Article Text

Abstract
Objectives: To provide a participant’s account of the development of a paper commissioned by the tobacco industry examining the reliability of self reported smoking status; to redress the distorted report of this Japanese spousal smoking study which evaluated the reliability and validity of self reported smoking status, and estimated confounding by diet and lifestyle factors.
Design: Repeated interviews on smoking status and its verification by environmental and biological markers for environmental tobacco smoke (ETS) exposure.
Setting: Urban wives in Osaka City and Sizuoka City, Japan
Participants: Semi-random sampling of 200 wives in each city. From the Osaka subjects, 100 non-smoking wives were selected for the validity study.
Main outcome measures: Kappa coefficient for reliability of self reported smoking status. Correlation coefficients between environmental nicotine concentration, cotinine in saliva and urine, and self reported smoking status.
Results: The κ coefficient for the repeated interview was high suggesting sufficient reliability of the response. The proportion of self reported current smokers misclassified as non-smokers was equivalent to the misclassified self reported non-smokers. Ambient concentration of nicotine and personal exposure to nicotine correlated with each other and also with salivary cotinine and self reported ETS exposure but not with urinary cotinine/creatinine ratio (CCR). There was no major difference in diet and lifestyle related to husband’s smoking status.
Conclusion: Self reported smoking status by Japanese wives shows high reliability. It also shows high validity when verified by both nicotine exposure and salivary cotinine, but not by CCR. A previous report questioning the credibility of self reported smoking status, based on questionable CCR, could thus be of dubious validity. In addition, possible dietary and lifestyle confounding factors associated with smoking husbands were not demonstrable, a finding not reported previously. Using all the data from this project changes the conclusion of the previous published report. In addition to the distortion of scientific findings by a tobacco industry affiliated researcher, anti-smoking campaigners made attempts to intimidate and suppress scientific activities. These distortions of science should be counteracted.
- CCR, cotinine: creatinine ratio
- ETS, environmental tobacco smoke
- IEMC, International ETS Management Committee
- anti-smoking campaigns
- confounding
- misclassification
- tobacco industry
Statistics from Altmetric.com
- CCR, cotinine: creatinine ratio
- ETS, environmental tobacco smoke
- IEMC, International ETS Management Committee
There has been an extensive, controversial, and vociferous debate over the possibility of the causal association between exposure to environmental tobacco smoke (ETS) and lung cancer. The issue was precipitated by the publication of Hirayama’s large cohort study from Japan.1 He demonstrated a twofold increase in the risk of lung cancer among non-smoking wives with heavy smoking (20 or more cigarettes/day) husbands compared to those with non-smoking spouses. However, this study has been the target of scientific and methodological criticism including that of Mantel2 who criticised the inappropriate application of his method of summarising χ statistics. Part of the reason for these criticisms arose from the brevity of Hirayama’s original publication, which did not include comprehensive information. When the detailed figures of the various confounding factors, reported in a Japanese journal by Hirayama, were used for the calculation to obtain χ statistics after stratification, his analysis was confirmed and the statistical criticisms were rebutted.3,4
However, following Hirayama’s publication, another large cohort study performed by the American Cancer Society found no or very little association between ETS exposure and lung cancer.5 The author of that study queried cultural differences between study subjects, claiming that more Japanese than American women may conceal their smoking, meaning that some active smoking women may have been misclassified as passive smokers in the Hirayama study. Since women smokers tend to marry men who also smoke, it may be expected that there would be a higher incidence of lung cancer in wives of smoking husbands compared to those of non-smoking husbands. The possibility of confounding unhealthy dietary and lifestyle aspects more frequently occurring in families with smoking husbands was also raised as an additional explanation to explain the findings contrary to the Hirayama study.
PART 1: CHRONOLOGY OF A TOBACCO INDUSTRY FUNDED STUDY
In 1991 Dr Christopher Proctor, a British scientist then employed by the Covington and Burling law firm in Washington DC, invited me to become principal investigator on a study designed to evaluate the extent of this potential misclassification and confounding. Proctor is now British American Tobacco’s head of science and regulation. The 2002 publication of Hong and Bero6 made the mistake of assuming that the study was originally initiated by me. I was aware from the beginning that the tobacco industry was funding the project.7 Consequently, I repeatedly requested and was verbally assured by Proctor that despite the commercial source of the funding the observed scientific facts ascertained by the study would be respected absolutely.
