Article Text

Abstract
BACKGROUND Since the passage of a voter approved state referendum in 1992 to establish a 25 cent increase on the excise tax on cigarettes and smokeless tobacco, Massachusetts has received an average of $40 million annually for its tobacco control programme. This funding allowed Massachusetts to expand and develop its tobacco control programme to become one of the most comprehensive in the world.
OBJECTIVES The development of the Massachusetts Tobacco Control Program is outlined, focusing on three stages of development: formation, strategic partnership building, and shared leadership.
METHODS The development of management structures, programmatic infrastructure, communication and partnership networks, and advisory structures are tracked throughout the three phases.
RESULTS The use of pre-existing public health resources, implementation of a strong training component, a geographical management structure, the creation of public and private partnerships, and the development of a shared leadership model contributed to building consensus and provided the foundation for coordinated approaches to tobacco control.
CONCLUSION Other states and countries can use lessons learned from Massachusetts about the organisational development of a comprehensive tobacco control programme as they embark upon similar efforts.
- Massachusetts
- infrastructure
- system development
- tobacco control programme
Statistics from Altmetric.com
More than 10 000 Massachusetts residents die each year as a result of tobacco use. In November of 1992, a voter approved referendum, Question 1, established the Health Protection Fund with revenue generated from a 25 cent increase in the excise tax on cigarettes and smokeless tobacco.1-3 An average of $36 million annually from the Health Protection Fund is used for the Massachusetts Tobacco Control Program (MTCP) for media, community based programmes, statewide projects, and research and evaluation. MTCP is designed to curtail tobacco related health risk in three ways: (1) persuade and help smokers to stop smoking; (2) prevent young people from starting to use tobacco, interrupt habituated use, and reduce youth access to tobacco products; and (3) protect non-smokers by reducing their exposure to environmental tobacco smoke (ETS).
State public health programmes develop and evolve over time. The role of public health departments is to develop environments and programmes that support healthy communities.4 This is the story of the organisational changes that occurred as the MTCP evolved from a small group of tobacco control advocates and grew to include 97% (338) of the cities and towns in the Commonwealth. Before Question 1 was passed, the Massachusetts Department of Public Health's (MDPH) tobacco control effort was confined to a small ($420 000), federally funded, National Cancer Institute (NCI) tobacco control policy research initiative.5 With the new influx of dollars, MDPH designed its tobacco control programme to integrate into Massachusetts' large and complex public health service system, utilising the scientifically based NCI policy model and elements of California's programme.6
Since the programme began, MTCP crossed geographic, institutional, and programmatic boundaries, creating a social movement that reduced cigarette consumption in Massachusetts by 31%, three times the national average.7 The process occurred in three overlapping phases: (1) formation (1993 to 1994); (2) strategic partnership building (1995 to 1997); and (3) shared leadership (1998 forward). Figure 1 shows a timeline describing the development of MTCP.

Timeline of MTCP development.
This article details the evolution of MTCP, tracking the development of management structures, programmatic infrastructure, communication and partnership networks, and advisory structures through the three phases.
Phase 1: formation of a statewide tobacco control programme
The characteristic of the first stage of the excise tax era was formation, which occurred from late 1993 through 1994. MTCP began with an award winning, $14 million media campaign to inform the public about the dangers of smoking and of exposure to tobacco smoke. It included television, radio, newspaper, and billboard advertising, and public relations efforts throughout the state.8
A major expansion of tobacco control required the integration of the programme into the existing public health system. In Massachusetts, the public health system includes a public/ private partnership system of hospitals, health centres, local boards of health and city health departments, community-based agencies and schools. Public health services are delivered through contracts, with the goal of providing a coordinated system of care at the community level. The process of integration began with a major, $14 million public bid for community based policy and programme initiatives, bringing programme dollars to communities quickly.9 An additional $6 million was allocated to fund statewide capacity building projects to support or enhance community based programmes such as a clearinghouse, quitline, and technical assistance and training projects designed to guarantee that a new cadre of tobacco control professionals would emerge. An evaluation plan to assure accountability was also put into place. (See the MTCP website for a description of MTCP programmes—www.state.ma.us/dph/mtcp.)
