Article Text

Abstract
Background There is increasing evidence that contact with other smokers, particularly in the family, is a strong determinant of risk of smoking uptake. A systematic review and meta-analysis of the magnitude of these effects is reported.
Methods Studies were identified by searching four databases to March 2009 and proceedings from international conferences. Meta-analyses were performed using random effects, with results presented as pooled ORs with 95% CIs.
Results 58 studies were included in the meta-analyses. The relative odds of uptake of smoking in children were increased significantly if at least one parent smoked (OR 1.72, 95% CI 1.59 to 1.86), more so by smoking by the mother (OR 2.19, 95% CI 1.73 to 2.79) than the father (OR 1.66, 95% CI 1.42 to 1.94), and if both parents smoked (OR 2.73, 95% CI 2.28 to 3.28). Smoking by a sibling increased the odds of smoking uptake by 2.30 (95% CI 1.85 to 2.86) and smoking by any household member by 1.92 (95% CI 1.70 to 2.16). After adjusting for overestimation of RRs it is estimated that, in England and Wales, around 17 000 young people take up smoking by the age of 15 each year as a consequence of exposure to household smoking.
Conclusions Parental and sibling smoking is a strong and significant determinant of the risk of smoking uptake by children and young people and, as such, is a major and entirely avoidable health risk. Children should be protected from exposure to smoking behaviour, especially by family members.
- Smoking uptake
- adolescence
- smoking
- systematic review
- meta-analysis
- tobacco and the lung
Statistics from Altmetric.com
Introduction
Approximately 1.1 billion people in the world are current smokers, and this figure is expected to rise to more than 1.6 billion by the year 2025.1 Since regular smoking results in a 50% likelihood of premature death and an average reduction of life expectancy by 10 years,2 smoking represents a massive public health problem. Tobacco smoke is powerfully addictive, so experimentation and uptake of smoking which, in developed countries typically occurs in late childhood or adolescence,3 is a highly hazardous behaviour. It is crucially important therefore to prevent exposure of young people to factors that increase their risk of smoking uptake.
Various risk factors have been shown to be associated with tobacco use in adolescents,4 ranging from individual to social and community and societal factors—including age, sex and socioeconomic status5; parental separation6 or family conflict7; and smoking among peer groups,8–10 in feature films11 and, perhaps most importantly, among family members.4 Smoking in the home is a recognised and entirely avoidable health hazard for children both before and after birth through passive exposure to smoke,12 however the influence of family smoking on the risk of smoking uptake and consequent future health of the individual is an aspect that to date has not be systematically reviewed and quantified.
In this paper we have reviewed the available world literature on the relation between smoking by family members and uptake of smoking among children and adolescents, and combined this information in meta-analyses to provide summary estimates of the magnitude of the effects of smoking by different family members. We have also used these estimates to calculate the number of children and young people in England and Wales who take up smoking each year as a result of smoking by others in their household. The work was carried out as part of a more extensive review of the effects of passive smoking in children for the Royal College of Physicians.13
Methods
Systematic review
We performed comprehensive searches of four databases (EMBASE, MEDLINE, PsycINFO and CAB Abstracts) from 2000 to March 2009 to identify all epidemiological studies assessing the association between smoking by children (2–12 years of age) and adolescents (13–19 years of age) and exposure to parental smoking (either parent, at least one parent, both parents), household smoking or sibling smoking (search strategies available by request). We also hand-searched conference proceedings from the Society for Research on Nicotine and Tobacco, the UK National Smoking Cessation Conference, the World Conference on Tobacco or Health from 2006 to 2009, as well as reference lists from identified relevant studies and previous narrative reviews. The systematic review was carried out in accordance with the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines.14
One author (MLJ) assessed the eligibility of studies from their titles and abstracts, excluding those that were not relevant. The full texts of eligible papers were assessed independently for eligibility by two authors (MLJ and JL-B) who extracted the data using a data extraction form. Disagreements were resolved through discussion.
No language restrictions were imposed during the searches, but papers written in languages other than English were excluded from the meta-analyses. The Newcastle Ottawa Scale15 was used to assess the quality of the included studies based on selection, comparability between exposure groups and ascertainment. The a priori chosen score of 7 was used to distinguish high from poorer quality studies.
