Article Text

Abstract
Background and aims Adolescents represent the next generation and have the greatest amount to gain from the tobacco endgame. They will provide the future momentum to achieve the tobacco endgame, thus it is important that their views on interventions are monitored. We examined support among 14–15-year-old New Zealanders for tobacco endgame goals and measures, and trends in this support from 2009 to 2012.
Methods This study used data from an annual survey of over 25 000 Year 10 students (14–15 year olds) undertaken by Action on Smoking and Health New Zealand. We assessed support for five tobacco control goals and measures: living in a smoke-free country; having fewer tobacco retail outlets; not selling tobacco in 10 years’ time; implementing outdoor smoking bans; and raising the price of tobacco.
Results Support for living in a smoke-free country was 59%, while support for a ban on all tobacco sales in 10 years’ time was 57% in the most recent survey year. Most respondents supported each of the tobacco control measures and gave strongest support to having fewer places where tobacco could be sold (71% in 2012). Support for the other two tobacco control measures in the most recent year ranged from 59% to 64% and had increased over time, in most cases significantly. Support was strongest among non-smokers and declined as participants’ smoking frequency increased.
Conclusions Young people support New Zealand's smoke-free goal and interventions that could help achieve it; this evidence should galvanise policy action, which remains out of step with public opinion.
- End game
- Public opinion
- Public policy
- Prevention
- Environment
Statistics from Altmetric.com
Introduction
The New Zealand government has committed to the goal of making New Zealand smoke-free by 2025, defined as reducing smoking prevalence and tobacco availability to minimal levels.1 Measures already in place include pictorial health warnings, the removal of tobacco retail displays, purchase age restrictions and regular excise tax increases; plain packaging, removal of duty free tobacco sales and designating cars carrying children as smoke-free spaces are currently under consideration. However, while each of these measures has contributed to reductions in smoking prevalence, additional policies are required to change current smoking trajectories and achieve the endgame goal. In order to achieve this objective, researchers and advocates have suggested varied tobacco control measures.2 Studies have examined New Zealand adults’ support for these measures;3–7 however, few international or domestic studies have examined support for tobacco control measures among children and adolescents.
Because New Zealand's goal of becoming smoke-free by 2025 is a medium-term objective, it will have a significant impact on young people, whose opinions will influence policy as they reach voting age (18 years). If young people do not engage with, and actively support, the endgame goal, there is a risk it could lose momentum. Assessing young people's support for the 2025 goal and how it might be achieved is thus crucial to informing policy priorities and advocacy strategies.
Furthermore, as citizens of a society, children have a right for their opinions and attitudes to be heard. The United Nations Convention on the Rights of the Child (UNCROC) (which New Zealand ratified in 1993) makes this right explicit; article 12 states that children should ‘be provided the opportunity to be heard’.8 Shier has outlined the levels of participation required to align with article 12 of the convention.9 The five levels of participation range from ‘children are listened to’ at the low level through to ‘children share power and responsibility for decision making’. Shier states that level 3 (ie, ‘children's views are taken into account’) is the minimum level required for any country that has adopted the UNCROC. Our study represents a small step to achieving this participation and ensuring that children's views are taken into account in policymaking.
As well as being important from a human rights perspective, studying adolescents’ attitudes to tobacco endgames is also important conceptually, as attitudes are likely to align strongly with current behaviour and may predict adolescents’ future actions.10 Research examining specific attitudes to smoking and adolescents’ own smoking behaviour has found antismoking attitudes are negatively correlated with smoking frequency, and adolescent non-smokers consistently hold more negative views of smoking than their smoker counterparts.11 ,12
Similar findings emerge in evaluations of large-scale attitude inoculation programmes, such as the Truth campaign, which exposed the tobacco industry's duplicitous practices, thus stimulating the development of antismoking attitudes and reinforcing intentions not to smoke.13 Overall, studies examining adolescents’ attitudes to smoking suggest antismoking attitudes are strongly associated with increased intentions not to smoke.
This evidence has two important implications: first, encouraging positive attitudes towards the tobacco endgame goal is likely to reinforce non-smoking intentions, which in turn will support realisation of the 2025 goal. Second, attitudes towards the endgame are likely to be strongly associated with adolescents’ own smoking status.
Although New Zealand was the first country to announce an endgame goal, the relative recency of this announcement means few studies have examined young people's views on potential tobacco control measures or endgame strategies. While Smith et al14—who used data from the 2009 Action on Smoking and Health (ASH) Year 10 snapshot survey—found a majority of young people supported reducing access to tobacco products such as reducing the number of places selling tobacco and increasing tobacco prices, no studies have examined more recent trends.