At this time, MTCP consisted of a small core staff. MDPH made a substantial commitment to provide necessary resources for programme start up, including providing staff to MTCP. MDPH staff were essential to managing the public bid and programme start up process. Figure 2describes the phase 1 organisational structure and the array of statewide, regional, and local programmes resulting from the public bid. During this time, state management was immersed in the difficult task of establishing a statewide tobacco control programme in a matter of months. Figure 2, reflecting this preoccupation, describes an incomplete organisational structure, depicting only MDPH contractors.10 Statewide, regional, and local programmes were grouped categorically by programme type. During the initial stage of development, organisational structures and mechanisms such as steering committees and strategic planning processes, linking programmes across geographic and programmatic boundaries, did not yet exist. Many stakeholders who were actively influencing tobacco control policy in the state were missing from the picture—for example, the Oversight Council, an advisory group of health professionals who were active in passing Question 1, and the Department of Education, which shares responsibility for reducing youth smoking rates, were two important missing players.

Phase 1: formation.
Once start up was completed, the challenge was to shift to programme implementation and a management model that would support ongoing operations. Up until this point, local, community based programmes were managed centrally by MTCP with a contract manager assigned to each programme type (modality) (see fig 2, local programmes.) Information about DPH policies such as contract and monitoring requirements were exchanged at large group provider meetings that were convened statewide by modality. While a centrally managed organisational structure was suited to a public bid and start up, it was not efficient at mediating conflicts and facilitating communication at the local level. For example, if there was a conflict between programmes in a community, managers representing each modality had to be involved in its resolution. The absence of locally based MTCP managers sometimes delayed the resolution of problems, increasing tension within communities and between the state and local programmes.
The major accomplishments of the formation phase were the creation of an award winning media campaign, the institution of new tobacco control programmes across the entire state resulting in dollars reaching communities quickly, and establishment of tobacco control professionals within a variety of public health settings. Building programme capacity and strategic partnerships and alliances were the next order of business. Programme models had to be crafted within demographically and politically unique community settings. Communities did not always have a full range of tobacco control services because the public bidding process did not produce applicants in all service categories. Additionally, limited dollars meant that resources were spread thinly. Tobacco control programmes were small, often with only one full time staff person who was unfamiliar with the demands of working in a publicly funded programme. Executive directors and supervisors at funded community based agencies were generally new to tobacco control so staff worked with minimal supervision and agency support. Building and expanding the tobacco control movement in Massachusetts required developing a highly collaborative network of programmes and strategic partnerships. This work, so essential to institutionalising—that is, firmly establishing—a tobacco control programme within the public health system became the focus of phase 2.
Phase 2: building strategic partnerships
In response to the conditions described above, the operating model changed in year 2 (1995 to 1996) from a focus on programme type, each developed and administered separately, to a geographic model that knit community based programmes together within regional boundaries. The MTCP reorganised its tobacco management structure and created a field operations unit, replacing programme specific managers with regional field directors who managed contracts in each region and organised local programmes funded by MTCP into six regional networks. Monthly regional meetings, convened by MTCP regional field directors, were designed to serve as a forum for regional action planning, information dissemination, provider collaboration and training. When reorganising its management team, MTCP hired regional field directors who had experience working in local tobacco control programmes. This helped build trust and a spirit of partnership. MTCP also brought in a senior manager, seasoned in public health system development and programme operations. The mixture of MTCP managers helped increase understanding between the field and the state. Figure 3 describes the partnership building phase, which marked a period of increased collaboration and strategic planning.

Phase 2: strategic partnership building.
