Article Text

Abstract
Objective: To examine the impact of smoke-free policies in Victorian gambling venues on electronic gaming machine (EGM) expenditure.
Method: Monthly EGM expenditure from July 1998 to December 2005, provided by the Victorian Commission for Gambling Regulation and the Office of the Liquor and Gambling Commissioner in South Australia, was analysed. The outcome measure was the ratio of monthly expenditure for Victoria to monthly expenditure in South Australia. Intervention analysis and autoregressive integrated moving average modelling were used to assess the impact of the smoke-free policy on expenditure.
Results: The smoke-free policy resulted in an abrupt, long-term decrease in the level of EGM expenditure. The mean level of monthly expenditure decreased by approximately 14%.
Conclusion: The smoke-free policy not only protects hospitality workers and patrons from exposure to secondhand smoke but has also had an impact on slowing gambling losses.
Statistics from Altmetric.com
Smoke-free policies were introduced into gambling venues in Victoria, Australia, to protect patrons and workers from the harmful effects of secondhand smoke and as a measure to reduce the addictiveness of gambling. There is no risk-free level of exposure to secondhand smoke. Smoke-free policies reduce the risk of premature death from lung cancer, respiratory and cardiovascular disease in non-smokers.1
Victorian gambling expenditure was $A4.251 billion in 2003–2004, with approximately 54% of this spent on gaming machines, also known as slot machines.2 Two previous studies from the United States have analysed the impact of smoke-free policies on gaming machine expenditure and the conclusions were mixed. Mandel et al.3 found no significant effect of the smoke-free law in three gambling venues in Delaware, USA; however, Pakko4 found a significant decrease in revenue when analysing the same data but with different model specifications. Another study from the United States found no effect of the smoke-free policy on profits from bingo and charitable gaming in Massachusetts, USA.5
Smoke-free laws commenced in Victorian gambling venues on 1 September 2002. The law requires that people must not smoke in venues with gaming machine areas that consist of only one room and gambling rooms in venues that consist of two or more rooms. The legislation includes bingo centres, the state’s casino (except the high rollers’ room) and pubs and clubs with electronic gaming machines (EGM). Victoria has a population of 4.9 million6 and the smoking prevalence of regular smokers was 18.3% in 2004.7 There are approximately 27 000 EGM in 523 pubs, gaming venues and licensed clubs in Victoria,8 with a limit of 105 machines per venue. The licensed clubs with EGM are sporting clubs and Returned and Services League branches. There are also approximately 2500 machines in the state’s casino. The casino’s gaming floor is more than 500 metres long and as well as EGM provides table games such as black jack and roulette.
For our analysis, South Australia was chosen as the comparison state because smoke-free regulations there were less restrictive than other states. For example, separate non-smoking rooms were not a requirement in South Australia. From 1 November 2005 no less than 25% of gambling areas had to be smoke free. Before this there were no restrictions. All other states required at least 50% of gambling areas to be smoke free.9 There are approximately 12 600 EGM in South Australia10 in 597 venues. Their casino has 950 machines. In 2003–2004 total gambling expenditure in South Australia was $A1.06 billion, with 68% on gaming machines.
Soon after the commencement of the legislation in Victoria, media reports stated that gaming revenue had fallen. The two main gaming operators in Victoria, Tabcorp and Tattersalls, reported revenue decreases of 7.6% and 10%, respectively, in the 2003 financial year when compared with the previous year.11 12 The state government reported an 8.5% drop in taxation revenue collected from EGM in 2002–2003, compared with the previous year.13 These results were attributed directly to the introduction of smoke-free policies in Victorian gambling venues.
A decrease in gambling expenditure was expected because of the known association between smoking and gambling. Smoking rates are higher among gamblers than non-gamblers (32% and 21%),14 and among problem gamblers smoking rates have been reported to range from 43% to 83%.15–18 Thirty-six per cent of patrons at gambling venues are smokers yet they contribute 50% of the gambling revenue.19
This paper examines the impact of smoke-free policies on EGM expenditure in Victoria. Three distinct hypotheses about the nature of the impact are examined. First, that the impact was abrupt and permanent; it resulted in a sudden and permanent shift in the level of expenditure. Second, that the impact was gradual and permanent; it resulted in a gradual change in expenditure and this accumulated effect was permanent. Third, that the impact was abrupt and temporary; it resulted in a sudden change, but this change disappeared in a relatively short time.
