Article Text

Abstract
Context: The global tobacco epidemic may kill 10 million people annually in the next 20–30 years, with 70% of these deaths occurring in developing countries. Current research, treatment, and policy efforts focus on cigarettes, while many people in developing regions (Asia, Indian subcontinent, Eastern Mediterranean) smoke tobacco using waterpipes. Waterpipes are increasing in popularity, and more must be learned about them so that we can understand their effects on public health, curtail their spread, and help their users quit.
Objective: To conduct a comprehensive review regarding global waterpipe use, in order to identify current knowledge, guide scientific research, and promote public policy.
Data sources: A Medline search using as keywords “waterpipe”, “narghile”, “arghile”, “shisha”, “hookah”, “goza”, “hubble bubble” and variant spellings (for example, “hooka”; “hukka”) was conducted. Resources compiled recently by members of GLOBALink were used.
Study selection: Every identified published study related to waterpipe use was included.
Data synthesis: Research regarding waterpipe epidemiology and health effects is limited; no published studies address treatment efforts. Waterpipe use is increasing globally, particularly in the Eastern Mediterranean Region, where perceptions regarding health effects and traditional values may facilitate use among women and children. Waterpipe smoke contains harmful constituents and there is preliminary evidence linking waterpipe smoking to a variety of life threatening conditions, including pulmonary disease, coronary heart disease, and pregnancy related complications.
Conclusions: More scientific documentation and careful analysis is required before the spread of waterpipe use and its health effects can be understood, and empirically guided treatment and public policy strategies can be implemented.
- epidemiology
- policy
- waterpipe
Statistics from Altmetric.com
Globally, 4.9 million deaths each year are attributed to tobacco use, and this annual toll may increase to 10 million within the next 20–30 years.1 Of these deaths, 70% are likely to occur in developing countries,1 making tobacco use a global epidemic.1,2 Unfortunately, despite the fact that developing countries bear the brunt of this epidemic, most research and treatment efforts address developed nations. Moreover, research tends to focus on tobacco use methods that are prevalent in developed countries (that is, cigarettes, smokeless tobacco) and often does not consider methods common in developing countries, such as the waterpipe. This emphasis was apparent during the recent 12th World Conference on Tobacco or Health (Helsinki, February 2003), where delegates noted the dearth of waterpipe research, despite the fact that as many as 100 million people use waterpipes daily.3
This review’s purpose is to describe the waterpipe as a tobacco use method that may be re-emerging as a virulent strain in the tobacco epidemic. The review focuses on research related to waterpipe epidemiology, health effects, and public policy. Past experience teaches that ignoring these aspects of tobacco use products can lead to a “public health disaster” that may have been preventable.4,5
METHODS
Waterpipe: terminology, description, and current popularity
Waterpipe terminology can depend upon region, and includes names such as “shisha”, “boory”, or “goza” (Egypt, Saudi Arabia;6–8), “narghile”, “nargile”, or “arghile” (Israel, Jordan, Lebanon, Syria9–11), “hookah” (Africa and Indian subcontinent;12,13), and “hubble bubble” (many regions—for example, see Shafagoj and Mohammed14). Besides terminology, there is also regional variation in shape, size, appearance, and tobacco smoked.3,7 Here, the term “waterpipe” is used to refer to tobacco use methods in which smoke passes through water.
Generally, waterpipes consist of head, body, water bowl, and hose (fig 1). The most common type of tobacco used in the waterpipe is called Maassel,10,11 which is sweetened and flavoured (for example, apple, mint, cappuccino). Other forms of tobacco may contain less sweeteners/flavours and are called Ajami, Tumbâk or Jurâk.6,11,15

Primary waterpipe components. Tobacco is placed in the head and often covered with perforated aluminium foil; burning charcoal is placed on top of the foil. Water half fills the bowl, submerging a tube through which smoke enters, but not the hose-connected tube through which smoke leaves. Thus, an inhalation at one end of the hose produces a vacuum in the air filled space of the water bowl, causing smoke to pass through the water (producing bubbles and the onomatopoetic moniker “hubble bubble”), into the hose-connected tube, and to the smoker. Disposable plastic mouthpieces can be added, to limit the spread of disease. The size of the waterpipe, number of hoses, and other features can differ widely.
