Article Text

Abstract
Objective: To assess the degree to which smokers living with a full household ban on smoking change their cessation related behaviour.
Design, setting, and participants: Prospective cohort study; follow up of a population based cohort of 1133 smokers, identified from a 1997 telephone survey of adult Oregonians. After a median of 21 months, 565 were located and reinterviewed.
Main outcome measures: Quit attempts, time until relapse, and smoking cessation, defined as seven day and 90 day sustained abstinence at follow up.
Results: A full ban at baseline was associated with a doubling of the odds of a subsequent quit attempt (odds ratio (OR) = 2.0, 95% confidence interval (CI), 1.0 to 3.9). Among respondents in the preparation stage at baseline (intention to quit in the next month with a quit attempt in the previous year), a full ban was associated with a lower relapse rate (hazard ratio = 0.5 (95% CI, 0.2 to 0.9)), while for those in precontemplation/contemplation (no intention to quit or intention to quit within the next six months, respectively), there was no significant association between full ban and relapse rate. For respondents in preparation, those with a full ban had over four times the odds of being in cessation for seven or more days before the follow up call (OR = 4.4 (1.1 to 18.7)), but for those in precontemplation/contemplation, full bans were unrelated to cessation.
Conclusions: Full household bans may facilitate cessation among smokers who are preparing to quit by increasing quit attempts. They may also prolong time to relapse among those smokers.
- smoking
- cessation related behaviour
Statistics from Altmetric.com
The practice of restricting smoking inside the home is becoming more common in the USA as non-smokers learn of the hazards of exposure to secondhand smoke.1 Smoking restrictions in worksites have led several investigators to explore whether these rules help smokers cut down or quit.2,3 Only a few studies, however, have explored whether smokers living in a household with smoking restrictions might quit smoking more often than those living without restrictions.
Two cross sectional reports from California have documented associations between bans and decreased amount smoked per day4 and greater interest in quitting.5 A national cross sectional study also showed an association between full household bans and quitting in the previous year.6 To date, however, we are unaware of any population based prospective data exploring whether smokers in a household with a ban actually change their smoking behaviour.
Our primary aim in this prospective study was to investigate the relation between household bans and smoking cessation. We were also interested in exploring whether household restrictions were associated with other cessation related behaviours such as the occurrence of a quit attempt and the length of quit attempts occurring during the follow up period. Previous work has shown that these behaviours are associated with a greater probability of eventual cessation7–11 and are likely to confer health benefits.12 If a low cost population based intervention such as a household smoking ban proves beneficial at all steps in the quitting continuum, not just in the ultimate step of cessation, it may be of significant use for clinicians, public health advocates, and individual non-smokers in discouraging smoking.
METHODS
Baseline survey
Between August and November 1997, a population based cross sectional telephone survey of 6199 adult English speaking Oregonians was carried out to provide information on smoking prevalence in the Oregon population and on knowledge and attitudes toward tobacco. Methods for the baseline study have been described previously.13
Follow up survey
In 1999, we conducted a follow up study of 1604 persons who were smokers or living in a household with at least one smoker, at the 1997 baseline survey. The median time to follow up was 21.3 months. A standardised questionnaire was administered by telephone and included questions on tobacco attitudes and practices. Average interview length was approximately 12 minutes. This analysis focused on 1133 respondents who were regular or occasional smokers at baseline. A smoker was defined as having smoked at least 100 cigarettes during their lifetime, and answering “every day” or “some days” to the question, “Do you now smoke cigarettes every day, some days or not at all?”.
Of the 1133 baseline smokers who were eligible for follow up (that is, who agreed to being recontacted and had information on home smoking bans), 583 completed interviews during two waves of call-backs—a response rate of 51.5%. The 48.5% loss to follow up was comprised of 10.2% refusals and 38.3% inability to locate the respondent. Of the 583 final cohort members, 18 were excluded from all analyses as they classified themselves as regular smokers at baseline and as never smokers at follow up.
Measures
We used data from the baseline survey to classify smokers according to their level of household smoking restriction using the following question: “Which of the following statements best describes the rules about smoking inside your home: (1) no one is allowed to smoke anywhere inside your home (full ban); (2) smoking is allowed in some places or at some times (partial ban); (3) smoking is permitted anywhere inside your home (no ban).”