Meta-analysis
Dichotomous data were extracted using raw values, crude ORs or adjusted ORs with 95% CIs. Adjusted ORs were used in preference where available. We performed meta-analyses using random effect models since the effect measures were expected to be heterogeneous. Exposure groupings (eg, any parent smoking) were defined empirically from those used in the studies. Heterogeneity between the studies was assessed using I2.16 Subgroup analyses based on quality (high vs poorer quality) and the definition of smoking status (current vs ever) were used to explore heterogeneity. Owing to disparate categories for the ages of the children and adolescents across the studies, subgroup analysis based on age at outcome was not feasible. Where extreme levels of heterogeneity were seen between the studies (I2 ≥90%), we performed sensitivity analyses to assess the effect of excluding outliers. We also restricted analyses to studies which adjusted for at least three of the following known confounders: age, gender, socioeconomic status, ethnicity, educational achievement, peer smoking and family structure. Publication bias was assessed using funnel plots. Analysis was performed using Review Manager 5.0.17 p Values <0.05 were considered statistically significant.
Population attributable fraction estimation
We estimated the proportion of children who live in a household in which at least one person smokes using data from the Health Survey for England,13 and used the formula p(OR − 1)/[p(OR − 1) + 1], in which p is the proportion of the cohort exposed to passive smoking and OR is the OR for smoking in children or adolescents where a member of the household smokes, to estimate the proportion of children whose smoking is attributable to household smoking exposure. We then used national smoking prevalence data