METHODS
Data sources and variables
Following the method of Glantz and Smith20 to account for underlying economic trends, unemployment and population changes, we computed the ratio of monthly net expenditure on gaming machines in Victoria to monthly net expenditure on gaming machines in South Australia from July 1998 to December 2005. Monthly net expenditure on gaming machines in Victoria and South Australia was obtained from the Victorian Commission for Gambling Regulation21 and the Office of the Liquor and Gambling Commissioner in South Australia.10
This ratio would be expected to decrease if the implementation of the smoke-free policy had the effect of reducing EGM expenditure in Victoria.
Statistical analyses
We used interrupted time series analysis (also known as intervention analysis) and autoregressive integrated moving average (ARIMA) modelling to estimate the effect of smoke-free legislation in Victoria (the intervention) on the ratio of Victorian to South Australian EGM expenditure (the time series). These statistical techniques are described in the Appendix. We examined three intervention models, based on the type of the impact of the intervention on the time series: abrupt and permanent; gradual and permanent; and abrupt and temporary. Each model was tested separately. The first model suggests that intervention results in a sudden shift in the level of the time series, and that this shift will be permanent. The second model suggests that the intervention will gradually change the level of the time series, and that this accumulated effect will be permanent. Finally, the third model suggests that the intervention will result in a sudden change in the time series, but that this change will disappear in a relatively short period of time. The ARIMA procedure in SAS/ETS22 was used for the analyses, and parameter estimates were computed using the conditional least-squares estimation method.
RESULTS
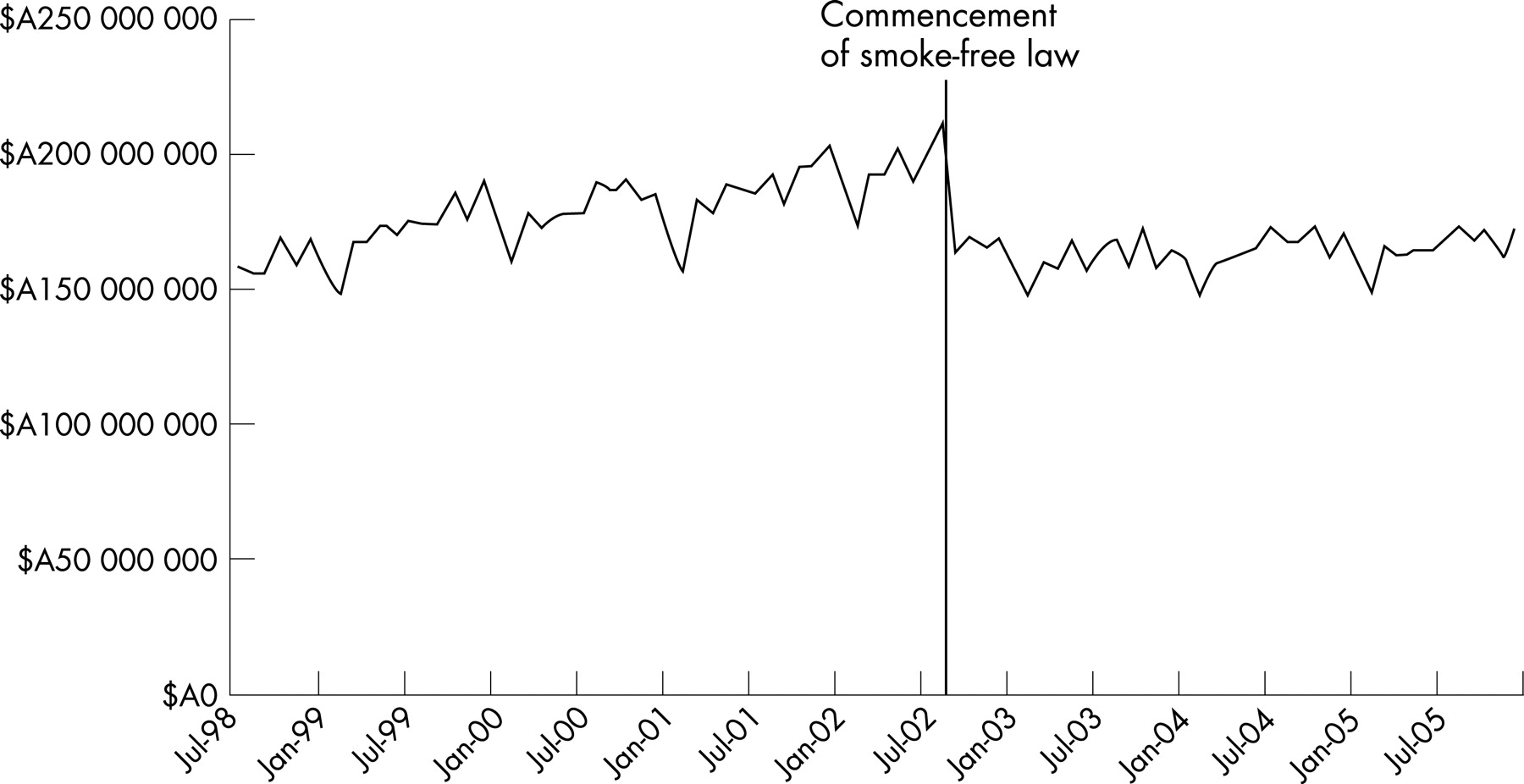
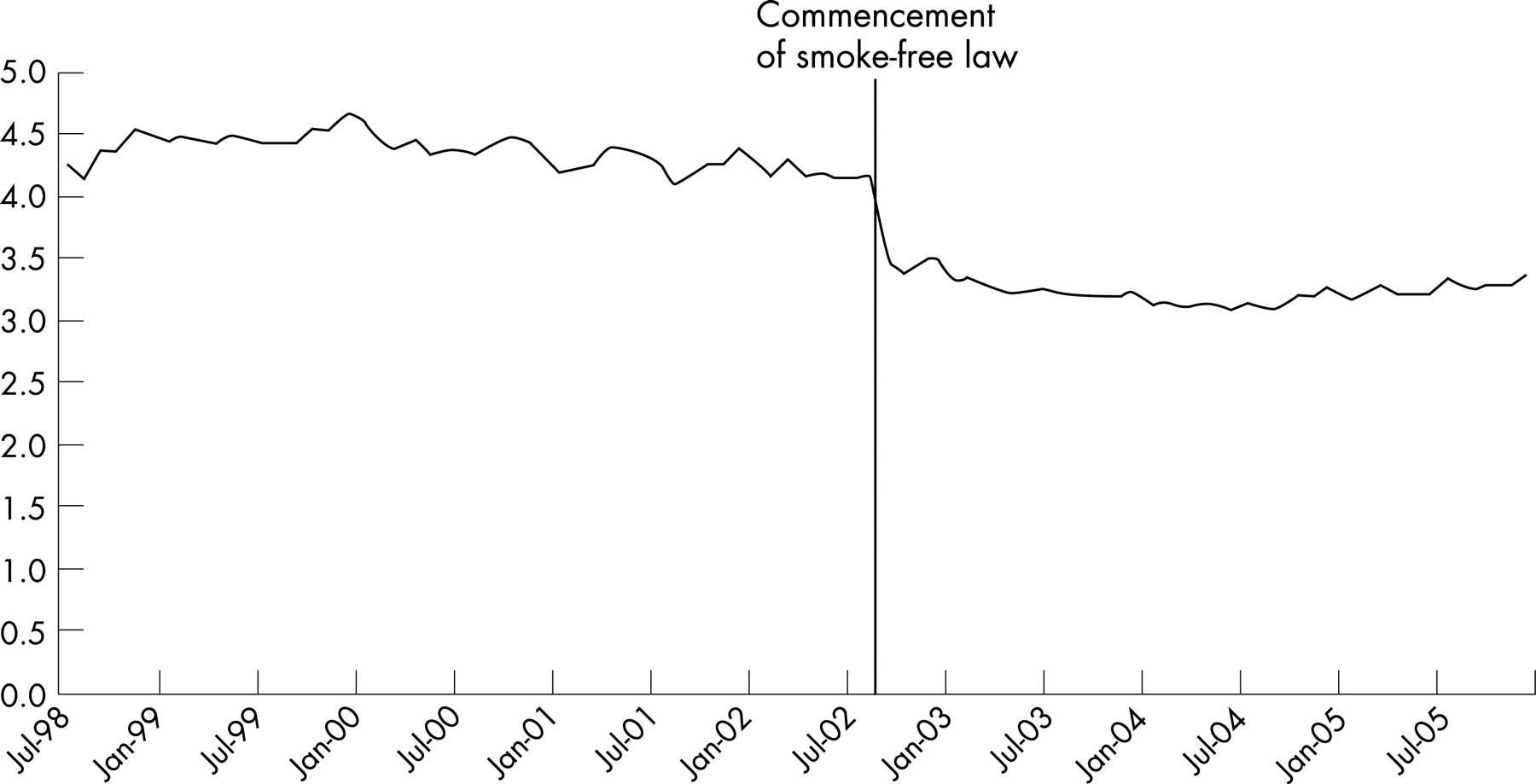
Figure 1 shows the Consumer Price Index-adjusted plots of net monthly EGM expenditure in Victoria from July 1998 to December 2005.23–30 The vertical line represents 1 September 2002, when the smoke-free law (the intervention) came into effect. The average monthly turnover in the year before the introduction of the law was $A218 million compared with $A188 million after the law came into effect. The graph shows an upward trend to August 2002, followed by a declining trend indicating a decrease in expenditure. The plot of the ratio is shown in fig 2. There is a slight downward trend before the smoke-free law and this becomes more apparent after the commencement of the smoking restrictions.


