Article Text

Abstract
Objective Studies evaluating the long-term impact of smoking laws on secondhand smoke (SHS) exposure using airborne markers are scarce. This study aimed to assess the long-term impact of the Spanish smoking law on SHS levels, using a specific and objective marker.
Methods Follow-up study, measuring vapour-phase nicotine levels before the implementation of the law and 6, 12 and 24 months after the initial assessment. A total of 443 samples were taken at baseline in eight different regions in offices in the public administration, private sector, universities and hospitality venues.
Results Two years after the law was implemented, the nicotine concentration decreased by a minimum of 60% in public administration, university and private sector offices, as well as in venues where smoking was totally banned. However, nicotine levels significantly increased by 40% in hospitality venues allowing smoking. No significant differences were found in hospitality venues with areas for smokers and non-smokers or in pubs and discotheques.
Conclusions Two years after the smoking law came into force, levels of SHS exposure in the workplace were significantly lower than before the law was implemented. Importantly, however, SHS levels were even higher than before the law was implemented in venues still allowing smoking. The data obtained in this study clearly show that the ‘Spanish model’ is not protecting the health of hospitality workers and that a complete ban is required. Furthermore, this study highlights the importance of long-term monitoring of compliance with smoking laws over time.
- Secondhand smoke
- passive smoking
- evaluation
- smoking law
- Spain
- environment
- environmental tobacco smoke
- public policy
Statistics from Altmetric.com
- Secondhand smoke
- passive smoking
- evaluation
- smoking law
- Spain
- environment
- environmental tobacco smoke
- public policy
Introduction
During the past decade, numerous countries have implemented smoking control laws aiming to reduce secondhand smoke (SHS) exposure and its health effects, such as respiratory symptoms, heart diseases and lung cancer.1 The smoking control laws enacted so far across Europe cover a wide range of restrictions, from total bans to partial restrictions allowing smoking areas in selected venues.2 In some countries, such as Ireland and Scotland, total bans were implemented, prohibiting smoking in all workplaces including hospitality venues without exceptions. In other countries, such as Italy, laws demanding complex technical requirements in relation to the physical separation and ventilation for smoking areas were implemented. Finally, in countries such as Spain (before 2011) and Portugal, only partial restrictions were applied, depending on the size of the venue. In these countries, hospitality venues over 100 m2 can designate a physically separate smoking area (occupying 30% of the total area of the venue), while venues smaller than 100 m2 may choose whether to allow smoking or not.3 ,4
Not surprisingly, the Spanish smoking law implemented in 2006 was being promoted by the tobacco industry in other countries as a model of smoke-free legislation,5 ,6 citing arguments such as ‘tolerance for smokers’ or even the potential losses that the hospitality sector would suffer with a total ban. However, economic studies previously carried out in other countries showed no negative impact of smoking bans.7 ,8
Studies evaluating the impact of these laws have shown significant reductions in SHS exposure as well as in the health effects associated with SHS exposure in venues with total bans.8 Most of these studies used pre-post designs, measuring either biological or airborne markers of SHS exposure before and after the implementation of the ban or analysing changes in self-reported exposure through repeated cross-sectional surveys. However, most of these studies have only measured the impact in the short term or medium term, with a follow-up period ranging from a few weeks to 12 months. Studies evaluating the long-term impact of these laws on the SHS exposure levels using airborne markers are scarce; to our knowledge, only two studies have been published to date.9 ,10 Therefore, there is a lack of evidence on the maintenance of the effects of smoking control laws in the long term.
The aim of this study was to assess the long-term impact of the Spanish smoking law on SHS levels, using an objective and specific marker.
Methods
We conducted a follow-up study, measuring vapour-phase nicotine levels before (October–December 2005) the implementation of the law (1 January 2006) and 6, 12 and 24 months after the initial assessment.
This study was carried out in eight regions of Spain (Balearic Islands, Cantabria, Catalonia, Extremadura, Galicia, La Rioja, Madrid and Valencia). In each region, a minimum of 50 samples were taken according to non-proportional quota sampling based on the type of setting (offices in the public administration, private sector, universities and hospitality venues) and the size of hospitality venue (over or under 100 m2). The premises within each type of venue were selected following convenience sampling based on feasibility and accessibility of the researchers to the venues.