Waterpipe use is centuries old, and its origins are obscure.3 It is used to smoke tobacco in regions of China,16,17 India,18–20 and Pakistan,12,21 and is often associated with the Eastern Mediterranean Region (EMR7,8,10,11,14,22). However, as recently as 1980, its popularity had been declining.14,23 Unfortunately, today in the EMR, boys and girls are using waterpipes, which they view as fashionable.9,10,24 Indeed, waterpipes are now commonplace in Arab societies, and many restaurants and cafés in the EMR serve them.3,25–28
Global health organisations are ill equipped to face this potential health hazard, because little is known about patterns of waterpipe use and health effects. Gaining this knowledge may be challenging: instruments specific to waterpipe do not exist, and many of the tools used for cigarette smoking may not apply to this method.10 A comprehensive and critical literature review regarding waterpipe use thus serves two purposes: it identifies the current knowledge base while highlighting future growth areas that can guide method development, scientific research, and public policy.
Search strategy and selection criteria
To identify published work, we searched Medline using these keywords: “waterpipe”, “narghile”, “arghile”, “shisha”, “hookah”, “goza”, “hubble bubble”. We also used variant spellings (for example, “hooka”, “hukkah”, “hukka”). In addition, we used resources compiled with the assistance of GLOBALink, the Society for Research on Nicotine and Tobacco, and the US Centers for Disease Control and Prevention. A recent review that focused on Egyptian waterpipe research7 was of particular value for its summaries of studies reported in Egyptian journals that are not indexed in Medline and that are otherwise not readily available.
RESULTS
Results yielded a total of 64 published papers, “in press” manuscripts, or abstracts. The regional distribution of this research highlights the global nature of waterpipe use: the majority of work is from the middle east (Egypt 24, Israel 2, Jordan 2, Kuwait 1, Lebanon 10, Saudi Arabia 3, Syria 5, Tunisia 1, Turkey 2, Yemen 1), though contributions also come from Asia (China 1, India 5, and Pakistan 3), Europe (Austria 1, France 1), Australia (1), and North America (USA 1). This work is discussed below, in terms of waterpipe epidemiology, health effects, and public policy.
Epidemiology
Epidemiological research methods are a valuable tool in understanding current trends in the global tobacco use epidemic. For a developing issue, such as waterpipe use, they can help establish incidence and prevalence rates, identify changes in prevalence over time, and reveal how beliefs and attitudes influence waterpipe use patterns. Few published studies address these topics with respect to waterpipe use.
Incidence and prevalence of waterpipe use
Although data on the spread of waterpipe use are scarce for the EMR, available information paints a worrisome picture. A national survey in Kuwait shows that 57% of men and 69% of women had used waterpipe at least once.29 Waterpipe use is also common in Egypt, where 22% of 6762 men from two rural villages reported current or past use.30 In this study and others,25 most users reported starting waterpipe use after their 19th birthday. However, recent data from the EMR show that substantial numbers of adolescents and young adults are now smoking waterpipes. In Syria, for example, about half of university students report having ever used a waterpipe, and about a quarter of males currently use it.10 The picture is similar in Lebanon, where, of 1964 Beirut university students, 30.6% of men and 23.4% of women reported current, weekly waterpipe use in 2001.24 Rates of waterpipe use are high among high school age students. Across several EMR countries, about 10–18% of 13–15 year olds use tobacco products other than cigarettes, most likely waterpipe.31,32 In a sample of 635 Egyptian children (mean age 15.5 years; 211 girls), 19% reported ever using waterpipe, with a clear influence of sex: 26% of boys and 5% of girls reported waterpipe use.33 In Israel, 22% of children 12–18 years of age reported using waterpipe at least every weekend.9 In this sample of 388, waterpipe use was three times more likely than cigarette smoking, and as common for boys as for girls. Additionally, a study of Arab American adolescents found that 26.6% of those sampled use waterpipe, emphasising the global nature of this method, at least among Arabs.34
Changes in prevalence of waterpipe use over time
Understanding changes in waterpipe use over time is challenging, because surveys conducted before 1990 rarely addressed this tobacco use method. To our knowledge, this issue has been examined empirically in only one population: Lebanese university students. A survey of students from several Beirut universities in 2001 reported 21.1% current waterpipe use,24 while a survey conducted in 2002 at the American University of Beirut reported 28.3% current users.35 A similar increase was observed for individuals reporting that they had ever used waterpipe: 43% of entering students reported ever use in 2002,35 compared to 30% four years previous.36 Thus, among this population, the prevalence of waterpipe use may be increasing quickly.