The 2009 ASH Year 10 snapshot survey was the first to include questions assessing support for potential tobacco control policy measures such as banning smoking in outdoor places where young people go and reducing the number of outlets allowed to sell tobacco . We updated Smith et al's analysis by examining up-to-date data, exploring trends and examining data from questions included since 2009 that assess support for an additional tobacco control policy (raising the price of tobacco), a tobacco control endgame aspiration (wanting to live in a smoke-free country) and a scenario (a ban on all tobacco sales in 10 years’ time). The aims of this research were
to examine and describe 14–15-year-olds’ support for tobacco control goals and measures in New Zealand
to examine the trends in support for tobacco control goals and measures from 2009 to 2012.
Methods
We analysed data from an annual survey for the years 2009–2012 of Year 10 students (14–15 year olds) undertaken by ASH New Zealand and funded by the Ministry of Health. This long-running survey was first fielded in 1999, and all New Zealand schools teaching Year 10 students face-to-face (ie, not by correspondence) are invited to participate each year. Schools administer the survey to their Year 10 students during supervised class time and individual students may decline to participate. In order to maintain confidentiality, students do not provide any identifying information and teachers are instructed not to check the questionnaires returned to them.15 The Ministry of Health Multiregional Ethics Committee approved the survey in 2007 for the 2008–2012 surveys. Significant changes to the survey are notified to the ethics committee through a yearly progress report.
The ASH questionnaire incorporates and extends some key measures from the international Global Youth Tobacco Survey (GYTS) relating to smoking and cessation behaviour, susceptibility, and exposure to secondhand smoke, as well as assessing the smoking status of family and friends. Since 2009 it has included questions investigating attitudes towards a range of tobacco control issues. The statements examined in this study are part of the larger survey conducted by ASH. The overall survey is developed and administered by ASH and includes some modifications each year (we note some statements were not included in the survey every year).
Between 2009 and 2012, school-level participation rates have ranged between 44% and 58%. Over 25 500 students have responded to the survey in each year, with 48% of the target population (28 447) responding in 2012 (see online supplementary table S4).
The characteristics of the returned sample remained fairly stable over time (table 1), with one exception being the age profile for the 2011 and 2012 surveys. These two surveys were fielded earlier during the school year than previous surveys. As such, fewer students had turned 15 prior to completing the questionnaire. Overall, sample characteristics show a close correspondence to population figures for Year 10 students available from the New Zealand Ministry of Education16 with respect to sex, prioritised ethnicity17 and school-based socioeconomic status (SES). In most cases, the sample characteristics were within 3% of the population parameters, although there was some systematic over-response by New Zealand Europeans and under-response by the low SES group. All analyses in the study are weighted by ethnicity and SES. Weights are also used to standardise the age distribution in each year (65% 14 year olds and 35% 15 year olds), to adjust for differences in age due to variation in the timing of the survey fieldwork.
Characteristics of the ‘Year 10’ sample by year (percentages)
Between 2009 and 2012, students were asked to indicate their level of agreement with five statements relating to tobacco control goals and measures (table 2). The statements included in the survey varied from year to year, but the wording for the statements remained consistent except for the fewer outlets selling tobacco products statement. Responses to these statements were divided into ‘agree’, ‘disagree’ or ‘don't know’.
Five tobacco control statements from the ASH Year 10 survey
For the most recent survey results (either 2012 or 2011 depending on the statement), we used logistic regression analysis to calculate adjusted ORs for the association between agreement with each statement and age, gender, ethnicity, SES, parental smoking status, friend smoking status, sibling smoking status and participant smoking status. Changes in responses to the five statements for the total study population were compared across years.
A dichotomous indicator of smoking susceptibility was also created using questions from the GYTS and originally adapted from a measure developed by Pierce et al.18 This analysis was restricted to never smokers only. Respondents were defined as being not susceptible if they answered ‘definitely not’ to both of the following questions: “If one of your best friends offered you a cigarette, would you smoke it?” and “At any time during the next year do you think you will smoke a cigarette?” All other respondents were defined as being susceptible.
All analyses were performed using SAS V.9.3 software. Significance tests were two-sided, with p<0.05 considered statistically significant. In addition to weighting estimates by ethnicity, school SES indicator and age, all confidence limits were adjusted for clustering at the school level.