for England and Wales to estimate the number of smokers by age 15 generated as a result of household exposure. Since ORs overestimate true RRs and this effect becomes increasingly relevant as the prevalence of the outcome increases, we also calculated the attributable risk using a lower RR based on an independent estimate that the magnitude of this likely overestimation is of the order of 15%.18
Results
Overview of included studies
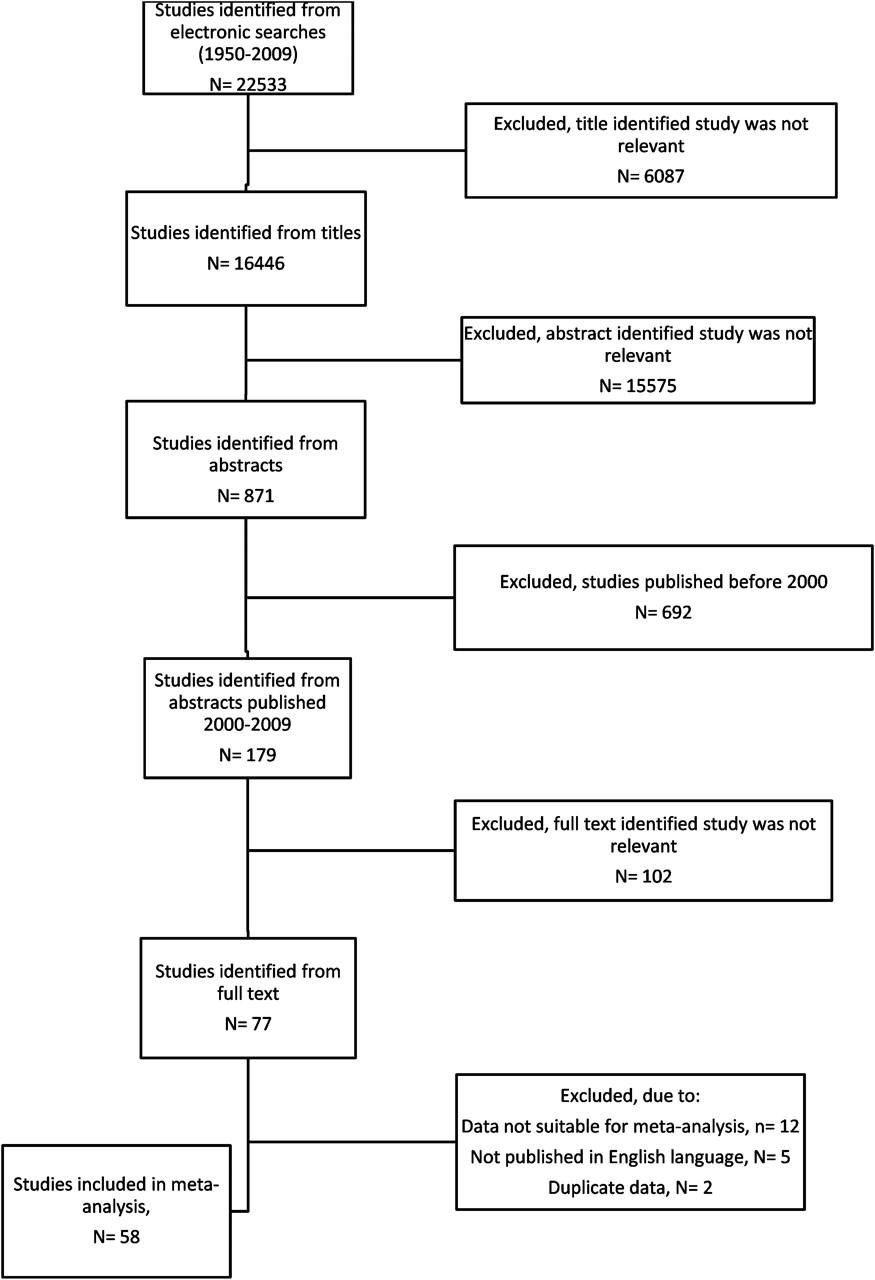
We identified 179 potentially eligible studies published between 2000 and 2009 and excluded 102 after screening the title and abstract. A further 19 studies were excluded from the meta-analyses because the data were not presented in a suitable format for meta-analysis,3 19–29 the same cohort was used in an already included study30 31 or they were published in a non-English language,32–36 leaving 58 studies included in the meta-analysis (table 1, figure 1).5 7 10 37–91 The majority of the studies were conducted in the USA or Europe and measured adolescent smoking status by self-reports, although two assessed cotinine in saliva.40 44 The majority of the included studies reported adjusted estimates, with only three reporting crude estimates.51 62 87 The quality of the studies ranged from 3 to 8, with a median score of 6.
Characteristics of the 58 included studies
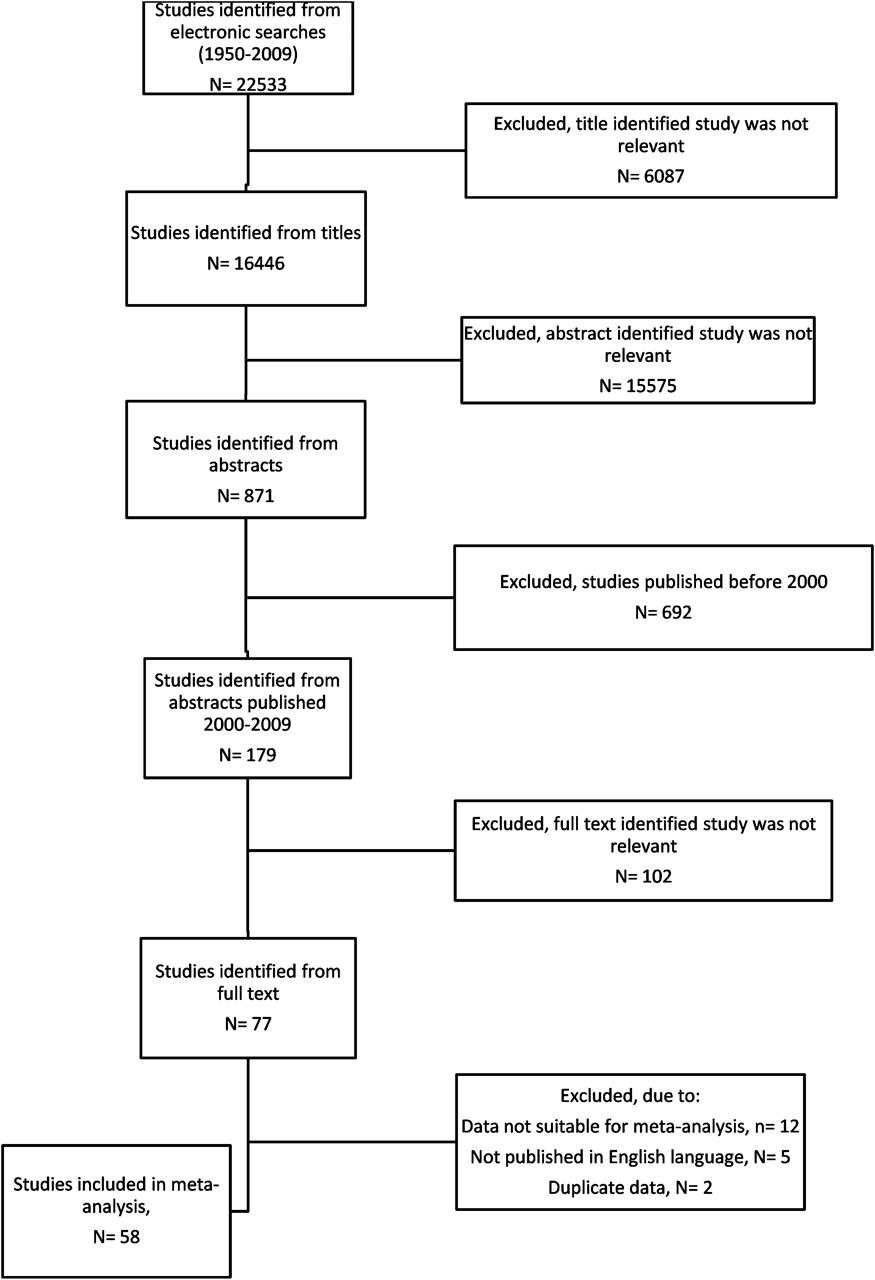
Flow chart of included studies.
Parental smoking
Exposure was determined by having one parent who smokes in 14 studies, of which a pooled analysis found that the risk of smoking in adolescence was increased by 62% (OR 1.62, 95% CI 1.49 to 1.76; see figure 5 in online supplement)10 38 40 42 47 48 65 71 76 78 83–86 which was independent of quality and the definition of smoking used. The effect was stronger for smoking by the