REGIONAL COLLABORATION
Each of the six regional networks is guided by a steering committee that works on goal alignment, strategic planning, regional public relations campaigns, and quality improvement. Steering committees are comprised of representatives from local and regional programmes and MDPH managers representing other segments of the public health service system, such as substance abuse and family and community health services. Also represented are the American Cancer Society and the Department of Education, two important organisations influencing tobacco control policy and programme implementation. Regional networks and steering committees crossed programme and system boundaries by bringing an average of 40 programmes together on a monthly basis in each region, and combining public agencies and private sector entities in new collaborative models. The concept of boundary crossing networks11 began to shape MTCP's organisational structures.
The regional structure also provided an ideal backdrop for undertaking large and complex projects with multiple participants, increasing the impact of activities. Project management seminars were held with steering committees and regional networks to furnish the tools to assess the efficacy of proposed projects and provide the organisational skills needed to implement large group projects.
Projects were designed and implemented across both modalities and regions and engaged partners outside of the MTCP system. For example, two regions collaborated with Clark University to design a survey of community attitudes toward environmental tobacco smoke (ETS). This survey reached 50 000 households and provided community specific information for use at local public hearings on ETS regulations. In another project, several regions participated in a basketball shooting competition, “Hot Shots”, that promoted a healthy, tobacco free lifestyle to students and educated them about the dangers of secondhand smoke. The state championship included 44 communities and reached approximately 20 000 children and their families. In another example, boards of health, prevention centres, and the Department of Education collaborated in one region to pilot a school tobacco policy forum to develop effective strategies to implement tobacco free schools. These policy forums were then replicated in other regions.
PROGRAMMES RESTRUCTURED
In the summer of 1997, the Department of Public Health conducted a public rebid of services and important changes occurred in the model, productivity goals and contract outcome measures.12Targeting dollars to areas where there were greater numbers of smokers and very complex social conditions that made policy and programme objectives more difficult to achieve was a theme throughout the rebid.13 Based on experience, traditional public health prevention programme models were adjusted so that they could better achieve MTCP policy objectives. For example, peer leadership programmes were refocused toward activities that supported limiting youth access to tobacco products. A funding formula was developed by MTCP for local boards of health and health departments that distributed money by population, as in the past, but also provided for enhancements for percent of poverty and the scope of tobacco control work undertaken.14 For example, boards of health could choose to engage in a range of activities to accomplish both youth access and environmental tobacco smoke policy objectives outlined in the public bid that preceded contracting. Boards that submitted proposals to undertake important, and sometimes controversial, environmental tobacco smoke initiatives received more funding than a board that avoided the issue because of opposition stimulated by the tobacco industry and its operatives.
Another outcome of the rebid was the alignment of smoking cessation programmes with healthcare industry performance and financing standards. MDPH has had a longstanding commitment to assist individuals in recovering from addictions through a publicly funded alcohol and drug treatment system. MDPH expanded this commitment by funding 48 smoking cessation programmes in a variety of health settings across the state as well as a programme development and technical assistance programme at the University of Massachusetts Medical Center. Although the model originally funded was a casefinding model (NCI 4A model—ask, advise, assist, arrange15 16), before the rebid smoking cessation programmes delivered a broad range of activity, heavily focused on outreach and community education. The number of counselling services provided directly to smokers was low. Services were primarily organised around the 4A case finding model with the expectation that cessation counsellors would implement the model within their institution and provide individual and group counselling services to those in need. Site visits revealed that cessation counsellors were isolated within their healthcare settings and had difficulty getting referrals from other caregivers within their institutions, primarily health centres and hospitals. Smoking cessation counsellors did not have the authority or the attention of management to implement the 4A model within their institutions.