Results
There was majority support for each of the five statements. Among the 2012 participants, 59% agreed that they wanted to live in a country where no-one smokes. Seventy-one per cent agreed that fewer outlets should sell cigarettes and tobacco, and 57% agreed that cigarettes and tobacco should not be sold in New Zealand in 10 years’ time. Of the 2011 participants, 59% agreed that smoking should be banned in all outdoor places where young people go and 64% agreed that cigarettes and tobacco should be more expensive so that children and young people cannot afford to buy them.
The level of support for the statements varied with sociodemographic and smoking-related variables (table 3). Females were more likely to support all the statements. Māori and Pacific students were less likely to support the statements relative to NZ Europeans, with the exception of the outdoor smoking ban statement, which Pacific students were more likely to support relative to NZ European students. Asian students showed varied support across the statements, and overall, there were no clear patterns in support by SES.
Associations (adjusted ORs*) for agreement with the five statements in the 2012 and 2011 surveys
By contrast, odds of support for the statements were consistently lower if one or both parents smoked, if a friend or sibling smoked, or if the student was susceptible to smoking. As might be expected, odds of support rapidly diminished with increasing smoking frequency. For daily smokers (which included 5% of the total survey population), agreement with the statements in 2012 was 10% for a smoke-free country, 22% for fewer outlets, 13% for no tobacco sales in 10 years and in 2011 was 16% for an outdoor smoking ban and 13% for raising the price of tobacco. In general, support for the statements increased over the study period within each smoking status category, although not always with statistical significance (see online supplementary tables S5–10).
When considering correlations of agreement between the statements, Cramer's V measure of association found associations ranging from 0.38 to 0.57 (see online supplementary table S11), which can be considered moderate to high correlation. These correlations were for the 2011 survey; the only year that all five statements were asked.
Support for a smoke-free country
Between 2011 and 2012, there has been a statistically significant 8% increase in the proportion of students who agree with the statement, from 51% (±1.3%) in 2011 to 59% (±1.2%) in 2012.
In 2012, ‘don't know’ was the next most common response accounting for 25% (±0.7%) of responses (a decrease from 28%±0.9% in 2011). The proportion of students who disagreed with the statement fell from 22% (±1.0%) to 16% (±0.9%), while the proportion of daily smokers agreeing with the statement was 10% (±2.0%) in 2012.
Support for fewer outlets selling tobacco products