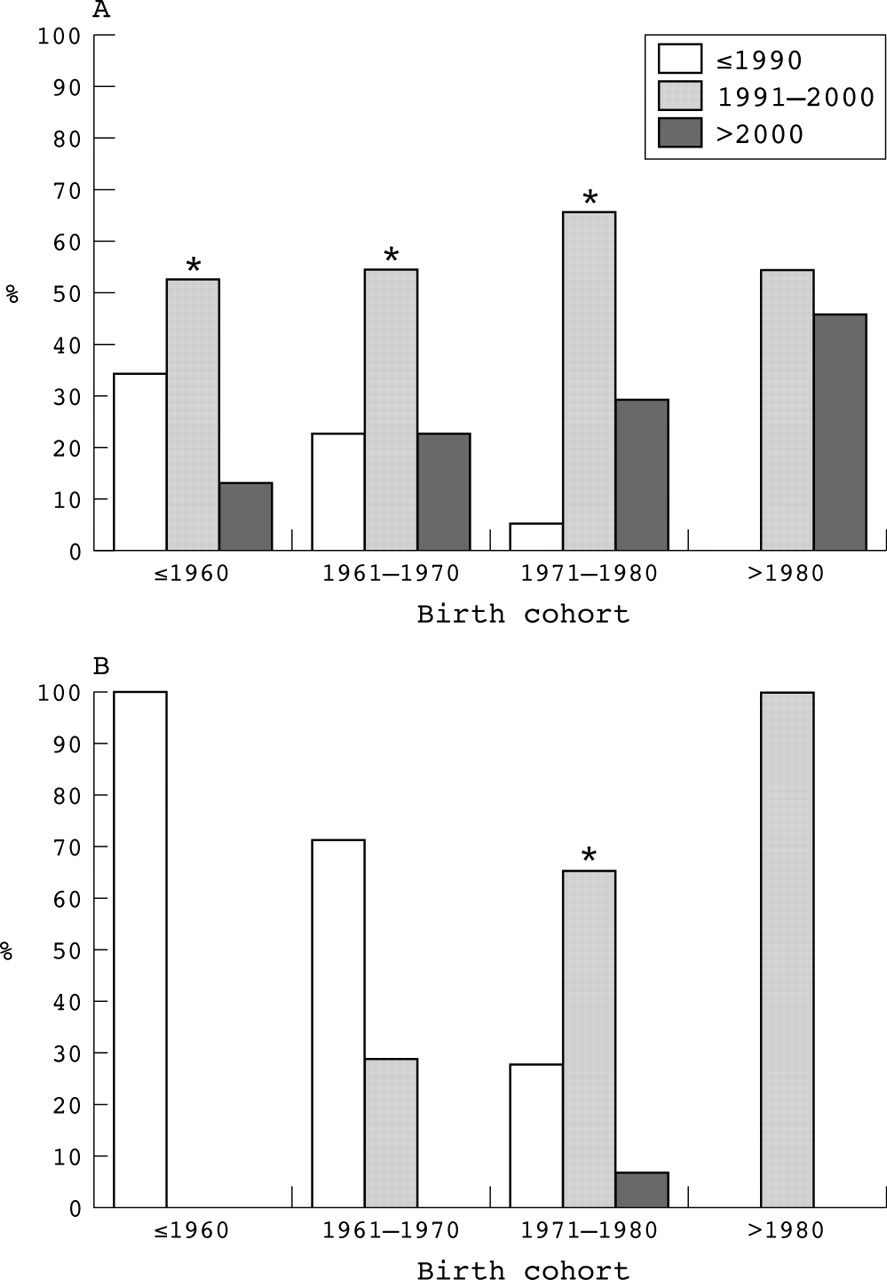
Another approach to measuring changes over time is to compare the time period of initiation of waterpipe use and cigarette smoking across several birth cohorts. As fig 2 shows, there is a clear age related pattern for cigarette smoking initiation in Aleppo, Syria, with older smokers initiating cigarette use in earlier decades. In contrast, across all age groups, most waterpipe initiation occurred during the 1990s, implicating this decade as the beginning of today’s waterpipe epidemic, at least in this Syrian city. Interestingly, Maassel was introduced in the 1990s, and this sweetened and flavoured tobacco may play a significant role in waterpipe initiation. In addition to flavour, Maassel simplifies the process of waterpipe preparation: there is no need to moisten, shape, and dry the tobacco before use, as with other tobacco forms, such as Ajami. Ajami was once the main tobacco used in waterpipes in Syria, but now accounts for less than 3% of waterpipe tobacco used by students.10 Thus, like flavoured and pre-packaged smokeless tobacco products in the USA that are recruiting new smokeless tobacco users,37 flavoured and convenient Maassel in the EMR appears to be recruiting new waterpipe users. Clearly this tobacco form is popular: revenues from Maassel sales in Bahrain reached $12 million in 1996 with a 36% increase in demand over previous years.26 In a survey of 300 Egyptian waterpipe café patrons,7 74% used Maassel.