We examined three outcomes: the occurrence of a quit attempt for at least one day before follow up; the time until relapse to smoking or follow up call; and cessation from smoking, defined as seven day and 90 day sustained abstinence at follow up.
Respondents who were abstinent at follow up (quitters) answered “not at all” to the follow up interview question, “Do you now smoke cigarettes every day, some days, or not at all?” To assess time since last cigarette, we used the question, “What was the date that you last smoked, even a single puff, on a cigarette?”. We assessed quitters using two definitions: those whose last puff was seven or more days before the follow up interview, or 90 or more days before follow up. Quitters whose time of last puff was less than seven days or less than 90 days were excluded from the relevant analysis rather than combined with the comparison group, as they may have eventually exceeded their observed periods of abstinence.
Quitting activity since the baseline interview among those still smoking at follow up was ascertained by asking the question, “Since we talked in the fall of 1997, about how many times have you quit smoking intentionally for 24 hours or longer?” Respondents who were abstinent at follow up were also credited with a quit attempt.
We examined the duration of quit attempts in order to determine whether household restrictions were related to relapse rates. We used the most recent attempt if there was more than one during the follow up period, and ascertained its length by asking, “For your most recent quit attempt, what is the total amount of time you did not smoke?” For quitters, we used time since last puff for duration of abstinence.
Information from the baseline survey was used to adjust for potential confounders (age, sex, race, educational level, employment status, presence of children under 18 in the household, baseline cigarette consumption, and stage of change). The stage of change model14,15 classifies smokers into the precontemplation, contemplation, or the preparation stage with respect to quit intention. Smokers in the precontemplation stage were not thinking of quitting smoking within the next six months at the baseline interview. Smokers in the contemplation stage were considering quitting in the next six months, and those in the preparation stage were considering quitting in the next 30 days and had a quit attempt of at least one day in the year before baseline. Smokers with an intention to quit in the next 30 days but who did had had a quit attempt in the previous year were classified as contemplators. In all analyses, we combined precontemplators with contemplators because of their similarities in addiction level and previous long term quit attempts.8 Furthermore, the preparation stage is differentiated by history of a quit attempt in the past year.
Analysis
We reweighted the follow up data, retaining factors affecting each respondent’s probability of selection at baseline and adding a weighting class adjustment to adjust for loss to follow up. The weighting class adjustment was computed by calculating the probability of response by those baseline demographic characteristics most highly related to response rate, and using the inverse of this probability to adjust for response at follow up.16,17 Finally, the data were post-stratified to the 1997 age and sex distribution by county. We used Stata 6.018 to carry out all analyses, a program which can account for complex survey designs and compute appropriately larger standard errors generated by such a design. We chose to use the odds ratio as a measure of association even though it is further from the null than the relative risk, as we were interested chiefly in the presence, direction, and relative strength of an association between smoking bans and smoking related outcomes. Adjusted Wald χ2 statistics were used to test for significance. All percentages presented in this paper are weighted, while counts are unweighted.
We also conducted Cox proportional hazards regression to examine whether household bans influenced the duration of quit attempts. The outcome for the analysis was defined as days until relapse to smoking occurred, and data for quitters were censored at the follow up interview. Although the analysis was done for the entire follow up period, we present Kaplan–Meier survival curves truncated at six months (180 days) to display better the earlier period of follow up where relapses were more frequent.
In all analyses, we chose to combine the no ban and partial ban categories because it is most relevant to study the effect of a full ban on smoking behaviour (full bans have been shown to be associated with fewer days of indoor smoking13, and will probably more often be recommended as a public health measure). Also, in preliminary analyses, the pattern of association between partial bans and the outcomes under study was more similar to that of no ban than full ban.
RESULTS
We examined differences in baseline characteristics among respondents and non-respondents. We found that non-respondents were significantly younger, more likely to be unmarried, to have lower annual household incomes, and to lack health insurance, but were similar to respondents with regard to sex, education and employment status, amount smoked, intention to quit smoking, and proportion having a full household smoking ban at baseline.