We included offices with a minimum of five workers in the local, regional and national administration. For each of these administrative levels, one building was selected in each region, and four environmental samples were taken from each building. In each region, a university was selected from which four air samples were taken. In the private sector, six samples (from three different buildings) in each region were taken from small firms (<10 workers) and six samples (from four different buildings) were taken from medium-sized firms (10–50 workers). The offices from the private sector included in the study belong to the service sector. In the hospitality sector, we selected four bars/restaurants over 100 m2, four bars/restaurants below 100 m2 and four discotheques/pubs in each region, taking one sample from each venue. In bars/restaurants with separate areas for smokers and non-smokers after the law came into force, samples were taken from both areas. Samplers were placed in the reception area, corridors, offices (desk positions) and toilets in public administration offices, universities and medium-sized offices in the private sector; in the reception area and offices (desk positions) in small offices in the private sector and in the main dining room in bars/restaurants. The owners and managers of the selected facilities and venues were contacted either by telephone or by letter to explain the details of the study and to request permission. After permission was obtained, we arranged an appointment to place the samplers.
Vapour-phase nicotine was measured using SHS passive samplers, following the method described and validated by Hammond11 and used in previous studies of SHS assessment.12–15 The samplers consisted of a 37-mm diameter plastic cassette containing a filter treated with sodium bisulphate. These samplers were manipulated by instructed personnel according to a common protocol and were placed in all the settings studied except pubs and discotheques for 7 days. The samplers had to hang freely in the air and were not to be placed within 1 m of an area where there was a regular smoker or where air did not circulate (eg, a corner, under a shelf or buried in curtains). In discotheques and pubs, where the expected nicotine concentration was higher, samplers were taken as personal monitors (wore by a trained person) during a one-night period ranging between 4 and 5 hours. Personal samplers had to be clipped to a shirt collar or lapel, with the windscreen facing out, away from the clothes.
For each sample the following data were recorded: the sample's code, region, setting, location, date and time of placement and removal, and smoking policy (smoking allowed, completely banned or partially banned in separate zones). Information on sampling area, sampling volume and ventilation in each establishment was recorded to evaluate extreme or inconsistent values. Nicotine concentrations below the quantification limit were assigned a value of 0.01 μg/m3, corresponding to half the value of quantification limit for one sample exposed over a one-week period. For quality control purposes, blank filters were placed within sampling filters (one filter in 20) and all had nicotine concentrations below the quantification limit. Nicotine analysis was conducted at the Laboratory of the Public Health Agency of Barcelona, using the gas chromatography/mass spectrometry method. The limit of quantification was 5 ng per filter. The time-weighted average nicotine concentration (μg/m3) was estimated by dividing the amount of extracted nicotine by the volume of air sampled (estimated flow rate (24 ml/min) multiplied by the total number of minutes the filter had been exposed).
The statistical analysis was restricted to places where nicotine measurements were taken at baseline and at 6, 12 and 24 months of follow-up (linked samples). Given the skewed distribution of nicotine concentration, we used median and IQRs to describe the nicotine concentration by setting. The percentage variation between baseline and 2 years, and between the first and second year, was assessed. We compared paired differences using the non-parametric Friedman test and statistical significance was set at 5% (α error). We used SPSS v 12.0.1 for all the analyses.
Results
Of the 443 measurements carried out at baseline (2005), 355 were repeated at the four measurements (table 1).
Settings studied and number of samples at baseline, 6, 12 and 24 months after the Spanish smoking law (January 2006)
In public administration and university offices the nicotine concentration decreased over time from 0.21 μg/m3 (0.08–0.56) to 0.05 (0.01–0.12) μg/m3 and from 0.24 μg/m3 (0.08–0.67) to 0.08 (0.04–0.16) μg/m3, respectively. In the private sector, the nicotine concentration went from 0.40 μg/m3 (0.07–1.29) to 0.06 μg/m3 (0.01–0.16) 24 months after the law came into force (table 2).
Median nicotine concentration (μg/m3) in offices at baseline and 6, 12 and 24 months after the Spanish smoking law (January 2006)(samples repeated at the four measurements)
In hospitality venues where smoking was completely banned, nicotine concentrations decreased over time, from 2.95 μg/m3 (2.23–4.07) at baseline to 0.11 μg/m3 (0.06–0.40) two years after the ban was implemented. However, in hospitality venues allowing smoking, the nicotine concentration increased two years after the law from 7.07 μg/m3 (2.00–11.78) to 10.12 μg/m3 (3.77–18.00) (table 3).
