Article Text

Abstract
Aim: To conduct a pilot randomised controlled trial of mobile phone-based smoking cessation support intervention for the UK population.
Design: Randomised controlled trial (txt2stop).
Setting: Community.
Participants: 200 participants responding to radio, poster and leaflet-based promotions regarding the trial.
Main outcome measures: The response rate for the outcome measures planned for the main trial. Participants’ qualitative responses to open-ended questions about the intervention content. Secondary outcomes were the outcomes planned for the main trial including the point prevalence of self-reported smoking at 4 weeks and pooled effect estimate for the short-term results for the STOMP and txt2stop trials.
Results: The response rate at 4 weeks was 96% and at 6 months was 92%. The results at 4 weeks show a doubling of self-reported quitting relative risk (RR) 2.08 (95% CI 1.11 to 3.89), 26% vs 12%. The pooled effect estimate combining txt2stop and a previous New Zealand trial in the short term is RR 2.18 (95% CI 1.79 to 2.65).
Conclusions: Mobile phone-based smoking cessation is an innovative means of delivering smoking cessation support, which doubles the self-reported quit rate in the short term. It could represent an important, but as yet largely unused, medium to deliver age-appropriate public health measures. The long-term effect of this mobile phone-based smoking cessation support will be established by a large randomised controlled trial currently in recruitment.
Statistics from Altmetric.com
Most people killed by tobacco started smoking as teenagers and smoking contributes to the death of one in two of those who continue to smoke past 35 years of age.1 2
Mobile phones provide a new channel for individualised programmes to be delivered inexpensively wherever the person is located. For many people mobile phones are always carried with them, therefore the intervention can take place at any time. The text message programme can also be personalised. Furthermore, mobile phone-based interventions can provide the anonymity that many people like.3 4
The STOMP (STOp smoking with Mobile Phones) trial of a text message-based smoking cessation intervention showed a twofold increase in self-reported quit rates at 6 weeks (239 (28%) vs 109 (13%), relative risk (RR) 2.2, 95% CI 1.79 to 2.70).5 Some limitations in the study, however, affected the validity of the results at 6 months. First, there was differential loss to follow-up at 6 months. Second, only a small sample of self-reporting quitters were selected for biochemical validation through salivary cotinine testing.
We conducted a pilot study for a randomised controlled trial that will assess reliably whether mobile phone-based support can improve smoking cessation rates at 6 months in the United Kingdom. We set out to adapt the STOMP intervention for a UK population, test the study methods and evaluate the effect of the intervention on the point prevalence of smoking at 4 weeks.
METHODS
Modifying the intervention for the United Kingdom
The STOMP intervention contains over 1000 text messages,5 examples of which are shown in table 1. To modify the intervention, youth smoking cessation counsellors, cognitive behavioural therapists, motivational interviewing-trained smoking cessation counsellors and potential participants reviewed all text messages in a series of focus groups. Each text message was reviewed in at least two focus groups of participants. The STOMP intervention included a month of free texting. It was not possible to provide this aspect of STOMP in the United Kingdom where numerous mobile phone companies are in operation.
The pilot randomised controlled trial
Txt2stop is a single-blind randomised controlled trial. The intervention is delivered by computer and the allocation is unknown to all investigators collecting or analysing outcome data.
The interventions
Control group
Participants in the control group received fortnightly, simple, short, generic text messages.
Intervention group
The txt2stop intervention is a composite intervention that includes key elements of existing effective interventions as identified in systematic reviews.6–9 These elements include making a public declaration; setting a quit date; self-monitoring; intra-treatment support from a quit buddy; extra-treatment support by encouraging testing family and friends for support, problem solving; distraction techniques. Participants are asked to identify their interests and issues related to quitting, such as fitness or weight gain, so that individually tailored text messages can be sent. A text “Crave” function allows participants to request an immediate message of support whenever they experience cravings for a cigarette. Daily text messages commence at randomisation with a countdown to quit day and then five messages per day for 4 weeks after the quit day. The intervention continues with a maintenance package of three text messages per week for 26 weeks.
Procedures
We advertised the txt2stop pilot trial using the radio, leaflets and posters. Participants registered their interest via text message. Research assistants contacted those who registered an interest. Eligible participants were aged 16 years or more, currently smoking cigarettes daily and interested in quitting, a current owner of a mobile phone, living within an hour of London, familiar with text messaging capabilities and able to provide informed consent to participate in the study. There were no restrictions on the use of other smoking cessation treatments or methods. Eligible participants were sent the participant and consent information. Participants sent their consent via a text message. The research assistant directly entered baseline data into the web-based trial entry form linked to the database. An electronic link to the computer-based randomisation resulted in the generation of a unique identifying number and allocation to the intervention or control group. The system then automatically generated intervention or control group texts according to the allocation. To ensure a reasonable balance on key factors that may influence the success of the smoking cessation intervention, the allocation used a minimisation algorithm, balancing for sex (male/female), age (16–18 years, 19–34 years, >34 years), educational level (to age 16 years or less, >age 16 years), socioeconomic status (employment manual, non-manual, not applicable) and the Fagerstrom test for nicotine dependence (FTND, 5 or less, >5) (see fig 1).