As part of programme restructuring, MTCP used behavioural health cost models that link payment to productivity, developing reimbursement rates for a 15 minute 4A intervention with a smoker, individual counselling, group counselling, and a large group educational lecture.17 Standards for record keeping were also established. Reimbursement for smoking cessation programmes moved from compensation for actual expenses incurred to a reimbursement system based on delivery of a unit of service (for example, a 15 minute counselling intervention). Utilising unit rate billing structures, similar to those used by the state and other insurers for outpatient substance abuse treatment and mental health services, helped institutionalise the 4A model within healthcare facilities. Billing data showed more referrals to cessation services, significantly increased programme productivity, and improved integration of cessation services within health facilities.18
The need for professional standards for counsellors was also addressed through the development of a cutting edge, competency based counsellor certification programme project funded at the University of Massachusetts Medical Center for tobacco treatment specialists (formerly called cessation counsellors). This project, which was piloted in the spring of 1999, is highly supported by tobacco treatment specialists providing services within healthcare settings, who identify training as critical to achieving positive outcomes with the more complicated cases they are seeing in treatment.
Throughout phase 2, emphasis was placed on strategic planning. Local programmes developed result focused contract workplans and coalitions linked programmes to one another, facilitating partnerships and creating formal community action plans. The contract scope of services and roles of local programmes were carefully defined to maximise efforts and avoid duplicating services. System wide training was designed based upon an analysis of the competency needed to do a particular job (for example, a coalition or board of health programme director, youth advisor or tobacco treatment specialists) and a skill based survey of the needs of programme staff and managers. A consultant was engaged to work directly with steering committees to develop their capacity to collaborate, strategise, and lead.
STATEWIDE COLLABORATION
In phase 1, the statewide media campaign and public relations effort was instrumental in educating and influencing public opinion, but it was not sufficiently synchronised with local activities. Collaborative public relations activities increased in phase 2 when MTCP, through its media contractor, Arnold Communication, allocated $750 000 over a two year period to steering committees to support local public relations initiatives. This created greater synergy between the statewide media campaign and communities. Through regional steering committees, for example, Arnold Communications developed eight radio messages for a region wide quit campaign using a mayor, city councilor, city commissioner of health, city manager, fire chief, police chief, school superintendent, and state representative. The same steering committee organised a partnership with 142 physicians that, in a full page advertisement listing each physician by name, urged city and town officials to adopt ETS regulations and ordinances. Two regions also collaborated with Arnold Communications and translated ETS advertisements into 10 languages including Spanish, Portuguese, Khmer, Laotian, Polish, Vietnamese, Armenian, Russian, Cantonese, and Haitian/Creole.19
Another important objective of phase 2 was to emphasise the role of statewide services in assisting or complementing community based efforts. An example of a highly effective collaboration of three statewide projects is the Community Assistance Statewide Team (CAST). Two trade associations and a legal policy project collaborate to assist cities and towns in their efforts to enact laws and regulations. The Massachusetts Association of Health Boards, Massachusetts Municipal Association, and the Tobacco Control Resource Center at Northeastern Law School provide technical assistance to municipalities as tobacco control laws and regulations are introduced in their communities.20 For example, they review all local regulations and provide advice to city solicitors in order to help them avoid costly litigation with the tobacco industry.
In Massachusetts, a community based strategy is an ideal vehicle for social change. The tobacco industry is generally more able to influence public policy at the federal and state levels and is less able to influence local elected officials.21 22 The Home Rule Amendment of the Massachusetts Constitution grants cities and towns broad legislative authority.23 Massachusetts' statutes also give broad power to local boards of health to act to protect public health through regulation and enforcement activities. MTCP developed in a “home rule” atmosphere that supports the right of cities and towns to self govern and guide public policy.
MTCP grew to include over 232 programmes in 338 (of the 351) cities and towns in Massachusetts. Along with the growth of community based programmes came a more complex policy environment. Until this point, a small number of nationally recognised and highly vocal tobacco control advocates dominated statewide policy discussions. The need for leadership to represent all stakeholders affected by public policy decisions was clear. As the programme expanded and infrastructure developed, it was essential that organisational structures adjust to assure that the entire tobacco control community worked toward the same goals and not at cross purposes.