{kind=link}
{kind=link}
We used data before September 2002 for the identification of the time series. The examination of the autocorrelation and partial autocorrelation function, and the diagnostic Q statistics revealed that the error process of the time series could be best described as ARIMA (0, 1, 4). This indicates no autoregressive parameter, first differencing and a fourth order moving average parameter (θ4). Table 1 provides parameter estimates for the impact of smoke-free legislation on the ratio of Victorian to South Australian EGM expenditure. The diagnostic test of the Q statistics indicates that the models were statistically adequate. The best model in table 1 is Model 1, which indicates that there was a significant abrupt and permanent decrease in the ratio of Victorian to South Australian gaming expenditure after the introduction of smoking restrictions. This represents an overall decline of 0.73 in the ratio, which is equivalent to approximately a 13.8% decrease in the mean level of monthly EGM expenditure in Victoria. The rate parameter δ in Model 2 is not significant and does not provide support for the model of gradual and permanent impact. The rate parameter in Model 3 is slightly larger than 1, which indicates that there was no decay in the initial abrupt change in the time series.31
DISCUSSION
An immediate decrease in EGM expenditure was apparent as a result of the introduction of the smoke-free policy, and expenditure remained below the level before the introduction of the policy. This analysis of EGM expenditure is to the end of December 2005. The trend of the expenditure line in fig 1 after January 2003 indicates a very gradual increase and it is possible that in the future expenditure levels could return to those before the introduction of the smoke-free policy.
A number of other strategies to minimise the harm from gambling were introduced after the smoke-free policy had commenced. From 1 January 2003 access to cash and automated teller machine (ATM) facilities at gambling venues was limited to $A200 per transaction, no cash withdrawals were possible from credit accounts from ATM facilities, a limit was placed on poker machine spin rates, and player information on the odds of winning had to be displayed.32 On new games approved after 1 January 2003, autoplay facilities were banned. This requires that a player fully releases a button before pressing it again to effect the next spin. Note acceptors for $A100 were also banned and a maximum bet limit of $A10 was enforced.32 From 1 January 2004 all forms of gaming machine advertising were banned. In analyses not reported here, we examined the effect of the set of strategies implemented in January 2003 and the advertising strategy put in place in January 2004, and found that neither had an impact on the outcome of our study (p = 0.925 and p = 0.507, respectively).
Adult population growth could potentially distort the estimates of the effect of the smoke-free policy on EGM expenditure if the population grew at a different rate in Victoria compared with South Australia. Growth in the adult population would be expected to increase gaming expenditure. Over the period 1998 to 2005 the adult population growth in Victoria was 10% compared with 5% in South Australia.6 33–40 This only adds strength to our findings that the smoke-free policy caused a decrease in EGM expenditure in Victoria.
Similarly, a significant change in the number of EGM in one state could potentially distort the estimates of the effect of the smoke-free policy on EGM expenditure. From June 2001 to June 2005 the number of EGM in Victoria decreased by 1.2% and by 0.2% in South Australia.10 21 The expected effect of the removal of machines in Victoria was to reduce the level of gaming expenditure. A study examining the effect of this policy found, however, that there was no evidence that venues from which machines had been removed suffered larger falls in EGM expenditure than any other venues.41 It therefore appears that the larger decrease in the number of machines in Victoria would have had little effect on our findings.