Median nicotine concentration (μg/m3) in hospitality venues at baseline and at 6, 12 and 24 months after the Spanish smoking law (January 2006) (samples repeated at the four measurements)
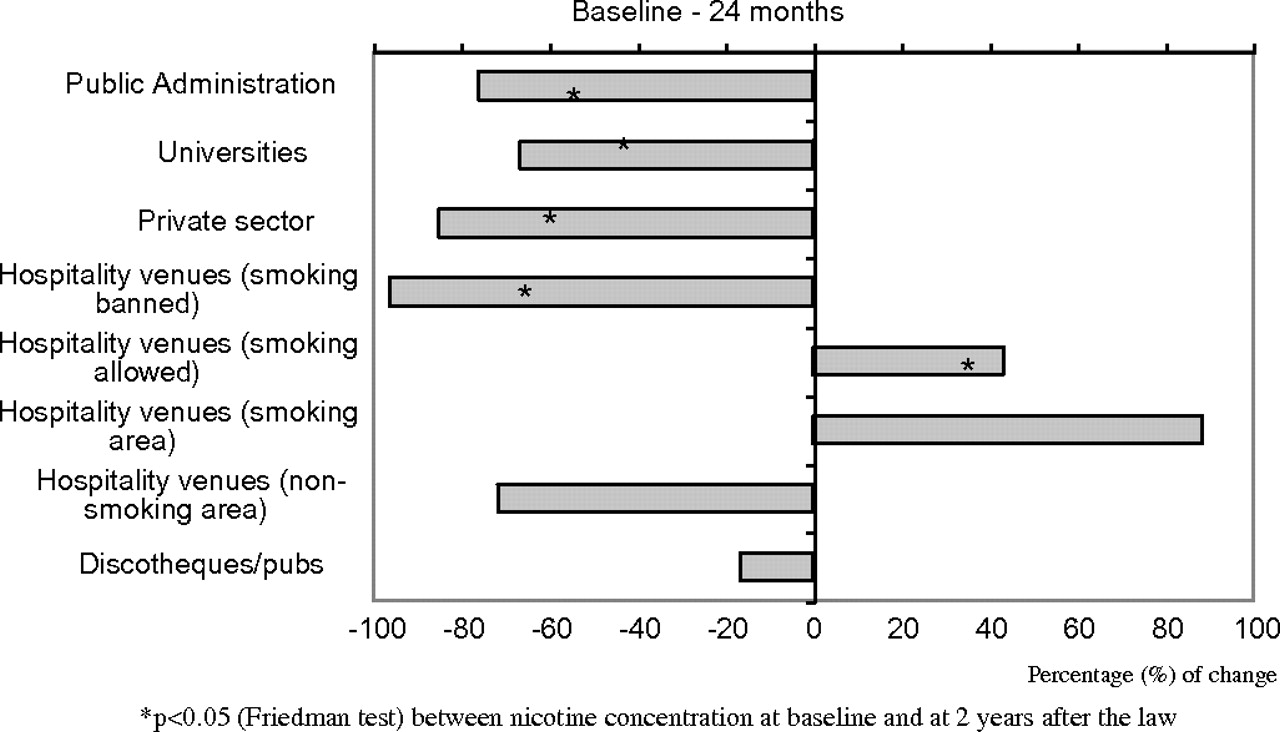
Two years after the law was implemented, the nicotine concentration decreased by a minimum of 60% in public administration, university and private sector offices, as well as in venues where smoking was totally banned. However, nicotine levels significantly increased by 40% in hospitality venues allowing smoking. No significant differences were found in hospitality venues with areas for smokers and non-smokers or in pubs and discos (figure 1).

Percentage variation of nicotine concentration between measurements at baseline and at 24 months after the Spanish smoking law (January 2006).
The percentage variation between the first and the second year after the law was implemented revealed a significant increase in nicotine concentration in the private sector as well as in non-smoking areas in hospitality venues with separate areas for smokers and non-smokers (figure 2).