A warning note sounded when some advocates pressed forward with a state youth access law against the advice of the legal policy experts, CAST, who worked closely with local boards of health and health departments. The bitter disagreement between tobacco control advocates that followed undermined their credibility with the legislators who had been encouraged to sponsor the bill. The bill, in conflict with a home rule strategy, was eventually dropped. As a result, the Massachusetts Coalition for a Healthy Future (Healthy Futures), which led the campaign to pass the tobacco excise tax in 1992, reorganised its legislative leadership to include legal policy experts representing the field.
It was also critical that those working on projects operating parallel to state programmes, such as tobacco control research initiatives funded by the federal government or foundations, be fully informed and linked to MTCP. It was particularly important that national experts and advisors living in Massachusetts feel that they were part of Massachusetts' tobacco control effort. Including all stakeholders helped assure that both researchers and community based programmes benefited from the expertise and resources available in the state and that accurate information about the MTCP was presented at meetings and conferences and in journals. These needs ushered in phase 3.
Phase 3: moving toward a shared leadership model
Phase 3 brought with it a gubernatorial election and appointment of a new commissioner of the Massachusetts Department of Public Health. Tobacco control advocates were also adjusting to major change within their own organisations. For example, Healthy Futures appointed a new chair. The Oversight Council, an external group of advocates advising the department on the use of Health Protection Funds, in an effort to be more inclusive, renamed itself the Health Protection Fund Advisory Committee and expanded its membership, reorganised, and chose new leadership. Change created instability and uncertainty, but it also created opportunities for new leaders to emerge and brought people together in new ways.
The Health Protection Fund Advisory Committee reorganised into five subcommittees representing the most important components of MTCP: media; school/youth; cessation; research and evaluation; and policy and regulation. Healthy Futures agreed to serve as the policy and regulation subcommittee of the Health Protection Fund Advisory Committee. Subcommittees became a mix of university based tobacco control researchers, directors of tobacco control programmes, and advocates.
