Article Text

Abstract
Objective To contribute new multinational findings on basic descriptive features of smoking and cessation, based upon standardised community surveys of adults residing in seven low-income and middle-income countries and 10 higher-income countries from all regions of the world.
Methods Data were collected using standardised interviews and community probability sample survey methods conducted as part of the WHO World Mental Health Surveys Initiative. Demographic and socioeconomic correlates of smoking are studied using cross-tabulation and logistic regression approaches. Within-country sample weights were applied with variance estimation appropriate for complex sample survey designs.
Results Estimated prevalence of smoking experience (history of ever smoking) and current smoking varied across the countries under study. In all but four countries, one out of every four adults currently smoked. In higher-income countries, estimated proportions of former smokers (those who had quit) were roughly double the corresponding estimates for most low-income and middle-income countries. Characteristics of smokers varied within individual countries, and in relation to the World Bank's low-medium-high gradient of economic development. In stark contrast to a sturdy male-female difference in the uptake of smoking seen in each country, there is no consistent sex-associated pattern in the odds of remaining a smoker (versus quitting).
Conclusion The World Mental Health Surveys estimates complement existing global tobacco monitoring efforts. The observed global diversity of associations with smoking and smoking cessation underscore reasons for implementation of the Framework Convention on Tobacco Control provisions and prompt local adaptation of prevention and control interventions.
- International
- epidemiology
- smoking prevalence
- cessation
- prevalence
- surveillance and monitoring
- tobacco products
Statistics from Altmetric.com
- International
- epidemiology
- smoking prevalence
- cessation
- prevalence
- surveillance and monitoring
- tobacco products
Introduction
In recent years, there have been major advances in our understanding of the descriptive epidemiology of tobacco smoking, other forms of tobacco consumption and tobacco attributed mortality and morbidity.1–7 An estimated quarter to a third of the world's population aged 15 years and older consumes tobacco on a daily basis.8 Surveillance and monitoring of smoking activity on a global level are important public health tasks in the context of effective tobacco control efforts.9
Surveillance and research accomplishments during the 1990s provided a glimpse of national differences of tobacco involvement. The WHO assembled information from surveys and administrative records so to permit publication of the 2003 edition of the WHO Tobacco Control Country Profiles. These profiles characterise the tobacco situation in 196 countries and territories around the world.3 Nevertheless, careful study of between-country variations in the tobacco smoking survey methods prompt cautious interpretation; many samples were non-representative; study designs and smoking assessments varied substantially. In another important cross-national study on the topic of nicotine prevalence and dependence, Fagerstrom and colleagues constrained some of the sources of variation and were able to present estimates based solely upon standardised nicotine dependence assessments. Nonetheless, even here there was some unevenness in methods of sampling and contexts for assessment (eg, in the clinical samples).10 11
Problems of this type can be overcome when research teams from different countries agree to follow a common protocol, as has been done in school surveys of tobacco and other drug involvement of young people in different regions of the world.2 4 12 13 Standardised surveys from probability samples of adults from numerous countries are also beginning to guide global tobacco control efforts.9 14–16 In addition, the first ever international cohort study of tobacco use, the International Tobacco Control Policy Evaluation Project, is now conducting parallel prospective surveys of representative samples of adult smokers in at least 20 countries (inhabited by over 50% of the world's population, 60% of the world's smokers), in an effort to evaluate the psychosocial and behavioural impact of the Framework Convention on Tobacco Control (FCTC).17 18
In the background of these investigations, there is a tobacco epidemic model synthesised by Lopez and colleagues, on the basis of previous surveillance data and several indicators of disease burden.19 The various epidemic stages described in this model highlight overall differences in the prevalence of smoking and attributable disease and deaths, as well as characteristic differences among users, such as ratios of male to female smokers. In many low-income and middle-income countries (generally characterised as Stage 1 and Stage 2 in the Lopez model), the estimated prevalence and consumption of tobacco cigarettes have been rising steadily.9 20 There is hope that vigorous prevention and early intervention efforts may help some of the low-income and middle-income countries avoid transitions to more advanced stages of increased consumption and disease burden that characterise later model stages. For example, many countries now are engaged in preventive actions to dissuade youths from smoking uptake. Nonetheless, each country will also need brief interventions and other aids to encourage quitting among smokers. Smokers who quit thereby limit the number of years of smoking and gain substantial benefits to health, wellbeing, and increased survivorship.21–23 In some high-income countries there have been recent increases in the percentage of former smokers, but generally little change in the percentage of former smokers has been found in low-income and middle-income countries where population-level monitoring has occurred.8
In consequence, along with surveillance of smoking uptake and associated health indicators, a population survey focus on former smokers, smoking cessation and characteristics associated with smoking cessation should be fruitful, providing additional clues about the course of the global tobacco epidemic. For this reason, our research group was granted permission to produce estimates of smoking prevalence, as well as to study former smokers, drawing upon some recently gathered data about mental health characteristics in 17 different countries from all regions of the world, representing a range of the higher-income, middle-income and low-income jurisdictions, during the first wave of the WHO World Mental Health Surveys Initiative (WMHS, http://www.hcp.med.harvard.edu/wmh). In this paper, we are able to characterise more than the ‘depth’ of the smoking epidemic in each country (as manifest in the country-specific prevalence estimates); we also gain a perspective on each country's progress in the promotion of smoking cessation in various population subgroups within each country—for example, as manifest in male-female differences in who has quit versus who has continued to smoked. For each regional site or country as a whole, and for males and females considered separately, the report provides estimates of smoking, based on cross-sectional survey data, with due attention to a two-group classification of smokers—that is, current smokers versus former or ex-smokers. Prevalence estimates are given for selected correlates of current smoking status (eg, age group) so as to help build up a more solid foundation of empirical survey findings, upon which tobacco researchers might construct more detailed and probing studies of the processes and conditions that foster smoking uptake and cessation in each place.