{kind=link}
{kind=link}
Percentage variation of nicotine concentration between measurements at 12 and at 24 months after the Spanish smoking law (January 2006).
Discussion
SHS exposure was reduced two years after the Spanish smoking law was implemented in offices in the public administration, universities, private sector and hospitality venues that adopted a total smoking ban. However, in bars and restaurants where smoking is still allowed, the nicotine concentration was even higher than before the law was implemented. Therefore, hospitality workers in these venues—80% of the total hospitality venues in Spain16—continued to be at risk of diseases caused by SHS, mainly lung cancer and coronary heart disease.
One of the strengths of this study is that it is the first follow-up study in Europe to assess the impact of a smoking law on SHS levels, by using a specific marker, in offices and hospitality venues two years after the law came into effect. Most studies published to date have only assessed the short-term or medium-term impact (maximum one year) of the smoking laws. Most of these studies have noted their short duration as a major limitation.11 ,12 ,17–20 The marker used to measure SHS exposure in this study (vapour-phase nicotine) is a specific marker, thus guaranteeing the study's internal validity. Ours is the largest of all the evaluative studies published in Europe to date, with more than 1400 nicotine samples taken and analysed during the fieldwork period. The follow-up rate (80%) was higher than those found in other reports using airborne markers, even though the follow-up in those studies was only one year. The losses in our study were mainly caused by venues that either closed or moved to another place over the years. Furthermore, while most publications have focused exclusively on the hospitality sector, our study also includes other workplaces such as offices in the public and private sector. Finally, samples were taken from eight different regions of Spain, representing not only distinct demographic, cultural and socioeconomic contexts within Spain but also different degrees of compliance with the law.
One of the limitations of the study is the convenience sampling approach used to select the venues. However, to avoid selection bias and to maximise external validity, we included venues stratified by the most important potential confounders such as type of workplace, size, smoking regulation and geographical area. Another possible limitation is the absence of a control group. However, equivalent comparison groups in evaluative public health research are not always feasible because of the complexities of the interventions evaluated,21 and because the law was implemented nationwide with no exemptions within Spain. However, the particularity of the law regarding the hospitality sector has allowed comparison between hospitality premises with no prohibition, those with smoking areas and those with complete bans.
This study goes a step further than previous investigations in Spain. All prior Spanish studies assessed the impact of the law at a maximum of 12 months after the law came into force. Some evaluated the impact of the law on the prevalence of SHS exposure,22 ,23 while others assessed the impact of the law on levels of SHS exposure.18 ,19 These studies showed a clear impact of the law on the prevalence and levels of SHS exposure in workplaces, as well as in hospitality venues that banned smoking.24 Their findings were consistent with those found in other countries such as Ireland or Scotland,17 ,25 where a number of studies have measured the impact of smoking laws on SHS levels at a maximum of one year. However, studies over a longer period are scarce. We identified two studies in Europe that measured the impact of smoking laws two years and three years after implementation using environmental markers. The first, carried out in Finland,10 measured nicotine concentrations in a sample of workplaces and found a reduction in these concentrations even three years after the implementation of the law. The second, performed in Italy,9 measured nicotine concentrations before the smoking law and two years after the law was implemented and found that the median nicotine concentration strongly decreased. Another study26 measured the impact of the Italian law using data from population-based surveys: the proportion of people reporting good compliance was lower two years after the law was passed than in the first year after its implementation. These results are consistent with our finding of an increase in SHS exposure in offices of the private sector and hospitality venues allowing smoking between the first and second year after the law.
Although nicotine concentrations significantly decreased compared with baseline concentrations in private sector offices, nicotine levels significantly increased between the first and the second year after the law was implemented. Furthermore, SHS levels in non-smoking areas in hospitality venues also significantly increased between the first and the second year after the law came into force. The increase observed in certain venues could be attributed to a lack of enforcement of the law, since the quality of implementation of these laws is a key factor in understanding the outcome evaluation. Unfortunately, indicators of enforcement are rarely published, although some data have been published in Spain during the last few years. One study27 approached public health departments in all Spanish regions—since enforcement of the law is the duty of regional authorities—and recorded the number of inspections and sanctions after the law. This study showed that in the first year after the law 15 800 inspections were carried out, but resulted in only 586 (3.7%) sanctions, mostly in the hospitality sector. A study evaluating28 compliance with the law in hospitality venues showed that 37% of these venues did not have adequate external signs. Furthermore, wide variation among regions was observed. In the long term, this lack of enforcement could erode the effect of the law, especially when the law itself permits exceptions and interpretations. Indeed, some regions have responded to the national law with regional laws permitting exceptions, which have been legally challenged by the national Ministry of Health.