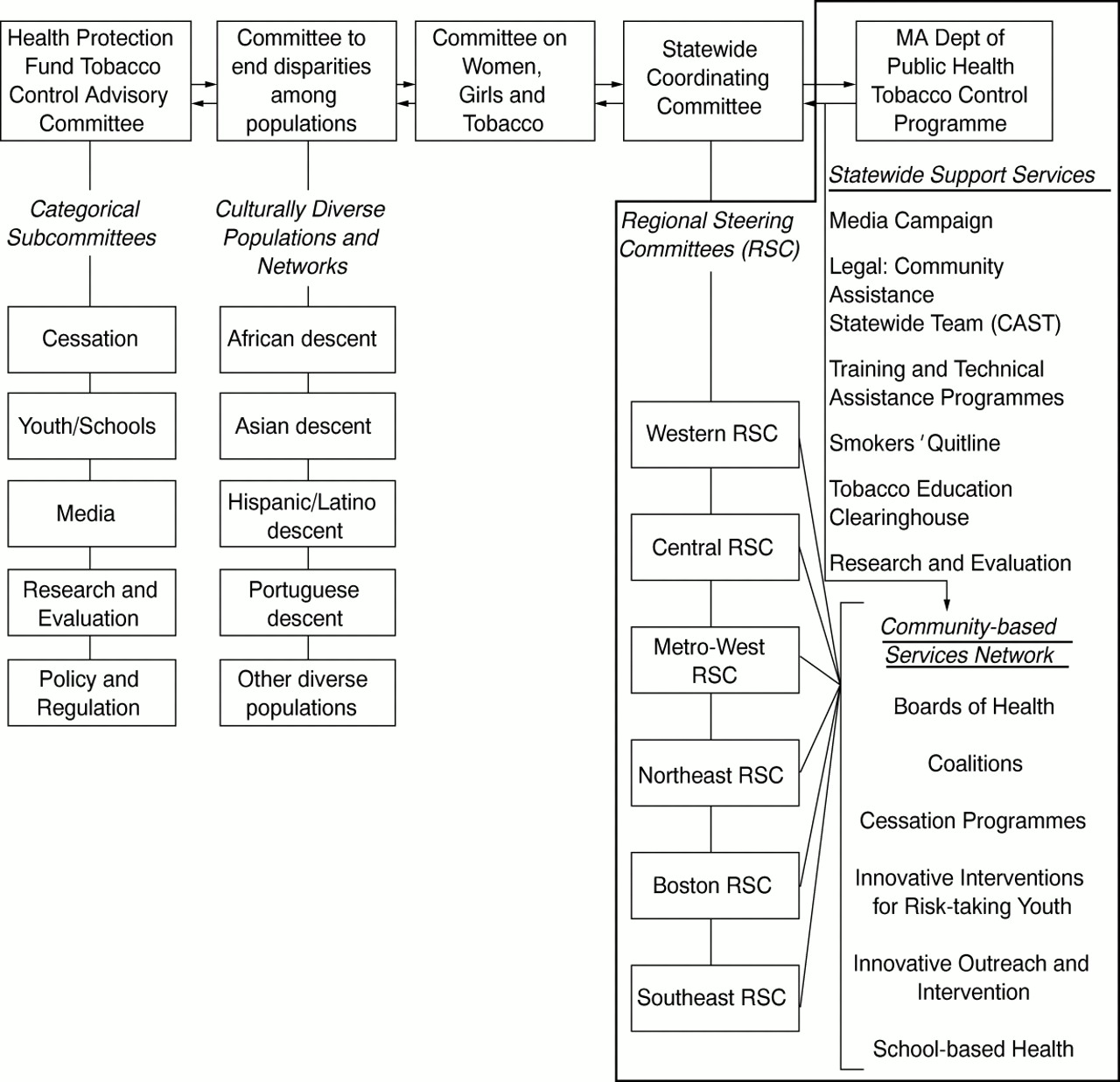
A leadership model emerged that was significantly more inclusive, representing all parties and stakeholders. Three new advisory committees were added at a level equal to the Health Protection Fund Advisory Committee: the Committee on Women, Girls and Tobacco; the Committee to End Disparities Among Populations which represents minority communities; and the Statewide Coordinating Committee which represents all MTCP community based programmes. In fig 4, for the first time all stakeholders are included on the organisational chart, communication lines are open, and all have a voice in the decision making process: researchers, advocates, public health professionals, and community based programmes. Community networks crossed institutional, geographic, and programmatic boundaries.

Phase 3: shared leadership.
The work attendant to implementing a shared leadership model began in November of 1998 at a statewide summit which officially inaugurated the model. Over 500 people attended and in breakout sessions began to examine strategies to address the trends and challenges facing each committee and its subcommittees.
In February 1999, the Department of Public health convened a statewide leadership training for Regional Steering Committee members. The training centred on defining leadership and the skills and qualities needed to represent local communities in statewide policy discussions. Under the guidance of an organisational consulting firm, Steering Committee members assessed their own individual leadership skills from which leadership profiles were developed and training needs identified. The day ended with each Steering Committee electing their representative to sit on the Statewide Coordinating Committee, an external committee to the Department of Public Health advising the department on tobacco control issues facing community based programmes.
At the same time, the Committee to End Disparities Among Populations and the Committee on Women, Girls and Tobacco were also actively organising to advise the department on issues facing women and girls, ethnic and linguistic minorities, and other diverse populations disproportionately affected by tobacco use. The Health Protection Fund Advisory Committee chairperson called an initial meeting of all committee and subcommittee chairpersons, opening a line of communication between all partners and stakeholders, signalling a change in the leadership model.