mother (OR 2.19, 95% CI 1.73 to 2.79; 24 studies, I2=99%; figure 2)41 48 49 51 55 57 58 60–64 66 68 69 72 79 80 82 87–91 than the father (OR 1.66, 95% CI 1.42 to 1.94; 18 studies, I2=90%; figure 3).48 51 55 57 58 60–64 70 72 79 80 87–89 91 Subgroup analysis based on quality found higher magnitudes of effect for higher quality studies for smoking by the mother (higher quality, OR 2.35, 95% CI 1.56 to 3.53, 13 studies); conversely, lower quality studies had a higher pooled magnitude of effect for smoking by the father (low quality, OR 1.94, 95% CI 1.52 to 2.48, 7 studies) (tests for subgroup differences, p<0.0001 for both comparisons). Studies which defined smoking status in the adolescent as having ever tried smoking found stronger effects (mother, OR 2.76, 95% CI 1.58 to 4.82, 11 studies; father, OR 1.88, 95% CI 1.47 to 2.40, 11 studies) than those that used current smoking (mother, OR 1.64, 95% CI 1.36 to 1.96, 11 studies; father, OR 1.45, 95% CI 1.15 to 1.83, 6 studies) (test for subgroup differences, p<0.0001 for both comparisons). Sensitivity analyses where studies with outlier results were excluded had marginal effects on the pooled estimates for mother and father smoking. Additionally, sensitivity analyses restricted to studies which adjusted for at least three of the specified confounders had small effects on the pooled estimates for smoking by the mother (OR 2.25, 95% CI 1.66 to 3.05, 15 studies) and father (OR 1.52, 95% CI 1.32 to 1.76, 11 studies).

Mother smoking and the risk of adolescent smoking. Squares represent the estimate of effect and horizontal lines the 95% CIs from the individual studies. The centre of the diamond represents the pooled OR and the corner of the diamond the 95% CIs. ORs >1 indicate that exposure to mother smoking increases the risk of adolescent smoking.