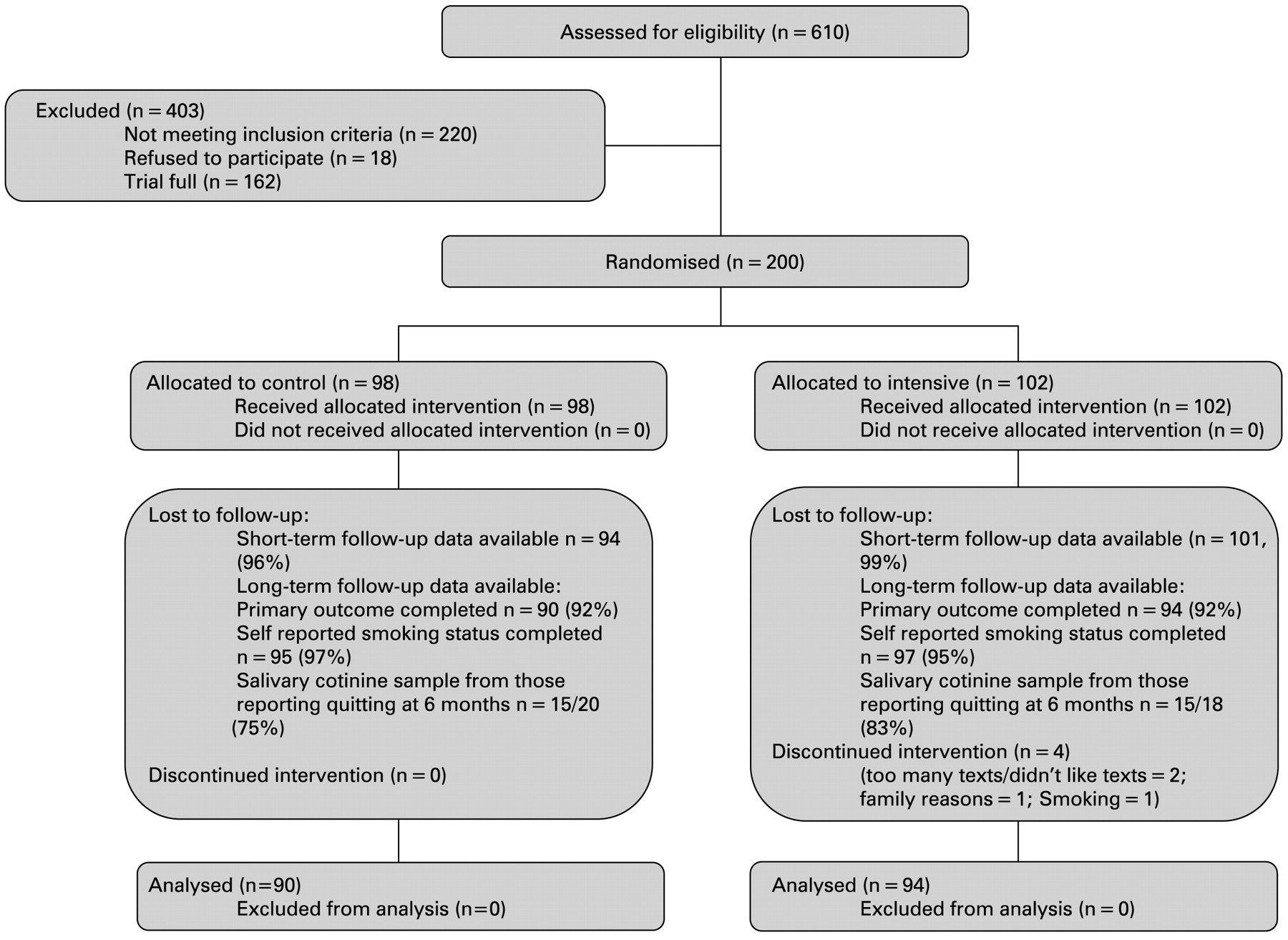{kind=link}
Flow chart.
Follow-up was at 4 weeks and 6 months. All self-reported outcome data were collected by mobile phone or email. Salivary cotinine testing was used to verify any self-reported smoking cessation at 6 months.10 Test kits containing a stamped addressed envelope were mailed to participants. Participants were also contacted to arrange collection of a salivary cotinine sample in person. Samples were stored in a freezer and delivered in batches to the laboratory where they were analysed.