The field work for the study took place in the autumn of 1991, with a second phase in June 1992. Proctor was provided with the data in March and August 19928 in the expectation that he would be a co-author with me and my Japanese colleague Professor Jun Kagawa, the two principal investigators. I received a draft paper via fax from Proctor on 14 October 1992.9 There was no list of authors on this draft. Shortly after I received the draft, Proctor and I spoke by phone where I questioned his interpretation of the data on misclassification and to illustrate my point I sent a fax to him on 27 October 1992.10
I received another draft from Proctor on 31 October 1992 which showed my name as sole author.11 In his cover letter, he accepted his overstatement (“Here is a revised version… with the conclusions somewhat watered down”) and changed the focus from misclassification to confounding in the text. I received a third draft on 10 November 1992 in which text in the “misclassification” section of the Results was further deleted and the previous statement “The misclassification rates in this study are somewhat higher than those reported in similar studies of Western populations” had disappeared only to reappear in the final published version12 authored by Peter Lee (see below).
The publication of Hong and Bero’s paper alerted me to the existence of a draft of the paper dated 21 April 199213 bearing my and Kagawa’s names. We did not write any of this draft. Subsequent searching located other drafts dated 28 May 1992 and 25 June 1992, where Peter Lee’s name appeared as third author.14,15 The latter, forwarded to 10 tobacco industry officials, was described by Proctor as being a “close to final” version “restructured” by Proctor and Lee. Again, I never saw these drafts, despite my name being on them. As described, the first version of the paper I saw was on 14 October 1992.
A reference in Hong and Bero’s paper describes how Lee, a researcher with an extensive history of paid consultancies with the tobacco industry, was included in the budget for the study to assist in the study design and in interpreting the data. According to the study plan, it was “not anticipated that Mr Lee will serve as a co-author of any of the publications flowing from the study”.7 At no stage in my interactions with Proctor was Lee’s name or role ever mentioned.
Correspondence from Proctor dated 14 and 21 April 199316,17 states he was working on a further draft of the paper. As described, I had major concerns about Proctor’s treatment of the data I had submitted, as set out in his October 1992 draft. On 7 July 1993, apologising for the delay, I wrote to Proctor requesting that we speak by phone on this.18 My letter stated that the data I had collected challenged the urinary cotinine: creatinine ratio as the gold standard for tobacco exposure and that the questionnaire approach to determining smoking status was “reliable and valid” judging from the concordance of data we had collected from the repeated study and via nicotine monitors. I attached data demonstrating this. I stated that there were therefore “somewhat fundamental issues” we needed to talk about before the paper progressed further. Word about my concerns apparently spread, as notes from a meeting of the International ETS Management Committee (IEMC) at Geneva in June 1993 record: “The Japanese authors [Yano et al] felt uncomfortable about this [the results set out in the draft] and are reluctant to publish it.”19
Again from the Hong and Bero paper, I learned that shortly after I had faxed Proctor about my ongoing concerns, he wrote to officials from six tobacco companies asking permission to remove me as author and have Lee submit the paper to a journal.20 Some time later, I discovered that Lee as sole author had published a report on the study in the International Archives of Occupational and Environmental Health12 without my consent. (Hereafter, I refer to this as Lee’s report to avoid confusion with the original study).