Methods
Populations and sampling approach
The WMHS Initiative continues to unfold, with new countries participating in successive waves, as resources become available and survey research teams learn and implement the standardised field survey protocol. This report is based upon WMHS data from the first 17 participating countries, with sites spread throughout all the major regions of the world. The consortium has a mental health focus, and its main goal is to estimate prevalence and impact of selected psychiatric disorders such as major depression and the anxiety disorders, worldwide, via standardised interviews and a common survey protocol.24–26 The countries, grouped by major region, encompass a range of economies as classified by the World Bank27:the Americas (Colombia, Mexico and the USA), Asia/Pacific (People's Republic of China (PRC), Japan and New Zealand), Europe (Belgium, France, Germany, Italy, The Netherlands, Spain and the Ukraine), and the Middle East and Africa (Israel, Lebanon, Nigeria, South Africa). While in many of the countries it was feasible to assess a nationally representative sample, estimates for several countries are based on area samples (table 1). The sample for Nigeria approximated 57% of the population, samples from Colombia and Mexico approximated 73% of their populations and samples for Japan and the PRC were selected from large metropolitan areas.
Characteristics of the first 17 population surveys for the World Mental Health (WMH) Survey Consortium
In each jurisdiction, nationally (or regional) representative household samples of adult residents were obtained via a multistage probability sample survey approach. To date, a total of over 80 000 adults have completed WMHS assessments, with participation levels as shown in table 1. Estimates reported in this paper are for adults age 18 years and older at the time of assessment; younger teenagers were surveyed in New Zealand and South Africa, where the research teams have prepared separate reports on smoking and other health characteristics of 15–17 year olds as part of internal country reports on their site-specific projects. In most countries, persons not speaking the country's primary languages were not sampled.
Field procedures
Training and field procedures for sampling, recruitment and assessment were standardised across countries.24 26 In almost all countries, trained lay interviewers carried out face-to-face recruitment and consent procedures, followed by either paper and pencil or computerised assessments. Informed consent was obtained after each individual had received a description of the study goals and procedures, data uses and protections, and participant rights. The institutional review board of the organisation coordinating the survey in each country approved and monitored compliance in human subject protection and informed consent processes.
Measures
The interview was divided into two parts to reduce respondent burden. Data for this paper are from the smoking screening questions assessed in the first part, completed by all participants at every site. This first part included standardised items on personal characteristics such as age, sex, marital status, a set of health behaviour screening items and a core diagnostic assessment for selected psychiatric disturbances. Items on employment and education were optional elements of this ‘Part 1’ assessment, and were not assessed in every country.
The key response variable in this report, for all countries except Israel, is based upon a self-classification of respondents who answered this question “Are you a current smoker [active], ex-smoker [former], or have you never smoked?” The Israel survey did not have the same question. Instead smoking status was identified by a set of responses to these two questions:“Are you currently smoking at least once a day [active]?” and “Have you ever smoked in the past, at least once a day [former]?”. Some sites also added a more comprehensive tobacco module in the second part of the interview with specifications for how much, how often, age of onset, etc (eg, cigarettes, cigars, pipes and other types of tobacco products), but the uneven availability of these data constrains multi-country analyses of the type reported here; these details are being reported by the individual sites in their own papers.28
Covariates of interest, also measured during interviews, included marital status categories, specified as currently married or living together, never married, or no longer married (widowed, separated or divorced) and five categories of education. Employment status categories reflect each respondent's main activity at the time of the interview. When respondents were not working or were students, homemakers or retired, they were classified as ‘other’ (mainly unemployed people).