In November the 1999 Annual Tobacco Control Summit, co-sponsored by the American Cancer Society and the Department of Public Health, was held to present the recommendation of the four statewide advisory committees and celebrate the success of the MTCP. Since the programme began, consumption had decreased by 31% and smoking prevalence by 10%.7 24 Also, Massachusetts was one of only a few states in the nation to allocate significant Master Settlement Agreement (MSA) dollars for tobacco control. TheYear 2000 Recommendations presented during the day were the culmination of a year of collaboration that began at the 1998 Annual Tobacco Control Summit. Seven themes emerged from the advisory committees and subcommittees: (1) support local community based tobacco control efforts; (2) continue a strong social marketing effort to counter industry advertising; (3) prioritise cultural competency in all programme development efforts; (4) continue to support the development and implementation of strong ETS regulations; (5) provide a full range of tobacco treatment services; (6) expand research and evaluation efforts; and (7) increase collaboration with schools to develop new tobacco control interventions for youth.25 These themes will guide the department in spending MSA dollars and inform future programme development efforts.
Recommendations and lessons learned
New programmes take time to develop. The evolution of MTCP involved gradual change in organisational structures and networks. Figure 5 summarises MTCP's development in four critical areas: management structures; programmatic infrastructure; communication and partnership networks; and advisory structures. Success depended on building consensus among stakeholders working in these networks and structures.
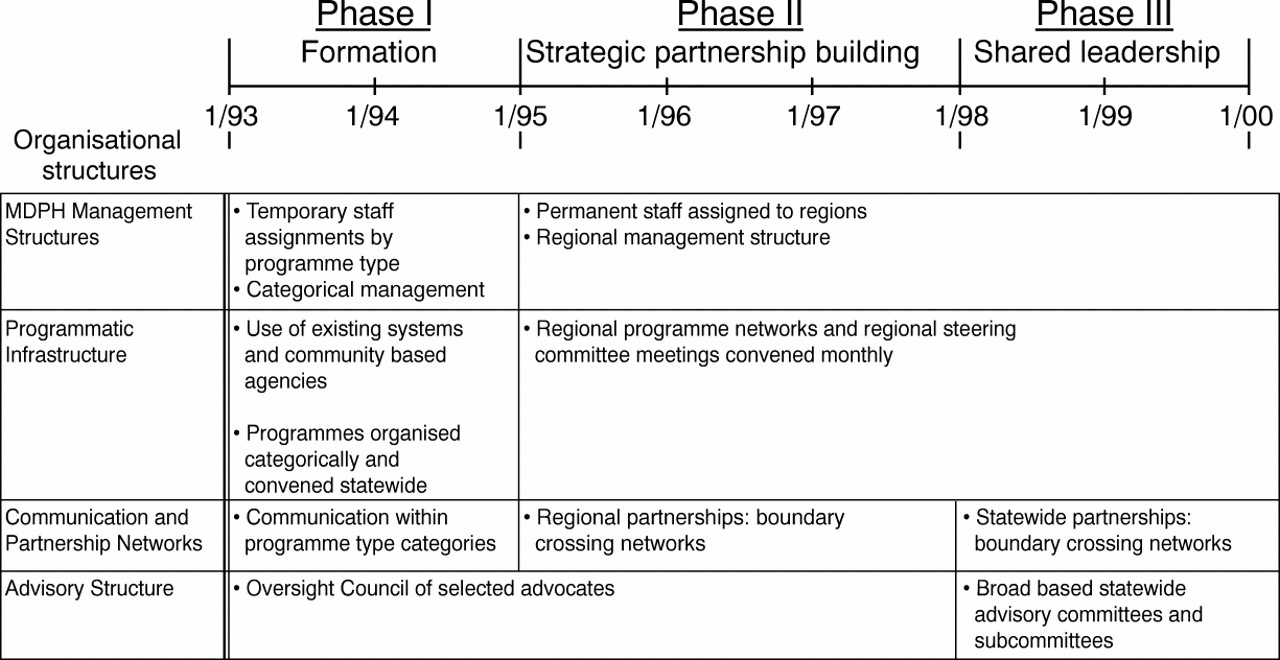
Evolution of organisational structures and networks.