Period of initiation of waterpipe use (A) and cigarette smoking (B) for different birth cohorts in Aleppo, Syria. These unpublished data come from a cross sectional survey done in 2003 among a random sample of café customers in Aleppo (n = 268; 61.1% men; mean (SD) age 30.1 (10.2); age range 18–68 years; response rate 95.3%). Participants were asked about their waterpipe use frequency, cigarette smoking status, current age, age of initiation of waterpipe smoking, and age of initiation of daily cigarette smoking. Asterisk indicates a significant difference between initiation time periods for each birth cohort (p < 0.05).
Attitudes and beliefs regarding waterpipe use
Attitudes and beliefs about tobacco use may shape behaviour.24,38,39 To date, very few studies have investigated attitudes and beliefs toward waterpipe use, although national and international studies of beliefs and attitudes regarding cigarette smoking abound.39–42 Perceived health effects may be of particular interest, as the experience in developed countries like the USA and Canada has been that tobacco products that are identified as “less risky” dominate the market.4 Anecdotal reports suggest that waterpipe use is perceived to have fewer health risks than cigarette smoking,43 and these reports may help to drive its current popularity. Regrettably, few empirical surveys have addressed this issue. In one, 90% of Israeli schoolchildren endorsed the notion that waterpipe use is not healthy, though 50% agreed that it was less harmful than cigarettes.9 Among university students in Syria,44 30% of those sampled thought waterpipes were less harmful than cigarettes, while, in Egypt, 21% of 206 adult male waterpipe users reported that they preferred waterpipe use over cigarette smoking because it was less harmful.25 However, 81–92% of these Egyptian users reported that they knew that waterpipe use was associated with lung cancer, asthma, heart disease, and infection transmission.25 These results highlight the uncertainty regarding the relation between perceived health effects and waterpipe use.
In some societies, gender may play an important role in maintaining low rates of women’s cigarette smoking, but may not have the same magnitude of effect on waterpipe use.24,45 One recent study in Syria examined perceptions for waterpipe use and cigarette smoking by sex of the respondent and sex of the user/smoker.27 Waterpipe use was generally more positively perceived than cigarette smoking, especially for women. Waterpipe users, especially women, were particularly enthusiastic about waterpipe’s positive aspects, including that it looks traditional, familiar, social, and attractive. Overall, waterpipe smoking may be becoming a behavioural norm in the EMR, especially for women24,27,46 and girls.9 This notion is supported by data from 13–15 year olds in the EMR: on average, the ratio of boys to girls reporting past 30 day cigarette smoking was 4.3:1.0, while the same ratio for past 30 day use of other tobacco products (most likely waterpipe) was 1.9:1.0.1
Health effects
Some of the health effects of waterpipe smoking may be predictable based on the components of waterpipe smoke. In addition, some research has examined directly the short and long term health effects to the user, as well as the impact of waterpipe use on a developing fetus and on non-smokers.
Components of smoke
Tobacco cigarette smokers are exposed to hundreds of potentially dangerous smoke constituents, including carbon monoxide (CO),47 carcinogens like tobacco specific nitrosamines,48 and the dependence producing drug, nicotine.49 This exposure leads to a variety of adverse health effects, including cancer, cardiovascular disease, and addiction.49 Waterpipe users may also be exposed to these smoke constituents, though little research addresses this issue.
The amount of CO in waterpipe smoke may depend upon waterpipe size, variety of tobacco, and charcoal type: relative to a cigarette (0.41% CO by volume) some combinations produced smoke with substantially greater CO levels (small waterpipe 1.36–1.40%) though others produced smoke with similar CO levels (large waterpipe 0.38–0.41%).50 Overall, the data support the contention that, at best, the CO yield of waterpipe smoke is similar to that of cigarettes.50 With regard to other constituents, waterpipe smoke produced by a machine contains significant amounts of dangerous constituents, including nicotine and heavy metals such as arsenic, cobalt, chromium, and lead.11,51,52 Under normal waterpipe use conditions, the smoke produced from a single waterpipe use contains approximately the same amount of nicotine-free, dry particulate matter (“tar”) as 20 cigarettes.11 However, the tar produced by a waterpipe may differ from that produced by a cigarette,53 because tobacco in a waterpipe is heated to about half the temperature (that is, 450°C) of tobacco in a cigarette. Temperature may be positively related to tar related tumorigenicity and mutagenicity.11,54 Of course, studies involving machine produced smoke may not predict constituent delivery to the smoker,4 thus research examining actual exposure to these constituents is an essential complement to this work.