Outcomes
Outcomes for the pilot study were the point prevalence of smoking at 4 weeks, the response rate for the primary outcome measure for the main trial; baseline smoking cessation rate in the control group; the proportion of participants whose assessed smoking status differed between salivary cotinine samples collected by post and in person; and participants’ qualitative responses to open-ended questions about the intervention content.
We collected outcome data pertaining to the primary and secondary outcomes planned for the main trial. The primary outcome for the main trial is self-reported abstinence (point prevalence—that is, no smoking in the past 7 days) at 6 months post-randomisation, with reports of abstinence verified by salivary cotinine testing using a cut-off of 7 ng/ml of cotinine.11 12 Secondary outcomes at 6 months are 28-day continuous abstinence, self-reported continuous abstinence since a quit day, involvement in any vehicle crashes and pain in the thumb.
Sample size
The pilot phase aimed to recruit 200 participants, and was not powered for outcomes at 6 months.
Statistical analysis
All analyses were based on the intention-to-treat principle and were conducted in Stata version 9.0. We estimated the relative risk and 95% confidence intervals of smoking cessation at 4 weeks and 6 months. We report the findings treating losses to follow-up as smokers and excluding losses to follow-up. As the txt2stop programme is based on the New Zealand STOMP programme we used random effects meta-analysis to give pooled estimates for the short-term results of the txt2stop and STOMP trials.13
RESULTS
Modifying the intervention for the pilot trial
Based on feedback from 62 participants we made four types of modification to txt2stop: we changed specific words—for example, different terms used in the United Kingdom; we changed culturally specific references—for example, sports personalities; we changed the framing of text messages—for example, to involve more “suggestion” and “less telling”; and we altered or removed some texts—for example, texts which participants found “too American”, “irritating” or “patronising”.
The pilot randomised controlled trial
We recruited the target of 200 participants within 18 days from the trial launch and closed the trial to further recruitment. The average age of participants was 36 (SD 9) and 126 participants (62%) were men. Sixty-six (33%) were in manual occupations. Participants smoked a median of 20 cigarettes per day (interquartile range (IQR) 12–22).
Using evidence-based methods14 we achieved 98% short-term follow-up, and 92% long-term follow-up in both intervention and control groups. Two participants withdrew from the study as they did not like the text messages or thought the text messages occurred too frequently. There were no instances where the postal salivary cotinine sample showed the participant had quit smoking and the sample collected in person showed the participant was smoking.
The txt2stop messages were described as “very good”, and “very motivating”. Some reported that specific aspects of the programme were helpful: “I found myself talking myself out of having another cigarette when my buddy was the one craving one”. or “Every time I was craving a cigarette I’d get a text and it would stop me. They’d always arrive at the right time”. Quit buddies were described as “great” by some but others were disappointed with their quit mate. Some participants wanted to be able to re set a quit date or set their own start time for the messages. A number of participants found the text abbreviations hard to understand and wanted messages in standard English. Some found the programme “too intense” and “intrusive” while others wanted the intensive phase to continue longer.
The short-term results at 4 weeks, assuming losses to follow-up as smokers, showed a doubling of self-reported quitting from 12% (12/98) in the control group to 26% (26/102) in the intervention group (RR 2.08 (95% CI 1.11 to 3.89). The pooled effect estimates for short-term abstinence in the txt2stop and STOMP trials was RR 2.18 (95% CI 1.79 to 2.65). There were no other statistically significant outcomes (table 2).
DISCUSSION
The txt2stop intervention effect and the pooled effect estimate for the txt2stop and STOMP trials show a doubling in self-reported quitting in the short term.
Using evidence-based methods we addressed the limitations of the earlier STOMP trial. Participants’ comments enabled us to modify the intervention for the United Kingdom and helped illustrate how specific components of the intervention may help participants to quit.
Mobile phones are a promising and innovative new means of delivering smoking cessation support. They could represent an important, but as yet largely unused, medium to deliver age appropriate public health measures. The long-term effects of such interventions need to be established.
What is already known
A New Zealand trial demonstrated that mobile phone-based smoking cessation support can be effective in the short term.
Long-term effects and the consistency in different populations remains uncertain.
What this paper adds
Tailoring and updating content to suit the UK public is feasible, and the programme is technically transferable.
The txt2stop pilot shows that the text message programme doubles the quit rate in the short term.
Evidence-based retention techniques can ensure long-term follow-up in this target group and a main trial powered to assess long-term cessation rates is feasible.
Footnotes
Competing interests: None.
Funding: Cancer Research UK.
Ethics approval: Ethics approval was obtained from the London School of Hygiene and Tropical Medicine ethics committee.