In conclusion, two years after the smoking law came into force, levels of SHS exposure in the workplace were significantly lower than before the law was implemented. However, exposure increased in private sector offices between the first and second year after the law, what could be interpreted as a potential relaxation of compliance with the law. This study highlights the importance of long-term monitoring of compliance with smoking laws over time. Especially important is the finding that hospitality venues where smoking was still allowed (70% of the venues in our study) had even higher SHS levels than before the law—probably due to a ‘concentration’ of smokers in those venues where smoking was allowed. Therefore, far from being protected, a substantial number of hospitality workers were exposed to higher SHS levels than before the law was implemented. Furthermore, it is also important to notice that in non-smoking areas the nicotine concentration decreased regarding the baseline but it never reached the substantial decrease observed in venues where smoking was totally banned. The data obtained in this study clearly show that the ‘Spanish model’6 was not protecting the health of hospitality workers and that a total ban was required. From 2 January 2011, the Spanish smoking law bans smoking in all hospitality venues with no exceptions.29
What this paper adds
This is the first follow-up study to assess the impact of the Spanish smoking law on SHS exposure in offices and hospitality venues two years after the law came into effect.
SHS exposure increased in private sector offices between the first and second year after the law was implemented, indicating some relaxation of compliance with the law and highlighting the importance of long-term monitoring of compliance with smoking laws over time.
Especially important is the finding that venues still allowing smoking had even higher SHS levels than before the law was implemented. Therefore, far from being protected, a substantial proportion of hospitality workers were exposed to higher SHS levels than before the law.
The data obtained in this study clearly show that the ‘Spanish model’ was not protecting the health of hospitality workers and that a complete ban was required.
References
Footnotes
↵* Spanish Smoking Law Evaluation Group Agència de Salut Pública de Barcelona (Barcelona, Spain): Carles Ariza, María José López, Manel Nebot, Francesca Sánchez-Martínez, Francesc Centrich, Glòria Muñoz, Eulàlia Serrahima, Institut Català d'Oncologia (Hospitalet, Spain): Esteve Fernández, Marcela Fu, Jose M Martínez-Sánchez, Anna Martín, Josep Maria Borràs, Stephanie Rania, Jorge Twose, Anna Schiaffino; Generalitat de Catalunya (Barcelona, Spain): Esteve Saltó, Araceli Valverde, Meia Faixedas, Francesc Abella, Enric Rovira; Xunta de Galicia (Santiago, Spain) Mónica Pérez-Ríos, Begoña Alonso, María Isolina Santiago, María Jesús García, Sergio Veiga; Govern de les Illes Balears (Mallorca, Spain): Arturo López, Elena Tejera, Magdalena Borrás, José A Ayensa, Ernesto Pérez; Generalitat Valenciana (Valencia, Spain): Francisco Carrión, Pepa Pont, José A Lluch; Gobierno de Cantabria: M Eugenia López, Sonia Álvarez, M Emma del Castillo, Fernando Martín, Blanca M Benito; Hospital San Pedro de Alcántara de Cáceres (Extremadura, Spain): Juan Antonio Riesco; Comunidad de Madrid (Madrid, Spain): Isabel Marta, Almudena García, Carmen Estrada,Virgilio Blanco; Gobierno de La Rioja (Logroño, Spain): Ana Esteban, M Ángeles Hessel; Universidade do Minho (Minho, Portugal): José Precioso; Acadèmia de Ciències Mèdiques d'Andorra (Andorra la Vella, Andorra):Margarida Coll.
Funding This study was partially funded by the Ministry of Health Instituto de Salud Carlos III (FIS PI052293 and RTICC RD06/0020/0089), and supported by the Department of Health of each participating autonomous region. Funding from the Department of Universities and Research, Government of Catalonia (AGAUR SGR 2009-1345, SGR 2009-42 and 2009 SGR 192) is also acknowledged.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.