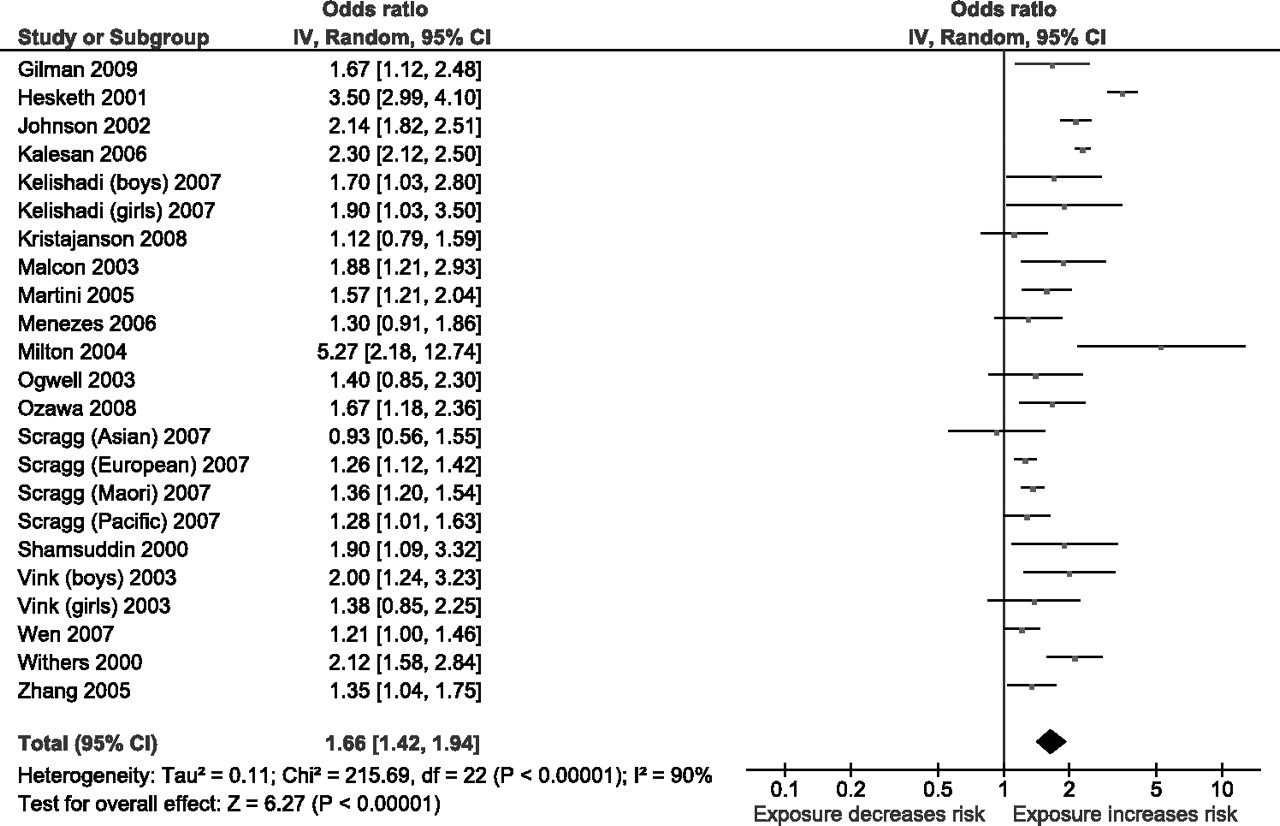
Father smoking and the risk of adolescent smoking. Squares represent the estimate of effect and horizontal lines the 95% CIs from the individual studies. The centre of the diamond represents the pooled OR and the corner of the diamond the 95% CIs. ORs >1 indicate that exposure to father smoking increases the risk of adolescent smoking.
Among children with at least one parent who smoked, the risk of smoking in the child was increased by 1.72 (95% CI 1.59 to 1.86; 10 studies, I2=23%, figure 6 in online supplement)7 39 44–46 53 54 56 74 75; if both parents smoked, the risk was increased almost threefold (pooled OR 2.73, 95% CI 2.28 to 3.28; 15 studies, I2=93%, figure 7 in online supplement).10 42 44 47 48 57 65 71–73 76 78 79 85 87 Subgroup analysis showed similar estimates for quality and for the definition used for smoking status. Sensitivity analyses where studies with outlier results were excluded reduced the pooled effects for both parents smoking (OR 2.16, 95% CI 1.88 to 2.48, I2=72%, excluded studies,42 57 Asian and European subgroups78 79). Additionally, sensitivity analyses restricted to studies which adjusted for at least three of the specified confounders had little effect on the pooled estimate for both parents smoking (OR 2.76, 95% CI 2.20 to 3.47, 11 studies).