Data analysis
Site-specific estimates are presented for proportions of smokers in relation to the characteristics just described. Estimation procedures for each country took into account differential probabilities of selection within households and communities, as well as post-stratification balance to known population census distributions (eg, age, sex). All estimates shown are based upon within-country weights and post-stratification adjustment, without a shift to world standard population distributions. In subsequent steps, we used simple cross-tabulations to study variations in smoking status (never vs ever and former versus current). Covariate-adjusted OR estimates were estimated via the generalised linear model with a logistic link to convey the strength of associations that link being male or female with being an ever-smoker and with respect to the active/former smoking contrast. Appropriate for complex sample survey designs, the survey commands and the Taylor series linearisation approach in Stata versions 9–10 were used for variance estimation and to estimate p values.29
Results
Country-specific smoking estimates
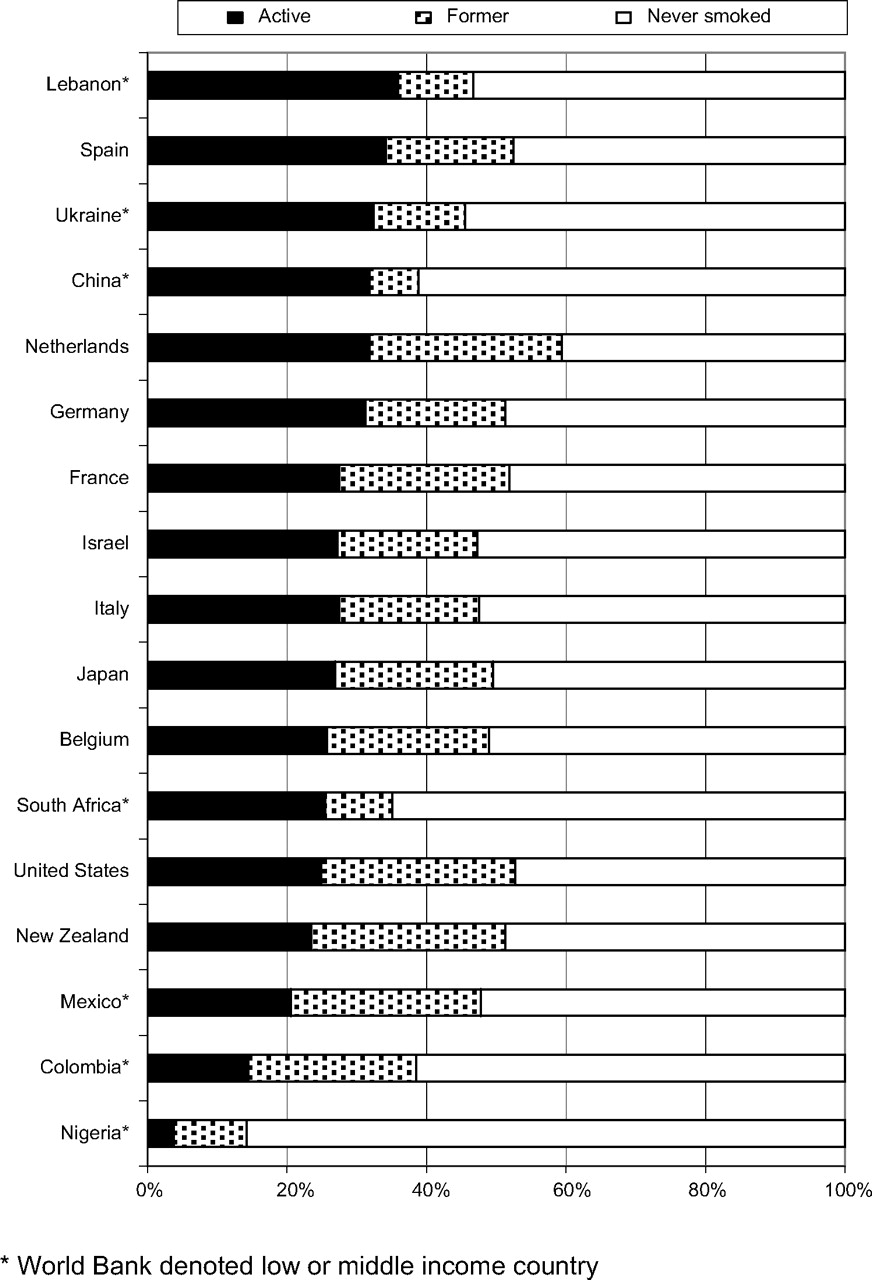
Estimated prevalence of smoking experience varied across the countries under study (figure 1). Typically, the estimated prevalence of ever-smoking (ie, active and former smokers combined) was lower in low-income and middle-income countries (14%–47%) compared to estimates for high-income countries (range 47%–60%). Throughout most of Europe, the USA, Israel and Japan, almost one-half of adults in the sampled community population initiated smoking; either they continue to smoke currently or they had smoked at sometime in the past. This estimated cumulative incidence proportion was largest in The Netherlands, where nearly three out of five adults had started smoking at some point during their lifetime. At the other extreme is Nigeria, with an estimate under 20%.