Since 2009, the percentage of students agreeing that there should be fewer outlets selling tobacco products has risen from 65% (±1.3%) to 71% (±1.2%) in 2012 (figure 1) (it should be noted that the statement changed between 2010 and 2011, see table 2). The percentage who responded with either disagree or don't know was similar throughout—in about the mid-teens each, with 2012 being the first year that the proportion of don't knows (17%±0.8%) was higher than that for disagreement (12%±0.7%). Indeed, for the latest year of data available, the proportion of don't knows was higher than that for disagreement for all of the statements except for the raising the price of tobacco products statement.

Frequency of responses to fewer outlets selling tobacco products statement 2009–2012, with 95% confidence bars.
In 2012, only 22% (±3.1%) of daily smokers agreed with the statement. However, this had increased from 18% (±2.5%) in 2009.
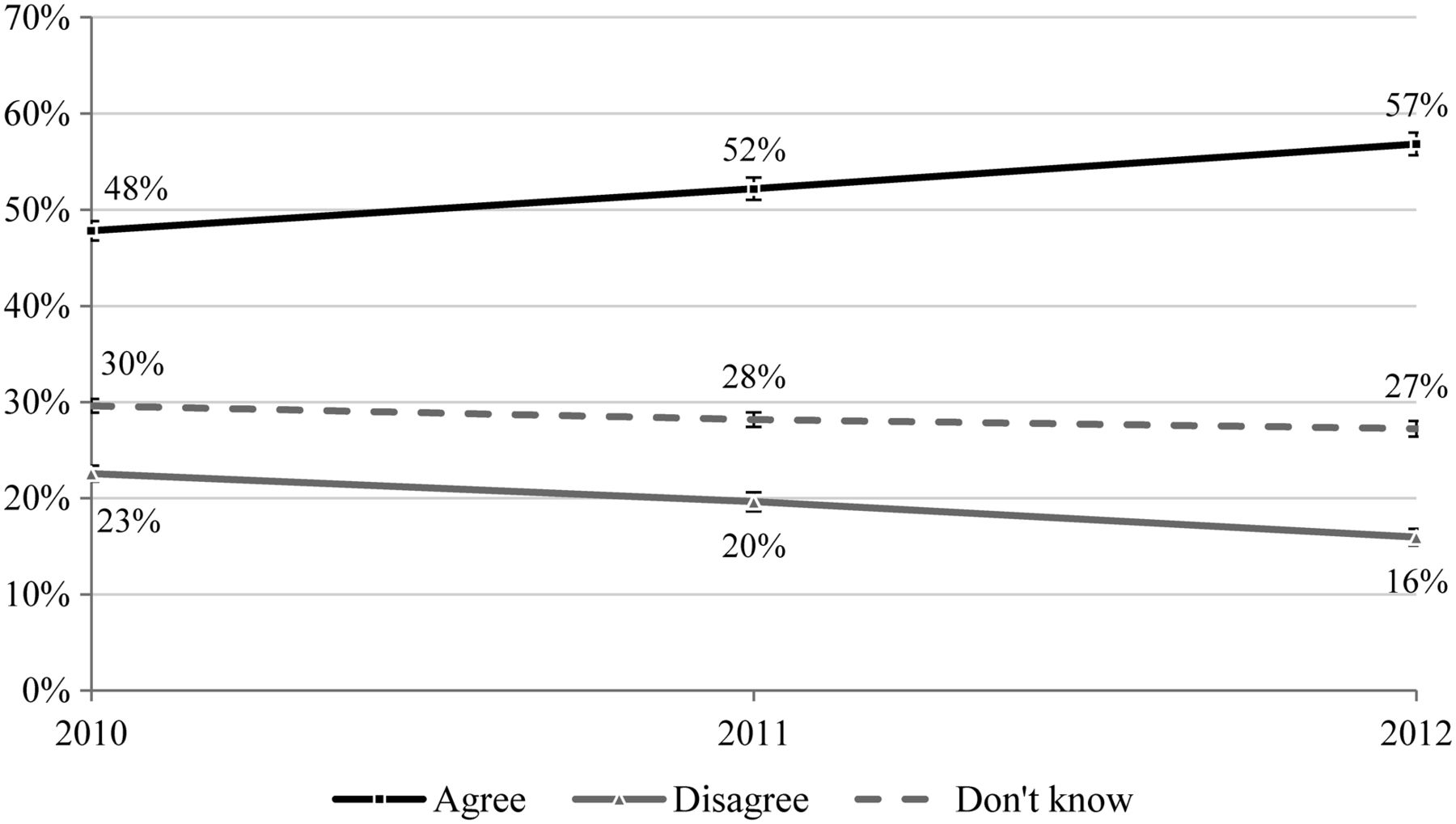
Support for no tobacco sales in 10 years
There has been a statistically significant increase in the percentage of students agreeing with this statement from 48% (±1.0%) to 57% (±1.2%) between 2010 and 2012 (figure 2). The proportion of daily smokers agreeing with this statement was 13% (±2.4%) in 2012.

Frequency of responses to no tobacco sales in 10 years statement 2010–2012, with 95% confidence bars.
Support for outdoor smoking ban
Support for banning smoking outdoors where young people go increased significantly from 51% (±1.3%) to 59% (±1.2%) from 2009 to 2011 (figure 3). The proportion of daily smokers supporting this statement was 16% (±2.6%) in 2011.

{kind=link}
{kind=link}
{kind=link}
Frequency of responses to outdoor smoking ban statement 2009–2011, with 95% confidence bars.
Support for raising price of tobacco products
Support to make cigarettes and tobacco more expensive so that young people cannot afford to buy it was not significantly different at 63% (±1.2%) in 2010 compared with 64% (±1.3%) in 2011. The proportion of daily smokers agreeing was 13% (±2.7%) in 2012.
Discussion
This study demonstrates majority support among young people for the New Zealand smoke-free goal and measures aimed at increasing the price of tobacco products or reducing their availability and visibility. For each statement, no more than 19% of students disagreed in the most recent year of data available. This means that for each statement, those who agreed with the statement outnumbered those who disagreed by at least 3 to 1. Smoking status was the strongest predictor of opposition to these measures, which is consistent with previous New Zealand and international studies.19–21 The increase in support for the statements across all smoking categories suggests that our findings are not solely a result of the decreasing smoking rates among adolescents. Increasing agreement (and declining disagreement) with the five measures tested should encourage policy action, particularly as majority support for each measure already exists and seems likely to grow.
This study extends earlier New Zealand research by demonstrating teenagers’ support for specific endgame measures14 ,21 and presenting the growth in that support over time. Similar findings have been reported separately in relation to the plain packaging of tobacco products.22 The study provides further evidence that support for tobacco control measures is associated with a lower risk of smoking in 14–15-year-old children.