Sibling smoking
A pooled analysis of 23 studies found that the effect of smoking by a sibling (usually defined within the included studies as an older sibling, with the remaining studies defining as any sibling) more than doubled the risk of an adolescent smoking (OR 2.30, 95% CI 1.85 to 2.86; 23 studies, I2=95%; figure 4).10 37 39 40 46 55 57–62 64 65 73 74 76 77 79 80 87–89 Subgroup analyses showed higher magnitudes of effect for poorer quality (OR 2.95, 95% CI 2.09 to 4.18) than for high quality studies (OR 1.87, 95% CI 1.62 to 2.17), and for studies assessing ever tried smoking (OR 2.60, 95% CI 1.95 to 3.46, 10 studies) (test for subgroup differences, p<0.0001 for both comparisons). Sensitivity analyses where studies with outlier results were excluded had marginal effects on the pooled estimate (OR 2.04, 95% CI 1.81 to 2.30, I2=77%, excluded studies57 59 64). Additionally, sensitivity analyses restricted to studies which adjusted for at least three of the specified confounder effect had similar marginal effects on the pooled estimate (OR 1.94, 95% CI 1.67 to 2.24, 12 studies).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sibling smoking and the risk of adolescent smoking. Squares represent the estimate of effect and horizontal lines the 95% CIs from the individual studies. The centre of the diamond represents the pooled OR and the corner of the diamond the 95% CIs. ORs >1 indicate that exposure to sibling smoking increases the risk of adolescent smoking.
Household smoking
Any household smoking (usually defined as either living with a smoker or that an adult smokes in the home) increased the risk by 1.92 (95% CI 1.70 to 2.16, 12 studies; I2=80%; figure 8 in online supplement).5 7 43 50 52 59 64 67 78–81 No significant differences in effect size were seen between the subgroup analyses for quality or definition for smoking status (test for subgroup differences, p=0.86 and p=0.17, respectively). Sensitivity analyses restricted to studies which adjusted for at least three of the specified confounders slightly reduced the pooled estimate (OR 1.69, 95% CI 1.54 to 1.87, 8 studies), but the effect remained highly statistically significant.
Publication bias
No evidence of publication bias was seen in the funnel plots for the relation between adolescent smoking and either parent smoking, both parents smoking, mother smoking, father smoking, and at least one parent smoking. However, there was some evidence of asymmetry in the funnel plot for sibling smoking and household smoking, where smaller sized studies showing protective effects on the risk of adolescent smoking seemed to be missing from the funnel plots (see figure 9 in online supplement).
Population attributable fraction
Health survey for England data indicate that, in 2007, around 22% of children aged up to 15 lived in a household in which someone smokes.13 Using the OR for household smoking (1.92) as the estimated RR of smoking in these children, the proportion of smoking uptake among children up to the age of 15 likely to be attributable to exposure to smoking in the home is estimated at 17%. In 2008 there were about 675 000 15-year-old adolescents in England and Wales,92 of whom 20% smoke93; a 17% attributable fraction translates into approximately 23 000 new smokers by age 15 arising from exposure to smoking in the home. Allowing for overestimation of the true RR from estimating pooled ORs,18 the adjusted estimate of RR is then approximately 1.67, the corrected population attributable fraction 13% and the estimated number of new smokers attributable to household exposure 17 000.