Short term health effects
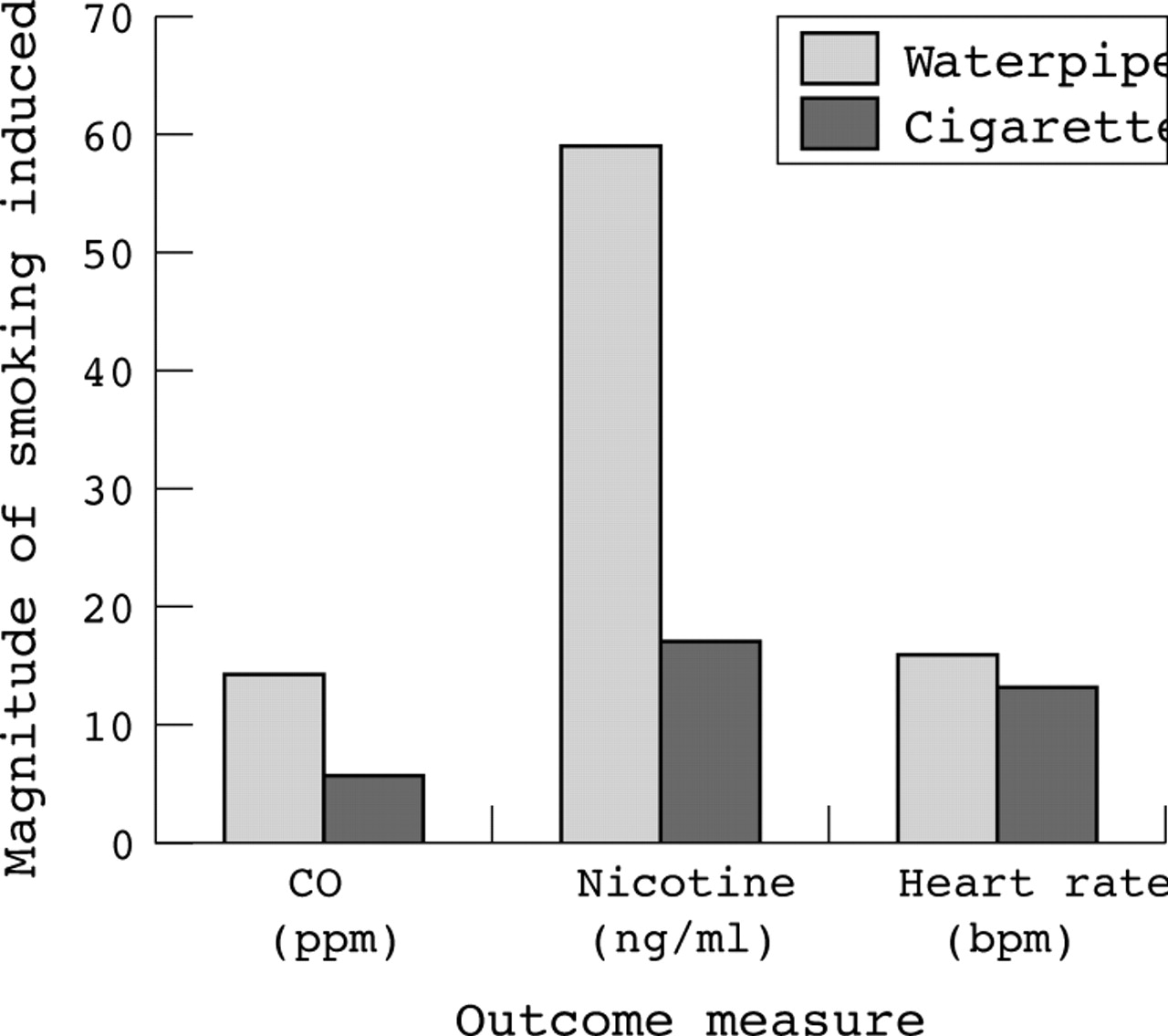
Smoke constituent delivery can be determined by examining smokers under controlled conditions, where CO and nicotine delivery, as well as cardiovascular and other effects can be assessed.55 Initial work reveals that, after 45 minutes of waterpipe use, expired air CO, plasma nicotine, and heart rate are significantly elevated.14,56 Cross study comparisons suggest that, relative to a single cigarette, 45 minutes of waterpipe use approximately doubles CO and triples nicotine exposure, with near equivalent effects on cardiovascular response (fig 3; acute tolerance may mediate cardiovascular effects over 45 minutes of use57). Of course, caution must be used when comparing the effects of waterpipes and cigarettes, because the average exposure time for a single waterpipe use (∼50 minutes11) differs from that for a single cigarette (∼5 minutes58). Nonetheless, with respect to CO, this cross study comparison is consistent with results of a field study in which blood samples from cigarette smokers (n = 601) and waterpipe users (n = 975) were analysed for carboxyhaemoglobin (COHb): relative to smokers’ average (SD) COHb concentration (6.47 (2.73)%), waterpipe users’ were significantly higher (10.06 (2.50)%; p < 0.001).6,59 As might be expected, the number of waterpipe uses/day was highly correlated (r = 0.84, p < 0.001) with COHb.6 Similar fieldwork suggests that waterpipe users are also exposed to some heavy metals (for example, cadmium).18 Clearly waterpipe users’ exposure to toxic smoke constituents has not yet been determined definitively, and may require an assessment of the effects of varying sized waterpipes, tobacco types, and smoking parameters, as well as within subject comparison with cigarettes. Current data14,53,56,60 do not support the notion that waterpipe use is benign with respect to CO and nicotine exposure, and/or cardiovascular effects.