I first became aware that Lee was attempting to publish a report using the data I had collected when, in November 1994, I was approached at a Tokyo meeting by Dr Franz Adlkofer. Dr Adlkofer said he had been asked by the editor-in-chief of the International Archives of Occupational and Environmental Health to review a manuscript which Lee had submitted to that journal based on these data. Adlkofer had previously published with G Lehnert, the journal’s editor.21 Unbeknown to me at the time, Adlkofer was a senior scientist employed by the German tobacco industry’s Verband der Cigarettenindustrie.22,23 A 1983 industry document records Adlkofer as wanting the German industry to financially support Lehnert’s work on cadmium because it was “necessary to maintain Prof. Lehnert’s ‘good will’, with reference to public smoking”.24
At a meeting at Adlkofer’s Tokyo hotel also attended by Ernst Wynder, I explained to Adlkofer the details of the respective roles of Proctor and myself in the study, as described above, and the major concerns I had with the draft paper that I had seen. I explained that as a principal investigator on the study, I had decided not to pursue publication of the study because of the irreconcilable differences I was having with Proctor. He insisted that the study should be published by me and that I should reopen discussions about it with Proctor and Lee.25 After returning to my office I sent a fax to his hotel which illustrated my point about Lee’s misclassification using the Lee’s draft table to explain the scientific disagreement between Proctor and I.26
In these circumstances, I assumed that Lee’s report would not be published. It was only on reading the Hong and Bero paper relating to the background of the study,6 that I realised that Lee’s report12 had in fact been published after being rejected by at least two other journals.27
On 11 April 1995, Lee wrote to the editor of the International Archives of Occupational and Environmental Health stating that he had revised the manuscript to make “it clearer that the study was planned by me with a Japanese scientist and market researcher brought in to help with the fieldwork”.28 This statement, and that which appeared in the published paper, is a travesty of the truth about my role in the project, making me sound nothing more than a translator, technical assistant, and interviewer coach. It says nothing of my principal investigator status nor of the copious computations I supplied to Proctor.
The publication of Hong and Bero6 described the tobacco industry’s intentions in commissioning the study. Most of the facts presented in their paper are in agreement with what I observed, the exception being that the person who proposed the project was Proctor and not me. Although the Hong and Bero report describes the role of the tobacco industry, it does not address the scientific meaning of the results of the study. Being the principal researcher of the study, it was with particular dismay that, on reviewing Lee’s report, I discovered that Lee had both misconstrued the findings of the study and had failed to include in his report major significant results I had supplied to Proctor which did not support the tobacco industry’s position. He even overturned my account of misclassification which Procter accepted. The result of this was that Lee’s report reached conclusions that were totally at odds with the actual findings of the study. In order therefore to attempt to redress the situation, I consider I am obliged to now provide the actual findings of the study and a detailed interpretation of the results.
PART 2: THE “LEE REPORT” REVISITED
METHODS
First phase study (November 1991)
Subjects
A semi-random sampling method was employed to recruit study subjects. In the designated central districts of Osaka City and Shizuoka (erroneously named as Shizoka in Lee’s report12) City, women interviewers from a market research company visited door to door to recruit 200 housewives (aged 20–55 years) in each city. Each agreed to be interviewed and to provide a 50 ml urine sample. A token gratuity (500 yen telephone card) was given in appreciation of their participation. The purpose of the project was explained as a general community health survey and ETS was not specifically mentioned. A second visit was made to collect urine samples, which were frozen and stored at a temperature of −20°C. The samples, contained in dry ice, were sent to the Winston-Salem Laboratory of RJ Reynolds for biochemical analysis. The results of the urine protein and urine sugar, but not the cotinine concentration results, were reported back to the participants by letter, accompanied with supplementary medical advice.
Interview
The interview was performed utilising a systematic questionnaire conducted in person. The smoking status of the subject, ETS exposure at home (smoking by husband, by other family member(s), or both) and that at the workplace, were ascertained by the response to the questions on the tobacco (cigarettes) use questionnaire. In particular, the length of wives’ time spent in close stay with their husbands at home for both weekdays and holidays was sought. In addition, questions concerning food intake frequency (24 items with semi-quantitative food frequency questionnaires) and lifestyle (30 items), as well as self reported exposure to indoor air pollution from kitchen oven and heating, were also asked. At the end of the interview, details of active and passive smoking during the previous 48 hours were requested to double check the ETS exposure status. The interviews generally lasted from 20 minutes to one hour.
Measurement of cotinine: creatinine ratio (CCR)
Urine samples were stored at −20°C until assayed. Urinary cotinine was measured by enzyme linked immunosorbent assay (ELISA) method.29 Urinary creatinine was also measured, and urinary cotinine was expressed as nanograms per milligram of creatinine (ng/mg) (CCR)30 The laboratory cotinine analyses were performed blind to the smoking status of each subject but the overall purpose of the project was recognised.