Cohort characteristics by exposure group (partial or no ban v full ban)
Table 1 presents the baseline characteristics of final cohort members with full ban v those with no ban or a partial ban. Smoking respondents with a full ban were younger (p < 0.05), more likely to be non-white, to have higher incomes (p < 0.05) and more education, to be married, and to have children at home than the group of smokers with partial bans or no bans at all. They were also more likely to be in contemplation or preparation, and to be occasional smokers (p < 0.05 for both).
Baseline cohort characteristics by household smoking restriction status*
Household bans and quit attempts
Of 565 baseline smokers, 371 (67%) had quit for at least one day before follow up. This group comprised respondents who had quit but relapsed during the follow up period (n = 256) and those who were in cessation at follow up (n = 115). Table 2 shows that those living with a full ban had twice the odds of a quit attempt lasting at least one day compared with those with no ban or a partial ban (odds ratio (OR) = 2.0 (95% confidence interval (CI) 1.0 to 3.9)). We also conducted an analysis restricted to those smokers who had quit but relapsed, and observed a similar association between household ban and quit attempts (data not shown).
Adjusted odds ratios for full household bans and one or more attempts to quit smoking between baseline and follow up*†
Household bans and duration of quit attempts
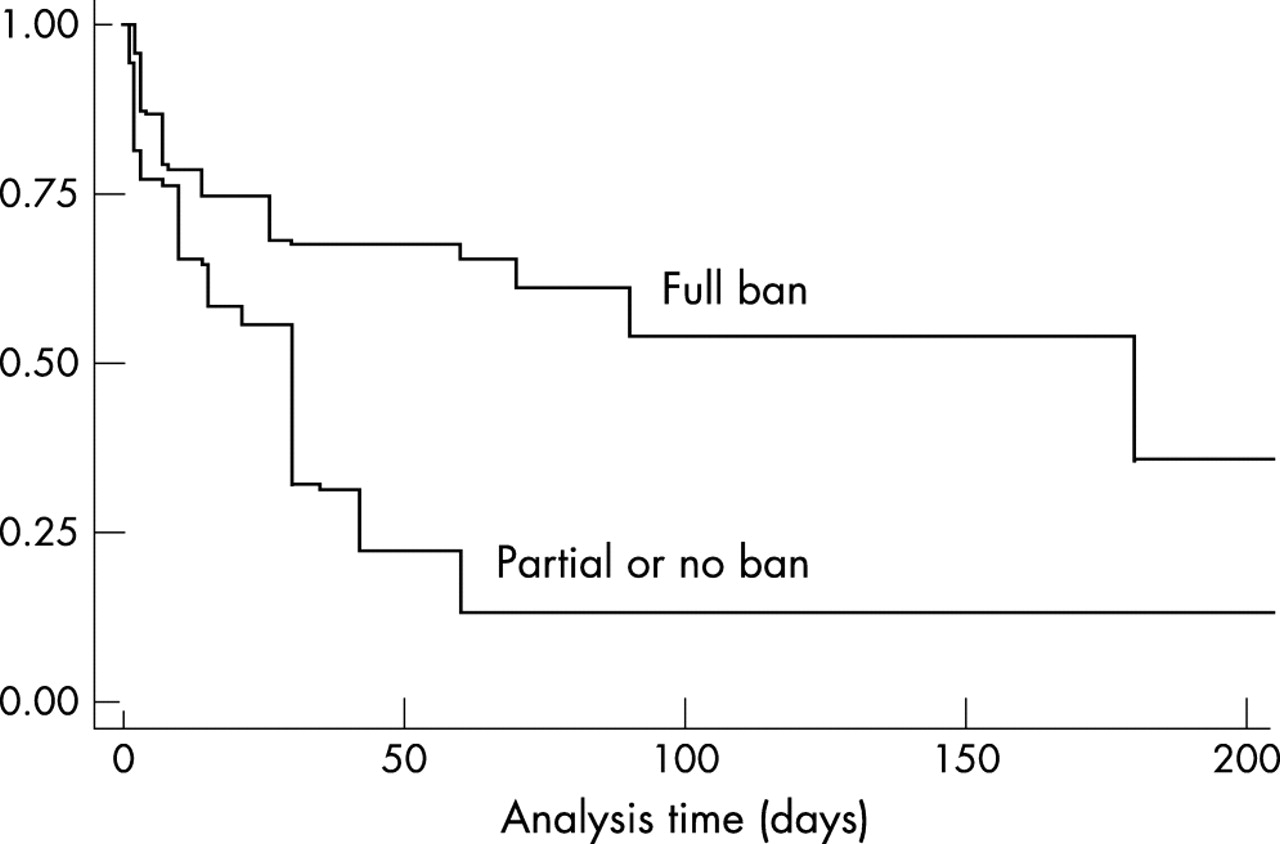
We examined whether a household ban might be associated with a longer time until relapse for these quit attempts. We found that stage of change at baseline modified the relapse rate (p = 0.02). For respondents in preparation (n = 82), a full ban on smoking was significantly associated with a lower relapse rate (hazard ratio (HR) = 0.5 (95% CI 0.2 to 0.9)) compared with those with no ban or a partial ban on smoking (fig 1). For those in precontemplation or contemplation (n = 281), having a full ban was not significantly associated with the relapse rate (HR = 0.3 (95% CI 0.8 to 2.0)) (fig 2). Addition of potential confounders to this Cox model did not appreciably change these estimates.