{kind=link}
Estimated overall prevalence of being an active or former smoker, by country, as well as the prevalence for never smoking. World Mental Health Survey Consortium Surveys.
We also see cross-national variation in the estimates derived from the WMHS cross-sectional survey data on current tobacco smoking (table 2). For example, Nigeria again provides an extreme value. In that country, the estimated fraction of current smokers among all adults is less than 1 in 20 (point prevalence=3.9). Columbia also shows a relatively low estimate at 14.6%. The estimated prevalence of current smoking is between 20% and 30% in nine of the countries studied, and in six countries the current smoking point prevalence estimates exceed 30%. Countries from each of the three income tiers are represented in the high prevalence stratum (Lebanon, Spain, Ukraine, PRC (Beijing and Shanghai sites), The Netherlands and Germany). As for being in the lowest rank with respect to estimated prevalence of current smoking among high-income countries, New Zealand, the USA and Belgium share this distinction.
Estimated overall prevalence (95% CI) of smoking status by country:WMH survey consortium, 2001–2005
Viewed cross-nationally, there is also considerable variation in estimates for former or ex-smoking (table 2). For example, in Nigeria, about three in every four smokers has quit; at the other extreme in the low-income and middle-income countries, for Lebanon, South Africa and China, the great majority of ever-smokers continue to smoke and did not qualify as former smokers. In European countries, roughly one-third to one-half of the smokers had quit. At the other extreme, in the Americas (Colombia, Mexico, USA), and in New Zealand, more than one-half had quit, describing themselves as former smokers.
Estimated proportion of smokers by selected background characteristics
Across countries, there is some substantial population subgroup variation in the estimated prevalence of current smoking, as can be seen in table 3 (low-income and middle-income countries) and table 4 (higher-income countries). Against a background of a generally sturdy male excess prevalence of smoking, relative to estimates for females, the male excess was rather modest or non-existent in New Zealand, Germany, The Netherlands and the USA, where roughly one-fifth to one-third of men and women qualified as current smokers. In contrast, nearly all adult current smokers in China and Nigeria were men; in South Africa, Ukraine and Japan, current smoking also was substantially more common among men.
Estimated prevalence of current smoking by selected sociodemographic characteristics in each of the low-income to middle-income countries (%, SE); World Mental Health (WMH) Survey Consortium
Estimated prevalence of current smoking by selected sociodemographic characteristics in each of the high-income countries (%, SE); World Mental Health (WMH) Survey Consortium
With respect to youngest adult age group (18–24 year olds), Germany and Ukraine had current smoking prevalence estimates above 45% (almost 1:1 odds of smoking), compared to other countries with corresponding values as small as one current smoker per 100 18–24 year olds in Nigeria (1.2%) and one per eight in Colombia (11.9%), and as large as one in 2.5 in Spain (42.1%). Current smoking prevalence among 18–24 year olds living in most of the high-income countries is often as high or higher than that for 25–44 year olds—something not seen among the low/middle-income countries. Current smoking prevalence estimates above 45% were observed only for 25–44 year olds in Spain and 35–54 year olds in Lebanon. Uniformly, current smoking prevalence estimates were lower for adults age 55 years and older, compared to their younger adult counterparts, most likely due in part to smoking-attributable excess mortality for smokers, although the contrast between 45–54 year olds and those 55 years and older was not especially marked in Mexico, Italy, Israel, The Netherlands and the USA.
The education gradients vary substantially across countries—in many countries, including the USA, prevalence is lower among those with no or some primary education than it is for those who finished primary schooling. In general, the highest current smoking prevalence estimates are observed for adults whose highest educational attainment was at the primary or secondary education levels. In many but not all of the countries, the proportion of smokers with minimal education was quite similar to the proportion of smokers found among those with the most education (ie, college graduates). In some countries smoking appears to be less common among college graduates while in other countries college graduates are more likely to smoke than those with no or some primary education only. The prevalence of current smoking for college graduates is comparable to that of adults with some college (but no college degree) in the Ukraine, Lebanon, Japan, Spain and Germany.