{kind=link}
{kind=link}
{kind=link}
Effects of waterpipe use (light bars) and cigarette smoking (dark bars) on expired air carbon monoxide (CO, parts/million), plasma nicotine (ng/ml), and heart rate (beats/minute). For waterpipe, data are from 18 (CO and heart rate14) or 14 (plasma nicotine56) men from Jordan who were frequent waterpipe users and who abstained from smoking before their participation in a study in which they used a waterpipe ad libitum over a 45 minute period. Difference scores for CO, heart rate, and nicotine were calculated from data before and after the 45 minute smoking period. For cigarette, data are from 20 men (n = 10) and women from the USA who were daily cigarette smokers and who abstained from smoking before their participation in a study in which they completed four, 8-puff smoking bouts from one of their own brand of cigarettes over a 2.5 hour period (that is, one 8-puff bout every 30 minutes55). Difference scores for CO were calculated from data before and after the first bout, and for heart rate were calculated before and during the first bout. For nicotine, difference scores were calculated based on blood drawn before the session began and after it ended (that is, after the final puff of the fourth smoking bout).
Nicotine dependence may also result from repeated inhalation of tobacco smoke from a waterpipe. Nicotine dependence is common among cigarette smokers,49 and likely underlies their continued tobacco use despite health risks, financial costs, and repeated attempts to quit. Relative to cigarette smokers, waterpipe users may receive equal or higher doses of this psychomotor stimulant (fig 3),56,61 thus they, too, are at risk for physical dependence. In cigarette smokers, nicotine’s dependence producing effects interact with learned behavioural and social components to exacerbate nicotine withdrawal and make quitting smoking very difficult.49 Until recently, no studies have characterised a waterpipe withdrawal syndrome, though some of the hallmarks of dependence are apparent: continued use despite potential health risks, financial cost, and reported inability/difficulty quitting.62 Preliminary results suggest that one marker of waterpipe dependence may be the transition from smoking as primarily a social phenomenon (that is, while relaxing with family or friends, often in restaurants or cafes) to a more solitary experience (that is, alone, at home).62
Aside from the direct effect of smoke constituents, the social dimension associated with waterpipe use may help spread infectious agents because, in many cultures, sharing a waterpipe is a common custom. For example, in Aleppo, Syria, the majority of waterpipe smokers among university students share the same waterpipe with their friends,10 in Beirut, Lebanon, 89.8% share the waterpipe,35 while, in Israel, 100% of children who use waterpipe reported that they pass the mouthpiece from mouth-to-mouth.9 In India, not offering to share a waterpipe with a guest is an insult.63 This practice can spread tuberculosis53,64 and viruses (herpes, hepatitis), particularly given that the temperature of smoke coming out of the waterpipe mouthpiece is likely similar to that of the ambient air.11 A report of a cluster of tuberculosis cases associated with waterpipe sharing demonstrates the risk,53,65 and the recent development and current use of disposable mouthpieces may help to reduce it.
