linear effect when the marginally significant (p = 0.080) quadratic effect was included in the model. Inspection of the means indicated that business support was seen as increasing over time in CP communities, but not in SBO communities. The difference diminished at time 5.
The general lack of effects at time 5 on these variables may have been caused by the unavailability at this time of data from eight of the communities.
Given that the intervention concentrated on preventing tobacco use, yet appears to have affected alcohol and marijuana use, we checked to see if parents' perceptions of community support for alcohol and drug abuse prevention were affected by the intervention. There were no significant effects on this variable.
There was no evidence that the community intervention increased parents' reports of their talking to their spouse about teen tobacco use or their joining a parent network against tobacco use.
Discussion
The results suggest that a community intervention that targets multiple influences on adolescent tobacco use can improve on the effects of a school based programme alone. Smoking prevalence was significantly lower in community intervention communities than in school based only communities after one year of intervention and one year after the intervention had been ended. The effect on smoking prevalence after three years of intervention also approached significance, using a two tailed test (p = 0.077). The overall slope of the prevalence of smoking across the five years of assessment did not differ between conditions, although the slopes did differ significantly when the time 2 data points were deleted from the analysis. The prevalence of boys' smokeless tobacco use was also affected after one year of intervention, with a net effect on prevalence of 6.3%. Thus, the Project SixTeen campaign, which included media advocacy, youth anti-tobacco activities, family communications about tobacco use, and access reduction, appears to be of value for preventing adolescent tobacco use.
The random coefficients analysis which deleted time 2 data points deserves further comment. For both conditions, the means at time 2 deviated from the general linear trend for that condition, but these data points provided the strongest evidence of an intervention effect. Thus, deleting these data points would not bias the analysis towards finding a significant effect in favour of the community intervention. The fact that the condition slopes differed when these data points were deleted suggests that our initial slope analysis involving all five data points was non-significant because the time 2 results deviated from the generally linear trend and not because the community intervention had no effect on the trend in smoking prevalence.
The findings are consistent with other studies of community interventions to prevent adolescent tobacco use.3-6 Two studies have shown that a school based prevention programme, when delivered in the context of a community wide cardiovascular risk reduction programme targeting adults, can have a significant effect on youth smoking prevalence use.3 5 However, neither of those studies included intervention elements directly targeting adolescent smoking through channels other than the classroom. Thus, they do not indicate whether a community intervention targeting adolescent tobacco use adds to the effects of a classroom programme. Pentz, Johnson, and colleagues3 4 did target adolescent tobacco use with a comprehensive intervention that included media, the organising of community leaders, and a component targeting parents. However, in the Pentz and Johnson study, the comprehensive intervention was compared with media and community organising alone, thus not making it possible to determine how well community components add to a school based programme alone.
The present study provides a clear comparison of school based and comprehensive community programmes for preventing adolescent tobacco use, and its results provide some support for the efficacy of a community programme. Moreover, the study provides the first randomised experimental evaluation of a community prevention programme in which whole communities were randomly assigned to conditions.
The results also suggest that preventing tobacco use may contribute to discouraging other substance use. Among ninth graders the conditions differed significantly on the slope of alcohol use; there was increasing alcohol use in SBO communities over the four years of the study, but alcohol use in CP communities did not increase. For marijuana use the intervention had the effect of damping down the increase in marijuana use that was seen in SBO communities and the society at large.23 There is reason to view tobacco use as one facet of a more global syndrome of adolescent problem behaviours.24-26 Moreover, there is evidence indicating that smoking is frequently the first of these behaviours to emerge.27 These correlational studies suggest that the prevention of tobacco use could prevent the development of other problems; however, experimental evidence has been lacking. The present results lend experimental support to the notion that preventing tobacco use could prevent other substance use.
These results are by no means as strong as we would have liked. Although the prevalence of smoking was affected in three of the four years, the slopes of the two conditions differed only when data from time 2 were not included. Moreover, the only effect on smokeless tobacco use was found after the first year of intervention among grade 9 boys. Finally, inspection of fig 2 shows that the general trend in the prevalence of smoking was increasing over the four years of assessments, a trend that has been noted in other assessments of adolescent smoking during this period.28 Thus, apparently the best that community intervention was able to do was to damp down an increase in smoking.
Finally, the communities involved in Project SixTeen are largely representative of rural areas in a single northwestern state and only two had significant numbers of minorities. Thus, the findings need to be replicated in larger and more ethnically diverse communities.
Acknowledgments
This research was supported by grant CA 38273 from the National Cancer Institute. Preparation of this manuscript was supported in part by grant DA 07389 from the National Institute on Drug Abuse. The authors would like to thank David Murray for advice on analysis and Ed Lichtenstein and Russ Glasgow for comments on the manuscript. We would also like to thank the following community coordinators for their contributions to this project: Jamie Henderson, Delaine Humphreys, Debra Levings, Virginia Koehn, Sandra Smith, Rebecca Whisman, Zada Wright, and Maija Yasui.