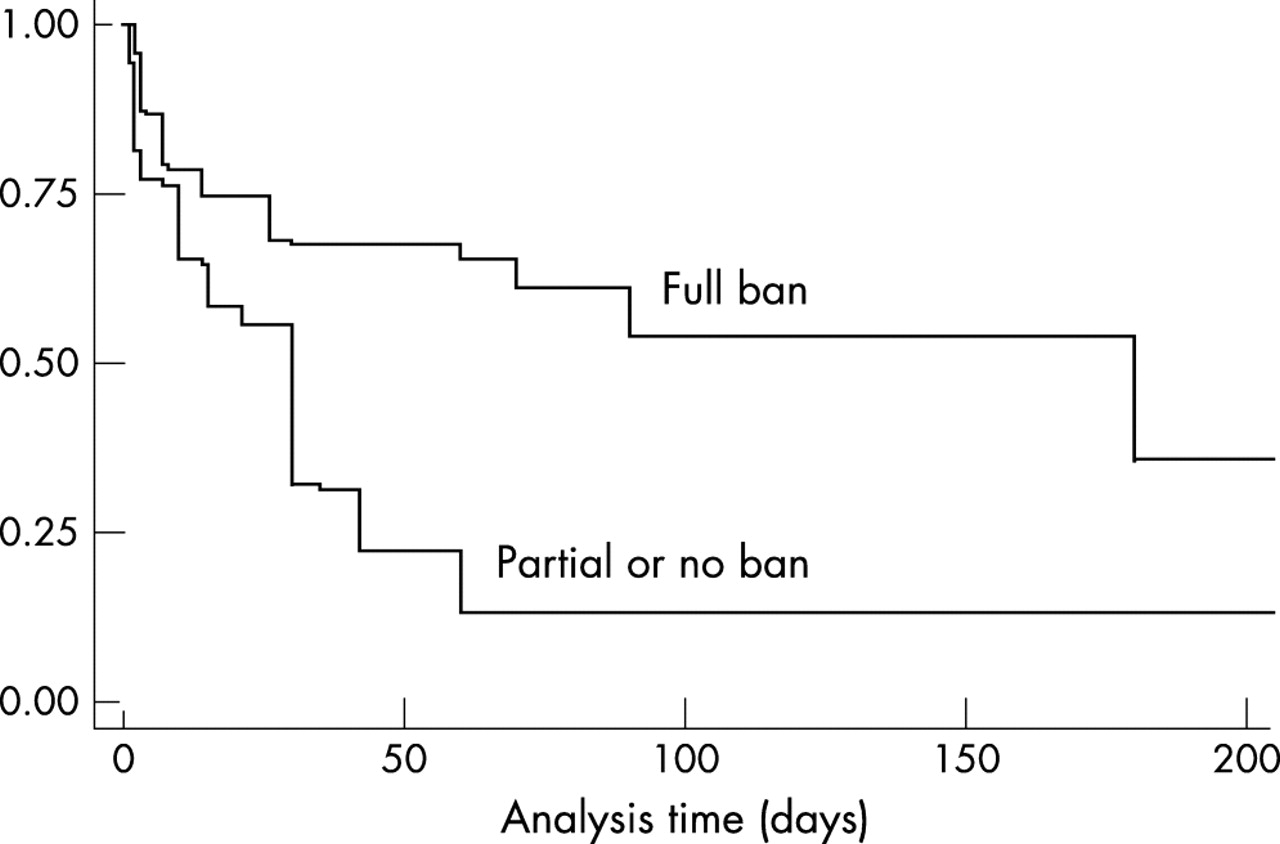
Kaplan–Meier survival curves for days to relapse to smoking by household ban status among 82 respondents in the preparation stage at baseline who had quit for at least one day during follow up. The analysis contains all smokers with a quit attempt; however, survival curves are truncated at six months to illustrate earlier, more frequent relapses better. One respondent had missing information on length of quit attempt. The difference between the curves is significant (p = 0.02).