Long term health effects
There is preliminary evidence linking waterpipe use to disease, though this research is made difficult by the fact that many waterpipe users also smoke cigarettes24,27,66 and/or engage in other behaviours that may increase cancer risk.67 Waterpipe use likely increases the risk of bronchogenic carcinoma,68 as well as lung,16,20,69 oral,8 and bladder21,70 cancers. The notion that waterpipe use is associated with cancer is not surprising, given that, like cigarette tobacco, the tobacco used in waterpipes contains tobacco specific nitrosamines,71 and that waterpipe extract produces degeneration and hyperkeratosis in rat mucosa.72 Moreover, in a study comparing 35 healthy waterpipe users with 35 healthy, non-exposed controls, waterpipe use was associated with a significant increase in frequency of chromosomal aberrations and sister chromatid exchanges.63 While the sample size was low, there were obvious trends toward a dose dependent relation on these outcome measures when the data were analysed based upon years of smoking and amount of tobacco smoked each day.63 Also, the frequency of satellite associations and the mitotic index was significantly higher in waterpipe users, relative to controls.63
Waterpipe use is associated with markers of atherosclerosis73 and with coronary heart disease,74 and several studies have examined its pulmonary effects.19,53,64,75–79 In one, elevated levels of free radicals were found in peripheral blood neutrophils of waterpipe smokers.19 These free radicals are known to mediate lung tissue injury.80 In addition, two studies assessed pulmonary function of waterpipe smokers compared to cigarette and non-smokers. Although the magnitude of effect of waterpipe use on lung function differed in the two studies, they both demonstrated worse mean forced vital capacity and forced expiratory volume in one second of waterpipe users compared to non-users.74,75 Additionally, airflow at 25–75% vital capacity was lower in waterpipe users relative to cigarette smokers,78 and peak flow rate was less than 200 l/min in 37% of waterpipe users, but only 3.8% of smokers,53 perhaps due to waterpipe induced changes in lung biochemistry, as indexed by differences in bronchoalveolar lavage fluids.52,81,82 Also, in a laboratory study of seven waterpipe using men, daily use was associated with increased plasma concentration of 8-epi-PGF2a, a marker for in vivo oxidation injury that is also elevated in cigarette smokers.3
As well as risking cancer, decreased pulmonary function, and cardiovascular disease, waterpipe users may also be vulnerable to other ailments. Separate case study reports suggest that waterpipe use can lead to eczema of the hand83 and to aspergillosis when immunocompromised patients use contaminated tobacco84; higher rates of tuberculosis in waterpipe users relative to smokers have been reported.53 Also, relative to non-smokers, tobacco users are at increased risk for “dry socket” following tooth extraction (postextraction alveolitis) and this risk may be heightened further for waterpipe users.85 Overall, the extant data are consistent with a link between waterpipe use and addiction, disease, and death.86 Nonetheless, these preliminary studies generally involved small samples and other limitations, and more work is required to establish these links definitively.
Impact of fetal exposure
CO exposure during pregnancy can harm the fetus, and is thought to underlie the low birthweight and low Apgar scores observed in neonates born to smoking mothers (that is, fetal tobacco syndrome).87 Clearly, fetal tobacco syndrome is a risk for babies born to women who use waterpipes during their pregnancy—these women face increased risk of having babies with low birth weight, low Apgar scores, and respiratory distress.88 In Beirut and its suburbs, a quarter of the 576 pregnant women who were sampled reported that they smoked waterpipe during their pregnancies.46
Impact of environmental tobacco smoke exposure on non-waterpipe users
Children are vulnerable to the harmful effects of cigarette related environmental tobacco smoke (ETS).89 Because children spend a majority of their time in the home, they may also be at risk for exposure to waterpipe ETS in homes where waterpipes are used. In a survey of waterpipe use patterns in Aleppo, Syria, 19% of waterpipe users reported primarily home use, and nearly half (48.4%) of heavy waterpipe users (those who smoked at least once per day) did so mainly in the home.62 Children’s exposure to ETS from waterpipe users is also high in Lebanon, where it has been linked to increased frequency of respiratory disease.90 Of course, the health effects of ETS exposure from waterpipe on children have not yet been evaluated comprehensively, but they are likely to include many of those that result from exposure to cigarette smoke, including increased risk of ear and upper respiratory infection, asthma, and sudden infant death syndrome.91 The higher content of heavy metals in waterpipe smoke compared to cigarettes11 may also have adverse health effects on exposed non-smokers. Because many waterpipe users also smoke cigarettes, the potential for an interactive effect of waterpipe and cigarette ETS on non-smokers must be considered.
PUBLIC POLICY ISSUES
Policy change signifies an important milestone in the control of public health threats, and tobacco control policies decrease cigarette smoking in many countries, including some in the EMR.92,93 Pro-health policy related to waterpipe use has lagged behind. Policy change (in the direction of tobacco prevention and control) is predicated on the presence of three key processes: documentation, analysis, and prescription.94 Documentation includes the gathering of statistical facts and the verification of statistical correlations, while analysis involves using documentation to gain an in-depth understanding of the behaviour in question. As demonstrated here, documentation of the increasing prevalence and health damaging effects of waterpipe use is progressing steadily, but more documentation and analytic research is needed. Nonetheless, given growing evidence of the harmful effects of waterpipe use, along with strong evidence of the adverse health consequences of other forms of tobacco such as cigarettes, cigars, and smokeless tobacco, waterpipe use should be considered dangerous unless proven otherwise. For many years the tobacco industry argued that evidence linking tobacco use to health damage was “inconsistent” and “incomplete”. This deceptive tactic too often delayed implementation of effective tobacco control policy. Policymakers should not fall into this same trap regarding waterpipes.