The way the smoke-free policy has reduced gambling activity is not certain and could take a number of different forms. For example, it may mean that gamblers are spending more time in areas where smoking is permitted, therefore reducing the time they spend at the machines, or that they are leaving the venue earlier after taking a break to smoke rather than staying. There has also been a decline in the percentage of both smokers and non-smokers regularly visiting gambling venues in Victoria (D. Germain, Centre for Behavioural Research in Cancer, written communication, November 2005). In 2001, 20% of regular smokers visited a gambling venue at least once a month and in 2003 this had dropped to 14%. Fifteen per cent of non-smokers were going once a month in 2001 compared with 11% in 2003.
What is already known
Two previous studies from the United States have analysed the impact of smoke-free policies on gaming machine expenditure; however, their conclusions were inconsistent.
What this paper adds
Our analysis indicates that the smoke-free policy in gambling venues resulted in a sudden and long-term decrease in gaming machine expenditure. Policy makers should be aware that the policy in gambling venues not only improves the health outcomes of workers and patrons by protecting them from secondhand smoke but may also slow the losses of gamblers.
Numerous studies have indicated that there is no negative impact of smoke-free policies on sales in restaurants and cafes.20 42–47 The reaction to the smoke-free policy from restaurant patrons, however, appears to be different to that of gamblers using EGM. In restaurants, smokers appear to have adjusted their behaviour by limiting smoking to before or after a meal. If a small proportion of smokers avoids restaurants or leaves earlier, this would be balanced out by the non-smokers who previously avoided smokey restaurants. In gambling venues with EGM, each minute away from a machine is money not spent, and smokers are not only stopping play to smoke but could be leaving earlier. As mentioned previously, non-smokers do not appear to have increased patronage (D. Germain, Centre for Behavioural Research in Cancer, written communication, November 2005). Gambling control advocates expected the legislation would be useful in curbing excessive gambling among EGM users in that enforcing a break in play would prompt many gamblers to reconsider their gambling.48
The state’s casino experienced only a 0.6% decrease in gaming machine revenue from 1 September to 30 June 2003, when compared with the same period in 2001.49 It appears that the casino was less affected by the smoking restrictions; first, because smoking areas are available close to groups of EGM, and second, that a player can interrupt play and transfer credit to a card, whereas in other venues players taking a break have to ‘cash out’ and receive coins.41 This interruption seems to have had a stronger psychological incentive to stop playing. This respite from playing may provide time for reflection on losing. The fact that the casino was less affected by the smoke-free policy than other venues suggests a possible differential impact of the policy depending on the type of venue. An area for future research could be to investigate the impact of the policy on different types of venues.
The gaming industry introduced a number of strategies to offset the smoke-free policies by encouraging smokers to continue playing in a smoke-free environment.19 These strategies have included changes to smoking rooms, with the provision of other gaming facilities, large screen televisions and comfortable seating, allowing smokers to reserve machines while smoking, positioning ATM and smoking facilities in view of the EGM and training staff in order to keep people at the machines to play continuously, for example by offering free drinks and food.19
When people spend money on gambling they forgo other expenditures and savings that would otherwise have generated incomes. Expenditure alternatives forgone to finance gambling have been estimated by comparisons of spending patterns of gambling and non-gambling households and problem gamblers.50 It has been shown that gamblers’ expenditure on housing, particularly home ownership, is significantly less than non-gamblers. Gamblers save less than non-gamblers resulting in fewer financial assets. Although some expenditure items are complementary to gambling, such as alcohol, tobacco and eating out, general retail expenditure is forgone. The average expenditures that are reduced are retail sales (23%), debt financed (12%), housing construction (35%), financial assets (24%) and taxation (7%). It is likely that if the level of gambling is falling gambling debts would be repaid and general retail expenditure as well as expenditure in the other areas would increase.50
Given that the smoke-free policy had a significant impact on gambling behaviour, it would be expected that employment in this sector would also be affected. Employment decreased slightly after the introduction of the policy; however, employment levels in this sector peaked in 2005. The average quarterly employment of employees in pubs, taverns, bars and clubs decreased by 4% in 2003 (25 050) and 2% in 2004 (25 625) when compared with 2002 (26 200). In 2005, however, there was a 16% increase (30 425) when compared with 2002.51 It appears that the policy may have had a temporary effect on employment in the sector, but within three years the number of employees exceeded levels before the policy was introduced.