With respect to marital status, in many of the European countries, a larger proportion of never married adults were current smokers, compared to other categories. Nonetheless, estimated prevalence was not always the lowest among those married—for example, in Lebanon, a higher proportion of married than never married adults were current smokers.
In terms of employment, with two exceptions, Nigeria and Colombia, more than one-quarter of the working adults in other countries were current smokers. The prevalence range is wide, from 24% of workers in New Zealand to 45% of workers in Spain. Current smoking among adult students varied from as low as 1–5% in Nigeria and China to above 30% among students in Ukraine, France, Belgium and Germany, as well as in Israel (where the estimates pertain to current daily smoking as explained in the Methods section). For the most part, as expected, the proportion of current smokers among homemakers reflected that among females in general, and the proportion among those retired reflected the prevalence in the oldest age group. In all countries but one, the ‘other’ employment category (consisting largely of unemployed adults) was a subgroup with quite high prevalence of current smoking, the exception was Nigeria.
Male-female differences
Table 5 has a focus on male-female variation in the occurrence of smoking, both past and current. In all but one country (Nigeria), more than 50% of the men had a history of having smoked (up to approximately 80% in Ukraine and Japan). Lower values were observed for women such that there is a tangible association between being male and a history of smoking in all countries under study (including Nigeria; see first columns of table 5). A history of smoking tended to be more common among females in the high-income countries (in particular, nearly 50% in New Zealand, The Netherlands and the USA). In every country a male-female variation in the odds of ever smoking was noted (table 5). In Belgium, France, Italy, Spain, Mexico, Israel and Colombia, the odds of ever smoking among males were three times greater than the corresponding odds of smoking among females in these countries (adjusted OR ranged from 2.9–3.7). Especially large OR estimates were found in Japan, the Ukraine, South Africa, China and Nigeria, owing largely to generally smaller smoking proportions for the women in these countries.
Estimated sex-specific distribution (%) of smoking status, with covariate-adjusted OR estimates for the association between being male and smoking status. Data from each country participating in the World Mental Health (WMH) Survey Consortium
In stark contrast to the sturdily replicated male-female variations in the uptake of smoking seen across these countries, there is no similar sturdy cross-national pattern in the prevalence or odds of remaining a smoker (versus quitting) for males versus females (table 5). In the higher-income countries, roughly 30%–50% of ever-smokers of both sexes have stopped smoking; Spain is the exception among these countries (table 5; final columns). Among lower-income and middle-income countries, a relatively smaller proportion of ever-smokers had quit in China and Lebanon (<25%), and a relatively larger proportion had quit in Nigeria and Colombia (>60%). Once they had started smoking, females were just as likely as males to continue smoking (ie, be a current smoker) in Nigeria, China, South Africa, Colombia, Lebanon, Italy, New Zealand and Germany. The only country showing a statistically robust female excess in the odds of continuing to smoke among adult smokers was Spain, where 75% of the adult female ever smokers continued to smoke, versus 59% of the adult male ever smokers (aOR=0.7; p<0.001); a special opportunity for gender-targeted smoking outreach and intervention exists in that country.
In contrast with the pattern in Spain, a male excess in the odds of smoking persistence was found in six countries. In Ukraine and Japan, the evidence indicates that male smokers were more likely to continue smoking than their female smoking counterparts (aOR=2.5 and aOR=2.2, respectively, p<0.001). Adult male smokers in Israel, Mexico, France and Belgium are modestly more likely to remain active smokers, compared to female smokers (aOR=1.4, 1.6, 1.2 and 1.4 for Israel, Mexico, France and Belgium, respectively, p<0.05). It is noteworthy that in Israel, France and Belgium, somewhat more than one-half of ever-smokers were active smokers; this was not the case in Mexico where smokers were more likely to have quit than to have remained active smokers.
Discussion
This study, with multiple sites around the world using common standardised research protocols, provides estimates to describe (1) adult smoking experiences and (2) patterns of association for continuing to smoke among smokers in relation to being a male or female. A few design and measurement issues merit attention before a detailed discussion of the findings. The sampling approach (eg, nationally representative vs specific areas within the country), eligibility requirements (eg, age range differences) and the items assessing smoking status were not entirely uniform across countries. Furthermore, as mentioned in the introduction, this research consortium was focused on mental disorders and the study did not focus exclusively on ‘tobacco’ smoking or the features of smoking as they vary from place to place (eg, use of water pipe in Lebanon versus commercial or hand-rolled cigarettes elsewhere). Reporting biases may occur as the willingness to identify oneself as a current or past smoker might vary across national boundaries or across the population subgroups under study.30 In some countries, the mental health focus of the field research might have led some smokers to decide not to participate. Limitations such as these may affect these estimates to an unknown degree.