{kind=link}
{kind=link}
Kaplan–Meier survival curves for days to relapse to smoking by household ban status among 281 respondents in the precontemplation or contemplation stage at baseline who had quit for at least one day during follow up. The analysis contains all smokers with a quit attempt; however, survival curves are truncated at six months to illustrate earlier, more frequent relapses better. Seven respondents had missing information on length of quit attempt. The difference between the curves is not significant (p = 0.95).
Prevalence of sustained abstinence at follow up call
About one fifth of the cohort (n = 115) had been abstinent from smoking for at least one day at the follow up call. A total of 2.4% had quit less than seven days before, 16.1% at least seven days but less than three months before, 19.4% at least three but less than six months before, 30.1% at least six but less than 12 months before, and 32.0% 12 months or more before the follow up call
Household smoking bans, stage of change and cessation (sustained abstinence at follow up call)
We found that the relation between ban status and sustained abstinence at follow up for at least seven and at least 90 days was modified by stage of change of the smoker at baseline (p = 0.05; table 3). Among persons in precontemplation or contemplation, a full ban had no significant association with seven day quits. Among those in preparation with a full ban in place, however, the odds of a seven day quit at follow up were over four times greater than those with no ban or a partial ban, after adjustment for demographics and baseline consumption (OR = 4.4 (95% CI 1.1 to 18.7)). Respondents who were in cessation for at least 90 days at follow up followed a similar pattern: among smokers in the preparation stage, those with a full ban also had over four times the odds of quitting compared with those with no ban or a partial ban (table 3).
Odds ratios for full household ban and smoking cessation for at least seven and at least 90 days, within strata of stage of change*
DISCUSSION
In this population based longitudinal study we observed that a full ban on household smoking was associated with a subsequent quit attempt, and was related to successful cessation among smokers who were in the preparation stage of the stage of change. A full household smoking ban was also associated with longer quit attempts for these respondents. For those not in the preparation stage, a full ban was essentially unassociated with increased odds of cessation or with longer quit attempts.
The findings of this study are subject to several limitations. With only participants’ first name and baseline phone number, we were unable to trace many non-respondents and therefore had a substantial loss to follow up. However, the percentage of baseline respondents lost to follow up in this study is comparable to several of the population based longitudinal studies conducted by the US Census Bureau.19 Much of the attrition in those studies, as well as in ours, was caused by inability to locate respondents. This is an increasing problem owing to the high geographical mobility of the US population (16.5% of the population moved between March 1996 and March 1997).20 This mobility rate is consistent with our data—of the 45% lost to follow up, 10% refused, and 35% could not be located after a two year period.
The comparability between our follow up subjects and the baseline group depended on factors such as age, race, income, and marital status, as shown in other studies on non-response.21–24 For these reasons, we used these variables to reweight the data to correct for some degree of non-response. This technique, however, also introduced somewhat greater variability into our estimates.