Second phase study (June 1992)
The purpose of the second phase study was to check the reliability and validity of the first phase study, and also to evaluate any potential confounding bias caused by traffic air pollution. The same subjects who participated in the first phase study were approached and the same interviews repeated, without the urine sample collection. However, for the second phase study, the subjects were asked to self complete a standard questionnaire for respiratory symptoms and the distance of their house from major traffic was assessed using a map.
Exposure monitoring study
With reference to the results of the interview and CCR obtained in the first phase study (1991), 50 non-smoking subjects who were exposed to ETS from their husbands, and another 50 non-smokers with no exposure to ETS, were selected in Osaka for the exposure monitoring study. The subjects were requested to continually wear, except when bathing, a personal nicotine monitoring device for the full seven days. They were also asked to place another similar nicotine monitoring device in their living room. The uptake rate of the device was 31.5 ml/min and the limit of detection was between 0.01–0.02 μg. The concentration of cotinine was measured in both saliva and urine. Using a dental swab, the subjects were instructed to collect saliva samples at the beginning and end of the seven day survey period, and one additional sample on the third day. Urine samples were collected at the end of the seven days. For each of the seven days, the subjects were asked to complete a diary questionnaire about their exposure to ETS, both at home and at work. Special attention was paid to the collection of detailed and accurate information regarding the number of cigarettes smoked by their husbands when juxtaposed to the subjects.
Measurement of nicotine and salivary cotinine
Analysis for the nicotine attached to the filter of the device was performed by a gas chromatographic method after extraction. The collected saliva impregnated swabs were placed and sealed into plastic containers and frozen. After extraction of the saliva from the swab by centrifugation, cotinine was measured by radioimmunoassay. All the analysis was performed in Winston-Salem Laboratory of RJ Reynolds and the detailed method and the crude data31 were described in the tobacco industry document analysis by Hong and Bero.6
Data analyses
Reliability was measured as the agreement between self reported smoking status in 1991 and 1992 using κ statistics. The Spearman correlation coefficient between the urinary CCR, the average salivary cotinine value, and the nicotine concentration measured for one week using passive smoke monitors worn by the subjects, and also placed in the living room, were calculated to examine the validity of the CCR. To examine the relation of self reported ETS exposure with these laboratory indices, analysis of variance was performed. Also, differences in the diet and lifestyle of families with and without smoking husbands were examined by analysis of variance to evaluate confounding bias in the relation between ETS exposure and lung cancer.
RESULTS
Characteristics of the subjects
The total number of subjects used for the analyses were 196 from Osaka and 200 from Shizuoka. Subjects excluded from the Osaka dataset included one subject whose husband was away at work, and another three who did not provide complete information on smoking status. Comparison of the subject characteristics between the two cities is shown in Lee’s report.12 For the following analysis, the subjects from the two cities were combined together. The average age of the subjects was 41 years old (range 22–55 years). Seventy eight wives (19.7%) self reported as current smokers, 32 (8.1%) as ex-smokers, and 286 (72.2%) as lifelong never-smokers. The average age of the never-smokers was significantly older than ever-smokers (42.8 years v 36.7 years; p < 0.001), and the proportion of husbands’ smoking was significantly lower for never-smoking wives than for ever-smoking wives (51.0% v 80.4%).
Reliability of the self reported smoking status
The reliability of the key information regarding smoking status and ETS exposure reported by the subjects in November 1991 and June 1992 is shown in tables 1 and 2. As the high κ coefficients indicate, the repeated interview showed good agreement suggesting the high reliability of the response.