Given the relative lack of research in this area internationally, it is difficult to provide any meaningful comparisons between countries at this time. However, evidence that young people support tobacco control measures in Canada,23 and similar associations between support for tobacco control measures and smoking status among youth in California,19 ,20 suggest our results are comparable to those reports from other jurisdictions with comprehensive tobacco control programmes or that are pursuing endgame strategies.
We cannot with certainty state why support for tobacco control measures has increased over recent years. However, we suspect that several factors may be influencing our findings. The measures introduced since 2009 attracted prominent media attention both leading up to and during any changes and may make tobacco control more salient to young people. Health education about tobacco in schools and ongoing mass media campaigns, including a specific youth-oriented campaign ‘Smoking—Not Our Future’, which has run continuously since 2008, have also denormalised smoking.24 National total population tobacco-use rates have also been falling: the most recent New Zealand census data (from 2013) demonstrate a current smoking rate of 15% (down from 19% in 2006).25 Overall, adolescents’ environments have become markedly less accepting of smoking, changes that are very likely to foster and reinforce smoke-free attitudes, and depress intentions to experiment with smoking.
Strengths of this study include the very large survey sample sizes covering students throughout the country and the availability of data over several years. However, the study has some limitations. The brevity of the questionnaire (to minimise respondent burden) limits our ability to examine in detail why young people hold the attitudes that they do. Qualitative studies are required to address this question and explore the factors underlying adolescents’ attitudes including how temporal factors, such as the perceived time to 2025, differ from adults’ perceptions. Students from low SES schools students were under-represented in the survey (although we attempt to adjust for this by using weighted analyses). In general, the demographic characteristics of the study participants were similar to the overall target population, suggesting that selection bias was not a serious issue. Nevertheless, trends in the survey results should be interpreted with caution, particularly for the fewer outlets selling tobacco products statement as the wording changed slightly over the study period.
The growing support for tobacco control measures and the tobacco endgame among adolescents is very encouraging to supporters of the Smokefree 2025 goal for several reasons. First, antismoking and pro-tobacco control attitudes are strongly associated with reduced risk of smoking among adolescents.10 If support for tobacco control continues to increase, tobacco use may continue to decrease. Second, the high support shown by most adolescents suggests they believe the measures tested may reduce the harm tobacco causes to themselves and their peers. Third, the strong support for tobacco control may encourage decision-makers to support robust tobacco control measures and to prioritise the achievement of tobacco endgames like New Zealand's Smokefree 2025. Finally, some may view the lower level of support among smokers as a cause for concern. However, we suggest this finding may reflect reluctance among adolescents who smoke to support specific tobacco control measures that threaten their continued smoking. If this is correct, reduced levels of support may indicate the measures’ likely effectiveness at reducing youth smoking.
The government and policymakers should be encouraged by the majority support demonstrated here and act promptly to implement comprehensive tobacco control measures. Reducing the number of retail outlets for tobacco products, implementing wider smoking bans in outdoor places (particularly where young people go) and raising tobacco prices are likely to be important components of endgame strategies. Individually and collectively, they will denormalise tobacco use, decrease smoking initiation and increase quit attempts. Most importantly, these measures will help protect the current and next generation of New Zealanders from the tobacco epidemic.
What this paper adds
We contribute data to the limited international evidence on support by young people for tobacco control measures.
There is majority support for a range of tobacco endgame control measures among New Zealand 14–15 year olds.
This support has been growing over the years 2009–2012.
The strongest predictor of support for the measures is smoking status of the individual: support decreases as self-reported smoking frequency increases.
Acknowledgments
The authors thank ASH New Zealand for supplying the data; we especially acknowledge the Health Promotion Agency for producing the survey instruments, managing the data collection process and setting up and maintaining the datasets. The authors thank the students who participated in all of the ASH New Zealand ‘Year 10’ surveys.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
Contributors RJ was responsible for drafting the manuscript. BH was responsible for coordinating access to the dataset and conducting the analyses. RE and JH obtained funding for the project. All authors participated in the study design, analysis interpretation and manuscript preparation.
Funding The ASH surveys were funded by the New Zealand Ministry of Health.
Competing interests Although we do not consider it a competing interest, for the sake of full transparency we note that some of the authors have previously undertaken work for health sector agencies working in tobacco control.
Ethics approval New Zealand Ministry of Health Multiregional Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.