When these WMHS estimates are compared to previous global estimates, different methodological approaches and measures of these previous studies must also be taken into account—for example, whether these studies report estimates of daily tobacco smoking or daily cigarette smoking. Accordingly, this study's estimates for smoking (in general) should be higher than reported estimates of tobacco smoking or daily smoking per se. Even so, this study's range of estimates for prevalence of current smoking in several countries (25%–32%) is not appreciably different from the 1995 global estimate of 29% for daily smoking prevalence among those aged 15 and older.8 In addition, these WMHS estimates for a majority of the countries surveyed are not too distant from the individual country estimates reported in the most recent WHO report from 2008.9
Characteristics of smokers and correlates of smoking varied somewhat across the individual countries, and in relation to the World Bank's low-medium-high gradient of economic development, but a quite prominent male excess in the odds of ever-smoking was found, and one exceptional finding concerns failure to quit smoking among adult women in Spain, already mentioned in relation to possible gender-targeted outreach and intervention as part of a comprehensive tobacco prevention and control approach. The male excess odds of smoking in China is remarkable; in that country, male smoking started to increase several decades ago, while smoking among females is a more recent development and occurs substantially less frequently.31 China represents a enigma for the Lopez tobacco epidemic model as it might well otherwise qualify for one of the more advanced stages.19 Otherwise, this study's multiple country-specific smoking estimates for males and females generally are in line with the four-stage model of the tobacco epidemic proposed by Lopez and colleagues.19
In the higher-income countries, smoking prevalence across age groups did not vary greatly or when it did (eg, in New Zealand, Belgium and Germany) the proportion of young adults (aged 18–24) smoking was found to be larger than was observed for other age groups. Initiation still occurs frequently among individuals aged 18–24 and tobacco product marketing campaigns often target young adults.32–34 On the other hand, in several of the lower-income and middle-income countries, smoking was more common among the middle adulthood age group, substantiating a need for tobacco prevention and control beyond the young adult years. Indeed, Cho and colleagues recently found that among adults in South Korea there was an age-related decline for males and an age-related increase for women.35 This is a pattern not investigated in the present study, which remains on the agenda for future WMHS reports, as is an intriguing hypothesis that in some places there may be “influence of a culture which discourages married women from smoking, and “liberates” divorced women from [these] cultural sanctions” that otherwise would keep them from starting to smoke.35
Regarding employment, in all but two countries under study, more than 25% of the adult workforce were current smokers. These estimates draw attention to a potential opportunity for workplace smoke-free policies and smoking cessation programmes of the type developed elsewhere.36 Initiatives encouraging worksites and public places to be smoke-free may also increase the interest in creating smoke-free homes.36
The relation between smoking and education was not monotonic and varied substantially across the WMH countries. Education is often used as an indicator of socioeconomic status (SES) as it remains fairly stable during adulthood and is correlated with occupation, income and wealth. Studies in European countries indicate that different tobacco control efforts may influence the smoking rates among various educational/SES groups differently.37 38 Perhaps country patterns of the association between education/SES and smoking reflect a stage within the tobacco epidemic, as low SES groups may follow high SES groups, after a lag, in their rejection of smoking, just as they followed high SES groups, also after a lag, in the adoption of smoking.39
In general terms, within the lower-income and middle-income countries compared to the higher-income countries, a smaller proportion of the adult population has a history of smoking. Yet in Lebanon, China and the Ukraine, the estimated proportion of adults currently smoking was higher than proportions found in most higher-income countries, and in these three countries, the estimated proportion of ever-smokers who had quit was at the lower end of the observed ranges. Increased cigarette consumption is common among countries targeted by transnational tobacco companies,40–42 and where cigarettes have become more affordable as a result of raising household income and low excise taxes.43 Countries with a high economic interest at stake (history of being a substantial producer of tobacco crops) may favour short-term financial benefits over long-term health risks.