Self reported current or previous smoking experience in 1991 and 1992
Self reported current smoking status or ETS exposure of non-smokers in 1991 and 1992
Validity of the self reported smoking status in comparison with nicotine monitoring
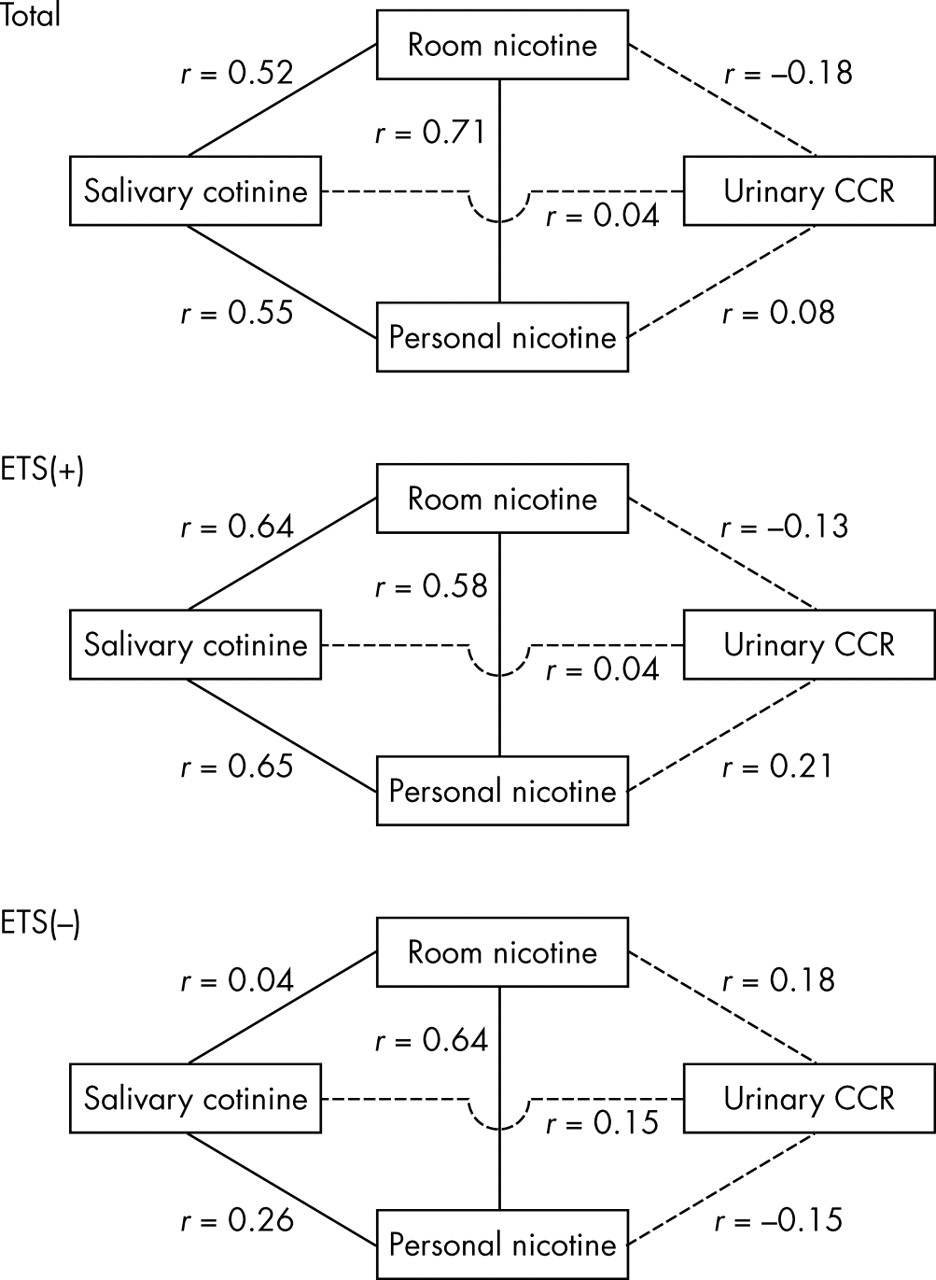
As can be seen in fig 1, the correlation of both room and personal nicotine concentrations, and salivary cotinine concentrations, was significant, especially among the subjects with ETS exposure. However, the urinary CCR correlated neither with the nicotine concentration nor the salivary cotinine, in any of the groups.

{kind=link}
The Spearman correlation coefficient between the urinary cotinine: creatinine ratio (CCR), the average of salivary cotinine concentration, and the nicotine concentration measured for one week using passive monitors worn by the subjects, and also placed in the living room measured in Osaka in 1992. Data were shown for the total subjects and for those with (ETS+) and without (ETS−) environmental tobacco smoke exposure.