An abrupt decrease in EGM expenditure resulted from the introduction of the smoke-free policy in gambling venues, and levels remained below those before the commencement of the policy. The sustained decrease in expenditure may be supported by a number of other policies to minimise harm from gambling. The purpose of the smoke-free policy in gambling venues is to improve the health outcomes of workers and patrons by protecting them from secondhand smoke. In addition, it has been a substantive intervention in slowing gaming losses.
Acknowledgments
The authors would like to thank Todd Harper for useful comments on a previous draft.
Appendix: ARIMA and interrupted time series analysis
A brief explanation of the three components of ARIMA models follows: “autoregression (AR)”, “integration (I)” and “moving average (MA)”. Let … Yt−1, Y, Yt+1, … denote observations at times … t−1, t, t+1. …. Let … at−1, at, at+1 … be random error (or “random shock”), which is randomly drawn from a normal distribution with zero mean and constant variance. The basic (first order) “autoregressive” model is written as:
Yt = θ0 + φ1Yt−1 + at,
where θ0 is the intercept parameter and φ is the first order autoregressive parameter to be estimated. The basic (first order) “moving average” model is written as:
Yt = θ0 + at − θ1at−1,
where θ1 is the first order moving average parameter to be estimated.
Time series frequently exhibit a trend or a drift, which is referred to as “integration”. An integrated time series must be made “stationary” before autoregressive and moving average parameters can be estimated. Stationarity or detrending is achieved by “differencing” the time series, for example by transforming each observation (Yt) to the difference between that observation and the previous observation (Yt – Yt−1).
The process of determining the correct error process that describes a time series requires a procedure consisting of three steps: identification, estimation and diagnosis. This procedure is repeated until a satisfactory model is achieved. The inspection of autocorrelation and partial autocorrelation function, which describe the correlation of the series with its various lags, is instrumental in the process of identification. A satisfactory model is one whose residuals are “white noise”, i.e. the series is stationary and there is no indication of autocorrelation. The diagnostic Q statistics are commonly used to test the null hypothesis of white noise.52 Each Q statistic is a chi-square statistic calculated from a set of six or more autocorrelations. For example, Q6 is computed from the correlation coefficient of the time series with its first, second, third, fourth, fifth and sixth lags.
In interrupted time series analysis, once the error process of the time series is satisfactorily determined, an “intervention component”53 (also called a “transfer function”) needs to be identified. The intervention component describes the impact of the intervention on the time series. We examined hypotheses relating to three types of impact: abrupt and permanent; gradual and permanent; and abrupt and temporary.
Let Nt be the noise or the error component as specified by the ARIMA model described above, and It be the intervention dummy variable coded “0 = before the intervention” and “1 = at and after intervention”. The intervention model with an abrupt and permanent impact can be written as:
Yt = ωIt + Nt,
where ω is the effect of intervention, i.e. the net difference in the level of the time series before and after the introduction of the intervention. The intervention component in this model is ωIt. The intervention model with a gradual and permanent impact can be written as:
Yt = [ω/(1 − δB)]It + Nt.
The intervention component is [ω/(1 − δB)]It. Here ω is the change in the level of time series at the moment of intervention, δ is a rate parameter describing how quickly (or slowly) the asymptotic impact (or eventual change) is realised, and B is the so-called “backshift operator” such that, for example, BYt = Yt−1. The same intervention component can be used for the model with an abrupt but temporary effect, except that It should be coded such that “0 = before and after intervention” and “1 = during intervention”.53–55 In an abrupt but temporary model ω is again the impact of intervention at the moment of intervention and δ is a rate parameter describing the pace at which the initial effect decays to zero.
REFERENCES
Footnotes
Competing interests: None.
Funding: AL is supported by the Victorian Health Promotion Foundation (VicHealth) and The Cancer Council Victoria. MS is supported by a fellowship from the Victorian Health Promotion Foundation (VicHealth). At the time of preparing this paper MS was supported by a fellowship from the Victorian Health Promotion Foundation.
Linked Articles
- In this issue