We had no way of validating the exposure (household smoking restrictions) or the outcomes (smoking cessation and other smoking behaviours) in this study. Self report of quit status, however, has been shown to be generally accurate except in special populations not represented in this study.25 We have previously suggested that differential misclassification of household smoking restrictions may occur contingent upon smoking status of the respondent.13 This was not a problem at baseline in this study as all the respondents were smokers. However, if smokers with bans at baseline were more likely to indicate quitting at follow up than smokers without bans through a tendency to report a socially desirable response, a bias could occur.26 The prospective nature of this study, however, may mitigate against this bias to some degree, as exposure information (ban) was collected 21 months before follow up smoking status.
Quit attempts, time until relapse, and smoking cessation
Only a few other reports—all cross sectional in design—have investigated whether smoking related outcomes were associated with household bans. Gilpin et al,4using data from a population based California tobacco survey, found that home smoking restrictions increased the likelihood of a quit attempt, and that given an attempt, a ban appeared to prolong time to relapse. Farkas et al also documented a fourfold increase in odds of a quit attempt associated with full household restrictions.6 Norman et al observed that household bans were related to an interest in quitting and the number of quit attempts in the previous year.5 Though these findings are consistent with ours, no investigation has been prospective in nature or has addressed whether smokers’ stage of change might play a role in the relation between smoking restrictions and changes in smoking related behaviour.
Previous work has established the importance of the length of a quit attempt as a predictor of subsequent success in quitting,8 and we observed that a full ban tended to lengthen quit attempts for abstaining smokers. As noted, this finding was generally in agreement with Gilpin’s study, although she did not note a modifying effect of stage of change. Other studies on relapse have noted that exposure to a smoker acts as a “cue” and promotes relapse,27–33 and that a non-smoking environment aids abstinence.34 A smoke-free household limits exposure to smoking cues from household members and visitors who might be smokers.
Only one of the above studies investigated an association between household bans and smoking cessation. Farkas et al,6 using data from the Current Population Survey, found that persons living in households with a full ban were almost twice as likely to have quit smoking in the previous year than those without a ban. Our results confirmed this association, but only within the subgroup of respondents who were in the preparation phase of the stage of change. The stage of change model has been used to match different types of interventions to smokers at different stages, thus more efficiently targeting groups susceptible to change.35–39 For example, the Clinical Practice Guidelines for Treatment of Tobacco Use and Dependence published by the US Public Health Service40 recommend assessment of every smoker for willingness to make a quit attempt in the next 30 days, and stage matched intervention. Under the guidelines, a provider employs pharmacotherapy and behavioural counselling for a patient in the preparation stage, but uses motivational intervention for a patient in the precontemplation or contemplation stages. Some telephone quit lines also screen callers for readiness to quit to deliver appropriate interventions.41 Our finding that the association between a household smoking ban and quitting is most pronounced among smokers in preparation could be useful in either of these settings if further research points toward a causal relation between bans and quitting.
We do not know from this study whether the home restrictions facilitated movement into the preparation phase or vice versa, as information on both of these variables was collected from the cross sectional baseline survey. On the one hand, household restrictions may lead to preparation by decreasing the convenience of smoking; on the other, those in preparation and already thinking of quitting may be more inclined to establish a household restriction. Although further studies might clarify the direction of this association for purposes of public health interventions, the fact remains that in either event the combination of the ban and preparation was more highly associated with cessation than the preparation stage alone.
Conclusions
We found that household smoking bans were associated with increased quit attempts. Furthermore, full bans were associated with a longer duration of those attempts and more frequent sustained abstinence at follow up, as long as the smoker intended to quit in the short run. Further research on this link is important because of potential applicability in both client focused settings and population based approaches. In clinical and help-line settings where smokers are screened for readiness to quit, health care providers could encourage household restrictions, if these restrictions continue to show promise as an aid to quitting. Also, if further studies confirm the relation, mass media messages that target smokers and non-smokers alike could emphasise both the secondhand smoke protection message and the possibility that restrictions might assist the smoker in the long process of successfully becoming a non-smoker.
What this paper adds
Several cross sectional studies have documented an association between home smoking bans and reduction in smoking related behaviours (lighter smoking, cessation, reduced risk of relapse). To our knowledge, however, no report has examined this relation longitudinally.
This follow up study suggests that among smokers who are preparing to quit, those living with full bans may subsequently quit more often than those living without them. If further research should show this association to be causal, the promotion of smoking bans could be useful in both client focused and population based approaches to smoking cessation.