Table 3 indicates that self reported ETS exposure correlated with both room nicotine concentration and personal nicotine exposure, while salivary cotinine did not. The average urinary CCR was slightly smaller in the subjects with ETS exposure than those without ETS exposure. Similar paradoxical relations between CCR and ETS exposure can be observed in the tables in Lee’s report.12 For example, in lifelong non-smoking wives, having a husband who currently smokes was related to a lower level of CCR compared with wives of non-smoking husbands. If a wife had a smoking husband, heavy smoking at home did not necessarily increase her CCR (appendix table 1). For non-smoking wives, working and having any exposure to ETS was also related to lower median CCR (appendix table 2) (to view tables 1 and 2 in the appendix please visit the Tobacco Control website—http://www.tobaccocontrol.com/supplemental).
Self reported environmental tobacco smoke (ETS) exposure and the laboratory indices (mean (SD))
Possible misclassification of active smoking status
Table 4 (table 2 in Lee’s report12) shows the distribution of CCR by self reported smoking status. Lee claimed that 28 of 318 (8.8%) self reported non-smokers were smokers misclassified by self report as non-smokers, which was much higher than the figures of between 1.9% and 3.4% obtained in the 10 country study by Riboli et al.32 However, Lee did not mention the 8 of 78 (10.3%) self reported smokers misclassified by CCR as non-smokers, which was also very high compared to western studies.33 Such events can occur by random reporting error of smoking status or because of CCR measurement error.
Cotinine: creatinine ratio (CCR) by self reported smoking status (equivalent to Lee’s table 2)
Confounding
Comparing non-smoking women with and without ETS exposure, only one of 30 lifestyle items and two of 24 diet items revealed significant differences (appendix table 3) (to view table 3 in the appendix please visit the Tobacco Control website—http://www.tobaccocontrol.com/supplemental). After excluding women with CCR > 100 ng/mg, “taking breakfast/lunch with husband” and frequency of juice drinking were significantly related to smoking status. However, considering the number of repetitions of the comparison, the significant relations could have arisen merely by chance.
DISCUSSION
The present study demonstrated a high reliability of self reported smoking status. Also, the measurement of nicotine concentration suggests high validity of self reported ETS exposure and invites a question about the validity of the CCR in this study. The CCR data were misrepresented in Lee’s report.
Lee has claimed that a higher proportion of misclassified current smoking Japanese women were included in the non-smoking group, when self reporting was used for the definition of smoking status and CCR was used as the gold standard. In general, cotinine is regarded as the objective index of smoking status,34,35 and CCR in excess of 100 ng/mg (sometimes 50 ng/mg) is used as a cut-off value to distinguish active from passive smokers.32 However, on close examination of the data from self reported smokers in table 4 (Lee’s table 2), we see that a similar percentage of CCR determined non-smokers were misclassified as current smokers by self report, which was also in contrast to western studies. Lee speculated that cultural attitudes and constraints against women smoking may be higher in Japan when compared to western countries. However, if this were the case it would be incomprehensible for non-smoking women to claim to be current smokers. This thus raises doubts concerning the value of the CCR as an objective and valid measure of smoking status.
Furthermore, there were also several inverse relations of ETS exposure or smoking status and CCR in almost half of tables 3 and 5 of Lee’s report (reproduced as appendix table 1 and 2). Although the differences may be small and could be due to chance, this raises further doubt about the credibility of the CCR in this study.
In addition to the misrepresentation of the facts demonstrated in his own paper, Lee did not report some of the important findings obtained in the project, which was the validity of the self reported ETS exposure status confirmed by the two nicotine indices of personal exposure and ambient concentration, and very low correlation of CCR with the nicotine indices. Salivary cotinine correlated with the nicotine indices when ETS exposure was present, but there was a slight negative correlation between room concentration of nicotine and urinary CCR. Since current smokers were not included in the validation study, only the non-smoking women with and without ETS exposure can be compared, but this again showed low validity of CCR in this study.