MTCP would not have been able in the first year to utilise health protection funds fully without using existing public health resources, especially personnel from other departments who supported the public bidding process and start up. Using staff from other parts of MDPH facilitated integration into the public health system. Building on and integrating into existing public systems is essential to developing a cost effective programme and reaching at-risk populations.
However, tobacco control is a new field. Much thought and effort must be directed to building the capacity of existing systems, through state-of-the-art training and technical assistance, to implement tobacco control policy and programme objectives. Also, dedicated tobacco control state managers and staff are critical to the organisation, management, and coordination of state funded programmes. Tobacco control advocates, legislators, and other state officials can assist states in developing tobacco control programmes by funding public health infrastructure.
Geographic management structures facilitate communication and allow for a more organised approach to planning and strategy development. Recognition of regional differences through regional structures facilitates communication and information exchange and allows for different voices to be heard and recognised. Management structures should support a two directional approach (top down, bottom up) as well as create opportunities for diverse populations to communicate across geographic and programme boundaries.
Developing advisory structures that bring together stakeholder groups is critical. Developing a culture that respects and values communication and collaboration helps tobacco control programmes to withstand industry opposition and allows conflicts between natural allies and friends within the state to be resolved quickly.
Massachusetts is making progress toward attaining a shared leadership model, giving all stakeholders a voice in the decision making process. More and more, those in the role of influencing public policy and those making public policy decisions are considering the opinions of the MTCP programmes working on the front line to change individual and community attitudes and behaviours.
Opening lines of communication has increased understanding among advocacy groups, funded programmes, and the academic community about the knowledge and concerns of each group. It has also improved understanding about the roles of advocates, researchers, government, and the community in policy development and increased participation of women and ethnic, linguistic, and cultural minorities in policy discussions.
Additionally, a geographic management structure and an inclusive advisory structure have provided forums to disseminate information about the MTCP model and the success of the community based policy initiatives. Increasing awareness of the success of MTCP has helped sustain and increase funding for the programme. Additionally, developing a culture of collaboration was an important factor in uniting the tobacco control community, enabling them to engage other public and private healthcare groups in the advocacy activities that led to the allocation of $22.8 million of MSA funds for tobacco control in Massachusetts' fiscal year 2000 budget.
Clearly, the use of existing public health resources; implementation of a strong training component; a geographical management structure; the creation of private and public partnerships; and the development of a shared leadership model contributed to building consensus and provided the foundation for coordinated approaches to tobacco control. Those engaged in developing state and national tobacco control programmes should consider these strategies.
In Massachusetts, much work remains to be done. Progress will depend on our ability to meet the challenges of the future, including the influx of dollars from the tobacco industry settlement which is changing the tobacco control landscape. Our strategies advance from the premise that a shared leadership model will help us to develop better solutions to the increasingly difficult problems that we face. What are the best ways to engage new partners and expand our influence? Only by including all stakeholders will we have sufficient information, understanding, and state-of-the-art technology to address problems such as high smoking prevalence in low income urban and rural communities or challenge the tobacco industry's youth marketing practices that continue to persuade children to smoke.26 We must continue to be vigilant and evaluate our efforts in the context of the complex environment within which we work. It is critical that tobacco advocacy groups, researchers, programmes, and communities partner to support adequate funding of tobacco control efforts, and that natural allies in the healthcare field work together to accomplish tobacco control agendas.27 Together we will reach our goal to make smoking history.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bangladesh's version of the Marlboro man: “Karim, I've got cancer from smoking” and a message “Tobacco kills, don't be duped”. Produced by the Bangladesh Anti-Tobacco Alliance.