Careful documentation and thorough analysis lay the groundwork for prescription, resulting in a strategic model to implement pro-health policy changes.94 The prescriptive process may be the most important policymaking role that science plays, and is challenged if documentation or analysis are inadequate. For example, policymakers can complicate the process by eschewing documentation and analysis in favour of a preconceived notion of the “prescription”. In Egypt, some Islamic leaders have forbidden smoking on religious grounds, with the result that many current waterpipe users and cigarette smokers consider their behaviour sinful, though this idea has not altered behaviour appreciably.95,96 Some policy makers in Egypt,97 Iran,98 Oman,99 and Thailand100 have proposed bans on waterpipe usage, without consideration of the cultural implications of this action. Prescriptions may be most effective, and receive the greatest support, when they are based on careful documentation and thorough analysis.
Clearly, any waterpipe use policy must be based on sound scientific research. Data on use patterns, attitudes and perceptions, and health risks associated with waterpipe use and ETS exposure are especially crucial. Subsequently, interventions for the prevention and control of waterpipe use must be tested. With this knowledge and analysis, researchers can recommend a strategic model for change. This model will likely benefit from strategies that have reduced the adverse health effects of cigarettes: marketing restrictions, warning labels, minimisation of children’s access, and support of health education programmes and cessation efforts.101,102 Indeed, the relatively limited advertising and promotion of waterpipe tobacco observed currently suggests an immediate opportunity to address waterpipe use proactively, by preventing initiation of these marketing approaches.
CONCLUSIONS
This review makes clear that there is a lack of knowledge and policy concerning waterpipe use. We were unable to find a single publication addressing treatment methods to help waterpipe users quit. Because waterpipe use is a global issue and potential global health threat, the concerted efforts of different research, public health, policy, and political institutions will be necessary to fill the knowledge, policy, and treatment gaps. Thankfully, some infrastructure is being put in place, and research efforts have begun (for example, the Fogarty International Center-funded Syrian Center for Tobacco Studies and Egyptian Smoking Prevention Research Institute,103 as well as the Research for International Tobacco Control-funded Tobacco Prevention and Control Research Group at the American University of Beirut, Lebanon). These efforts will need to be complemented with global efforts to:
-
address similarities and differences among the different types of waterpipes and waterpipe tobacco
-
explore issues related to social, health, and dependence aspects of waterpipe use, with a focus on guiding interventions that prevent new users and help current users quit
What this paper adds
The global tobacco epidemic may kill 10 million people annually in the next 20–30 years, with 70% of these deaths occurring in developing countries. Current research, treatment, and policy efforts focus on cigarettes, while many people in developing regions (Asia, Indian subcontinent, Eastern Mediterranean) smoke tobacco using waterpipes. Waterpipes are increasing in popularity, and more must be learned about them so that we can understand their effects on public health, curtail their spread, and help their users quit.
This integrative review paper suggests that perceptions regarding health effects and traditional values may facilitate waterpipe use among women and children. Waterpipe smoke contains harmful constituents and there is preliminary evidence linking waterpipe smoking to a variety of life threatening conditions, including cancer, pulmonary disease, coronary heart disease, and pregnancy related complications. More scientific documentation and careful analysis is required before the spread of waterpipe use and its health effects can be understood, and the necessary empirically guided treatment and public policy strategies can be implemented.
-
implement policies and regulations that help curtail this form of tobacco use worldwide (for example, sale to minors, smoking restriction, taxation)
-
develop evidence based counter-advertising about the health and economic hazards of this form of smoking, especially for women and younger children.
There is a growing recognition, with a minimal research base, that tobacco smoking using a waterpipe is increasingly common and potentially lethal. Awareness of the health threat associated with waterpipe use may be early enough that a comprehensive and coordinated global research programme, implemented now, may help guide the policy and treatment efforts that prevent a new wave of tobacco associated addiction, disease, and death.
Acknowledgments
This work was supported by US Public Health Service grants R01 TW005962, R21 TW006545, R01 CA103827, and R01 DA011082 and a grant provided by Research for International Tobacco Control.
REFERENCES
Footnotes
-
↵* Also Institute of Epidemiology and Social Medicine, University of Muenster, Germany
-
↵† Also Department of Health and Sport Sciences, and Center for Community Health, University of Memphis, Memphis, Tennessee, USA
-
↵‡ Also Department of Psychology and Institute for Drug and Alcohol Studies, Virginia Commonwealth University, Richmond, Virginia, USA