Another fact not mentioned in Lee’s report was the results of the confounding study, which was one of the two main purposes of the project. Despite the very elaborate questionnaire, no apparent difference in diet or lifestyle was observed when non-smoking wives with and without ETS exposure were compared. Hence, the original hypothesis that families with smoking husbands have different diets or lifestyles compared to those with non-smoking husbands was not supported. Therefore the association between ETS exposure and the higher incidence of lung cancer in the wives of smokers cannot be explained by confounding bias.
Together, these findings suggest that the CCRs used in this study were not necessarily valid. The misclassification could therefore possibly be due to the unreliable CCR rather than to self reporting smoking status. One study has indicated the exaggeration of ETS exposure by CCR due to smoking associated change of urine flow,36 whereas in general, urinary cotinine has been regarded a valid measure to detect ETS exposure.37,38 Since the measurement of CCR was done without knowledge of the smoking status of each subject, there was no opportunity for measurement bias; however, for whatever reason the CCR measurement was not valid in detecting ETS, it could lead to mere random misclassification of smoking status for both smokers and non-smokers. If this occurred, the resulting random misclassification could be a source of bias. The data in table 4 (Lee’s table 2) are compatible with this assumption. The data were not biased, although Lee’s commentary on the data was biased.
Contrary to Lee’s assertion, a valid interpretation of Lee’s table 2 strengthens Hirayama’s findings. Random misclassification generally inclines the effect measure (odds ratio) toward the null.39 If the same random misclassification affected the original Hirayama’s spouse study, the results he obtained would be biased towards the null and the magnitude of the effect of ETS exposure in causing lung cancer may have been underestimated in his study. If the misclassification were to be corrected in Hirayama’s study, the true odds ratio could be larger than he reported, showing an even stronger association between ETS exposure and lung cancer.
Since the original study was performed, there have been several studies and reviews40–44 which examined the misclassification of smoking status by self report, including a Japanese study.41 Most of these40–43 indicated that even if there is misclassification of smoking status through self report, it is small and unlikely to explain the increased health risks observed in epidemiological studies on ETS. Also the possible confounding by lifestyle differences between non-smoking women, with and without a spouse who smoke, has been investigated by many researchers. Hackshaw quantitatively evaluated the effect of such possible confounding in eight other studies, concluding it to be negligible.45
What this paper adds
Association of exposure to environmental tobacco smoke (ETS) and lung cancer was first reported by a large cohort study in Japan. However, the study was challenged by Lee who claimed that in comparison to western countries, a higher proportion of current smoking Japanese women were misclassified as non-smokers as indicated by the urinary cotinine/creatinine ratio (CCR), thus creating an overestimation of the risk of ETS to cause lung cancer.
Some of the data on which Lee based his report were at variance with his conclusions, and suggest the dubious validity of CCR as an index of smoking status. The data obtained, but not reported by Lee, showed high correlation of self reported exposure status to ETS with nicotine exposure and salivary cotinine concentrations, but not with the CCR. This finding has raised questions as to the value of the CCR as the gold standard in the verification of self reported smoking status, and therefore the credibility of Lee’s conclusion.
In addition to the misrepresentation and misappropriation of results by a researcher with an extensive history of association with the tobacco industry, there have been attempts to intimidate and suppress scientific findings by anti-tobacco lobby campaigners in Japan.46,47 Induced by misleading translations47 of the article by Hong and Bero,6 they have rejected any informed discussion concerning the Hirayama study. I have been accused of questioning the validity of the Hirayama study, which they regarded as sacrosanct and not to be re-examined.46,47 Demands have been made that my medical school should censor my research and publications in this regard.49,50 My offers of an inquiry and an open forum to examine the matter have been refused51 and condemn other’s explanation as metaphysics without discussion.52 My personal and scientific concern for the unauthorised publication and misuse of data by Lee has prompted the revisiting of this issue. Likewise, I consider it imperative for the integrity of scientific research that any distortion of scientific findings, by either pro- or anti-smoking campaigners, is counteracted.
REFERENCES
Supplementary materials
The table is available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Appendix table 1. CCR by husband�s smoking (Reproduced from selected lines of Lee�s table 3)
Footnotes
-
Competing interests: none declared