Previous studies have found individual and environmental characteristics associated with serious quit attempts and cessation,38 44–46 and find that increasing age helps predict quitting.44 47 48 Among a nationally representative sample of US adults, age, race, quantity of cigarettes smoked per day, income and health were independent predictors of quitting for at least 1 year; and younger age, female gender and urban residence were predictors of relapse.48 In four higher-income countries taking part in the International Tobacco Control Policy Evaluation Project, despite similarities in individual characteristics predicting making a quit attempt (intention, having tried to quit previously, duration of last quit attempt, less dependent on nicotine, more negative attitudes about smoking and younger age), differences in the success of quitting were found across countries suggesting environmental and sociocultural factors may contribute to varying trends in tobacco use.49 Consistent with these WMHS results, Jha and colleagues8 have noted a time trend that favours increased quitting among smokers in higher-income countries, but not in middle-income countries. Country differences in smoking and cessation rates may be attributable to tobacco control efforts at national levels as well as those targeting individual control. In Europe, reduced smoking rates have been found in countries with more developed and comprehensive tobacco control policies that included taxes, bans and restrictions, information campaigns, health warnings and access to treatment.38
Conclusion
It has been projected that within 25 years 10 million tobacco-related deaths will occur annually, with 70% of these deaths in lower-income and middle-income countries. It is estimated that roughly 25 million premature deaths in the first quarter of this century and about 150 million more by mid-century might be avoided if half of the active smokers were to quit.7 Our findings describe the characteristics of smokers in multiple countries around the world that might be used to guide tobacco control activities and smoking cessation campaigns. The results make it clear that there is a sturdy male excess in odds of starting to smoke, but otherwise a diversity of sociodemographic associations with smoking. Moreover, the male-female variations observed for starting to smoke are not present in the patterns observed for quitting once smoking starts. As we already have mentioned in the text, the observed variations may underscore the reasons for implementation of the FCTC provisions and prompt locally tailored outreach and intervention policies and programmes for tobacco prevention and control. Spain and the situation with females who smoke but haven't quit is a case in point, as is the situation with respect to workplace smoke-free policies and programmes to encourage smoking cessation in most countries studied here. A recent Cochrane review provides guidance in this respect.50
What this study adds
This study provides new multinational findings on the basic descriptive epidemiology of smoking and cessation from adults residing in seven low-income and middle-income countries and 10 higher-income countries from all regions of the world. The estimates are based on a general field survey research protocol as applied at each country or within-country site, with self-reported current and past smoking, as implemented for the WHO World Mental Health Initiative (WMH). Observed variations in current and former smoking status across the countries underscores the reason to implement FCTC provisions while also recognising a need for locally tailored interventions.
Acknowledgments
The surveys discussed in this article was carried out in conjunction with the WHO World Mental Health (WMH) Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork and data analysis. These activities were supported by the US National Institute of Mental Health (R01MH070884), the John D and Catherine T MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864 and R01 DA016558), the Fogarty International Center (FIRCA R01-TW006481), the Pan American Health Organisation, Eli Lilly and Company, Ortho-McNeil Pharmaceutical, Inc, GlaxoSmithKline and Bristol-Myers Squibb. A complete list of WMH publications can be found at http://www.hcp.med.harvard.edu/wmh/. The Chinese World Mental Health Survey Initiative is supported by the Pfizer Foundation. The Colombian National Study of Mental Health (NSMH) is supported by the Ministry of Social Protection. The ESEMeD project is funded by the European Commission (contracts QLG5-1999-01042; SANCO 2004123), the Piedmont Region (Italy), Fondo de Investigación Sanitaria, Instituto de Salud Carlos III, Spain (FIS 00/0028), Ministerio de Ciencia y Tecnología, Spain (SAF 2000-158-CE), Departament de Salut, Generalitat de Catalunya, Spain, Instituto de Salud Carlos III (CIBER CB06/02/0046, RETICS RD06/0011 REM-TAP) and other local agencies and by an unrestricted educational grant from GlaxoSmithKline. The Israel National Health Survey is funded by the Ministry of Health with support from the Israel National Institute for Health Policy and Health Services Research and the National Insurance Institute of Israel. The World Mental Health Japan (WMHJ) Survey is supported by the Grant for Research on Psychiatric and Neurological Diseases and Mental Health (H13-SHOGAI-023, H14-TOKUBETSU-026, H16-KOKORO-013) from the Japan Ministry of Health, Labour and Welfare. The Lebanese National Mental Health Survey (LEBANON) is supported by the Lebanese Ministry of Public Health, the WHO (Lebanon), anonymous private donations to IDRAAC, Lebanon, and unrestricted grants from Janssen Cilag, Eli Lilly, GlaxoSmithKline, Roche and Novartis. The Mexican National Comorbidity Survey (MNCS) is supported by the National Institute of Psychiatry Ramon de la Fuente (INPRFMDIES 4280) and by the National Council on Science and Technology (CONACyT-G30544- H), with supplemental support from the PanAmerican Health Organisation (PAHO). Te Rau Hinengaro:The New Zealand Mental Health Survey (NZMHS) is supported by the New Zealand Ministry of Health, Alcohol Advisory Council, and the Health Research Council. The Nigerian Survey of Mental Health and Wellbeing (NSMHW) is supported by WHO (Geneva), WHO (Nigeria), and the Federal Ministry of Health, Abuja, Nigeria. The South Africa Stress and Health Study (SASH) is supported by the US National Institute of Mental Health (R01-MH059575) and National Institute of Drug Abuse with supplemental funding from the South African Department of Health and the University of Michigan. The Ukraine Comorbid Mental Disorders during Periods of Social Disruption (CMDPSD) study is funded by the US National Institute of Mental Health (RO1-MH61905. The US National Comorbidity Survey Replication (NCS-R) is supported by the National Institute of Mental Health (NIMH; U01-MH60220) with supplemental support from the National Institute of Drug Abuse (NIDA), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Robert Wood Johnson Foundation (RWJF; Grant 044708) and the John W Alden Trust.