Discussion
This study uses systematic review and meta-analysis methods to provide summary estimates of the effect of living with a family member who smokes on the risk that a child or young person takes up smoking. The analyses confirm that smoking by siblings, parents or other household members—and particularly by parents—is a strong and significant influence on smoking uptake. The effect of individual family member smoking is strongest for smoking by the mother, but is stronger still when both parents smoke, with a near threefold increase in risk. We estimate that around 23 000 adolescents who are smoking regularly at the age of 15 in England and Wales are doing so as a consequence of exposure to household smoking. The consequences of smoking uptake in these individuals are likely to include significant morbidity and premature mortality, and also the financial poverty arising from a regular habit which, at 20 cigarettes per day at current UK prices, costs around £2000 per year. For those who commence smoking at younger age, these impacts are likely to be all the greater since early uptake of smoking is also associated with higher levels of tobacco dependence94 and heavier smoking.5
The great majority of the studies we assessed relied on self-reported smoking status which has been shown to be a good indicator of true smoking status in general, but may underestimate smoking in adolescents.95 This may result in underestimation of the observed effects and also contribute to some of the observed heterogeneity between studies. A limitation of this meta-analysis was that high levels of heterogeneity were observed for some comparisons, which suggests that there are unexplained reasons for variation in the findings between studies over and above chance which may result in potentially misleading summary estimates. We investigated the reasons for heterogeneity by performing subgroup analyses and sensitivity analyses; however, these analyses revealed relatively consistent findings. Generally, the pooled results did not differ appreciably between studies of different methodological quality or in relation to the definition of smoking status of the adolescent. ORs were higher, however, for studies that measured ever having tried smoking, consistent with the fact that a substantial proportion of children and young people experiment with smoking but do not become regular addicted smokers. We assessed the effects on smoking status in adolescence rather than attempting to assess the effect on the stage transitions of tobacco use—where adolescents can be labelled as ‘triers’, ‘experimenters’, ‘regular users’ and ‘dependent users’96—due to an insufficient number of studies being identified which categorised the stages of smoking. It is therefore difficult to determine at which stages the effects of parental and sibling smoking have more impact. Although inconsistent findings for a dose response association were seen in previous studies,97 we found strong evidence of this, where adolescents were at a greater risk of smoking when both parents smoked than when only one parent smoked. We also found that the magnitude of the effect was stronger when the mother smoked than when the father smoked. This finding appears to be more pronounced in recent years,97 and there was some evidence of a sex-specific effect where girls were influenced more by maternal than paternal smoking while the opposite applied to boys (data not shown). Further reasons for heterogeneity between the studies could be differences in approaches to adjustment for confounding; however, our sensitivity analyses restricted to studies which adjusted for multiple known confounding factors generally found the pooled results were very similar to the results from the unrestricted analyses. However, the pooled estimate for exposure to any household smoking was reduced from a pooled OR of 1.92 to 1.69, but the results remained highly statistically significant.
A limitation of our systematic review was that we excluded studies at the full text stage which were written in a non-English language, so the findings of the meta-analyses are biased towards English speaking countries. However, this exclusion criterion only resulted in five papers being excluded (conducted in France, the Netherlands, Slovakia, China and Austria), so the exclusion of these papers is unlikely to have a substantial impact on the conclusions of this study.
In the meta-analysis we estimated pooled ORs since 56 of the 58 included studies reported this measure of effect. Since smoking in adolescents is not rare, our estimated pooled ORs will overestimate the true RRs although, at an estimated 15%,18 the magnitude of this effect is small. Thus, allowing for overestimation of the true pooled estimate has marginal effects on the estimated strength of the association. Allowing for the overestimation in the calculation for the population attributable fraction results in an estimated 17 000 new smokers by age 15 arising from exposure to smoking in the home.
The importance of this study is that, irrespective of the true magnitude of these effects, it identifies a further and to date neglected third-party impact of smoking behaviour. The health risks to children and adults arising from passive smoke exposure are now well recognised and extensively documented,12 13 but arise directly and only from exposure to tobacco smoke. In this instance we identify an impact with the potential for substantial short- and long-term harm to health arising from the availability of cigarettes and/or the role model of smoking behaviour in the family. The number of children potentially affected is substantial, with around 2 million children in the UK living in a household that includes a smoker. This is a massive public health problem in its own right.
Effective measures to prevent smoking are well defined and promoted by the World Health Organization98 and include a range of policies that will help to reduce the prevalence of smoking in younger adults—and hence the typical parents of younger children—and thus reduce exposure to smoking behaviour. However, they do not yet address the need to ensure that children grow up in a home that is not only smoke-free—to protect them from the direct health consequences of passive smoking—but also free of smokers—to protect them from the adverse effects of smoking role models since observation of parental smoking behaviour can have profound influences on the perspectives of preschool children who view this behaviour as appropriate or normative in social situations.99 100 Preventing this latter effect will demand further radical changes in public policy and behaviour, and in the acceptability of smoking in places where children are present. Protection of children from this major cause of harm needs to become a high public health priority.
References
Supplementary materials
Footnotes
See Editorial, p 842
Linked article 154963.
Funding This work was supported by the UK Centre for Tobacco Control Studies (http://www.ukctcs.org) with core funding from the British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council and the Department of Health, under the auspices of the UK Clinical Research Collaboration; and by project grant C1512/A11160 from Cancer Research UK. The study sponsor had no role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.