References
Footnotes
Funding The preparation of this manuscript was funded by the US National Institute on Drug Abuse (R01DA016558 and K05DA015799).The surveys discussed in this article was carried out in conjunction with the World Health Organization World Mental Health (WMH) Survey Initiative. We thank the WMH staff for assistance with instrumentation, fieldwork, and data analysis. These activities were supported by the United States National Institute of Mental Health (R01MH070884), the John D and Catherine T MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864, and R01 DA016558), the Fogarty International Center (FIRCA R01-TW006481), the Pan American Health Organization, Eli Lilly and Company, Ortho-McNeil Pharmaceutical, Inc, GlaxoSmithKline, and Bristol-Myers Squibb. A complete list of WMH publications can be found at http://www.hcp.med.harvard.edu/wmh/. The Chinese World Mental Health Survey Initiative is supported by the Pfizer Foundation. The Colombian National Study of Mental Health (NSMH) is supported by the Ministry of Social Protection. The ESEMeD project is funded by the European Commission (Contracts QLG5-1999-01042; SANCO 2004123), the Piedmont Region (Italy), Fondo de Investigación Sanitaria, Instituto de Salud Carlos III, Spain (FIS 00/0028), Ministerio de Ciencia y Tecnología, Spain (SAF 2000-158-CE), Departament de Salut, Generalitat de Catalunya, Spain, Instituto de Salud Carlos III (CIBER CB06/02/0046, RETICS RD06/0011 REM-TAP), and other local agencies and by an unrestricted educational grant from GlaxoSmithKline. The Israel National Health Survey is funded by the Ministry of Health with support from the Israel National Institute for Health Policy and Health Services Research and the National Insurance Institute of Israel. The World Mental Health Japan (WMHJ) Survey is supported by the Grant for Research on Psychiatric and Neurological Diseases and Mental Health (H13-SHOGAI-023, H14-TOKUBETSU-026, H16-KOKORO-013) from the Japan Ministry of Health, Labour and Welfare. The Lebanese National Mental Health Survey (LEBANON) is supported by the Lebanese Ministry of Public Health, the WHO (Lebanon), anonymous private donations to IDRAAC, Lebanon, and unrestricted grants from Janssen Cilag, Eli Lilly, GlaxoSmithKline, Roche, and Novartis. The Mexican National Comorbidity Survey (MNCS) is supported by The National Institute of Psychiatry Ramon de la Fuente (INPRFMDIES 4280) and by the National Council on Science and Technology (CONACyT-G30544- H), with supplemental support from the PanAmerican Health Organization (PAHO). Te Rau Hinengaro:The New Zealand Mental Health Survey (NZMHS) is supported by the New Zealand Ministry of Health, Alcohol Advisory Council, and the Health Research Council. The Nigerian Survey of Mental Health and Wellbeing (NSMHW) is supported by the WHO (Geneva), the WHO (Nigeria), and the Federal Ministry of Health, Abuja, Nigeria. The South Africa Stress and Health Study (SASH) is supported by the US National Institute of Mental Health (R01-MH059575) and National Institute of Drug Abuse with supplemental funding from the South African Department of Health and the University of Michigan. The Ukraine Comorbid Mental Disorders during Periods of Social Disruption (CMDPSD) study is funded by the US National Institute of Mental Health (RO1-MH61905). The US National Comorbidity Survey Replication (NCS-R) is supported by the National Institute of Mental Health (NIMH; U01-MH60220) with supplemental support from the National Institute of Drug Abuse (NIDA), the Substance Abuse and Mental Health Services Administration (SAMHSA), the Robert Wood Johnson Foundation (RWJF; Grant 044708), and the John W Alden Trust. Other funders:NIH.
Conflict of interests None.
Ethics approval The institutional review board of the organisation coordinating the survey in each country approved and monitored the compliance of human subject protection and obtaining informed consent. Data analysis activities were approved by the Johns Hopkins Bloomberg School of Public Health and Michigan State University institutional review boards.
Provenance and peer review Not commissioned; externally peer reviewed.