Article Text

Statistics from Altmetric.com
Managed care organisations (MCOs) enjoy a history of promoting health through preventive services and health maintenance activities. In this unique capacity as healthcare providers, these organisations can effect healthy lifestyle changes in their member populations.
The single most important cause of premature death and preventable illness, in the United States today, is cigarette smoking.1 Most individuals who smoke express a desire to quit.2 Through the implementation of smoking cessation programmes, MCOs can play a major part in helping motivated individuals to join the ranks of quitters.
As part of the Robert Wood Johnson Foundation initiative, Addressing Tobacco in Managed Care, an annual survey of all managed healthcare plans is being conducted each year from 1997 to 2000. These surveys have the following objectives.
To assess the knowledge, attitudes and practices related to the Agency for Health Care Policy and Research (AHCPR) smoking cessation guideline3
To monitor the status of efforts to incorporate tobacco prevention and cessation interventions into routine care
To monitor the status of efforts to influence tobacco policies at the state, local or national level
To identify barriers faced by managed healthcare plans in their efforts to address tobacco control
To identify strategies used by managed healthcare plans to overcome barriers.
The results of the first annual survey are outlined here.
Methods
The survey was a mailed questionnaire with telephone follow up. The 32-item questionnaire was sent to all the health plans in the American Association of Health Plans’ (AAHP’s) database of member and non-member plans (n = 637). Of the 637 MCOs in the original sample, 95 plans (15%) were excluded, due to duplication in the sample, mergers or being inoperative, leaving 542 valid MCOs in the sample. A total of 323 plans replied, a response rate of 60%. The final results of the survey are based on these responses.
Results
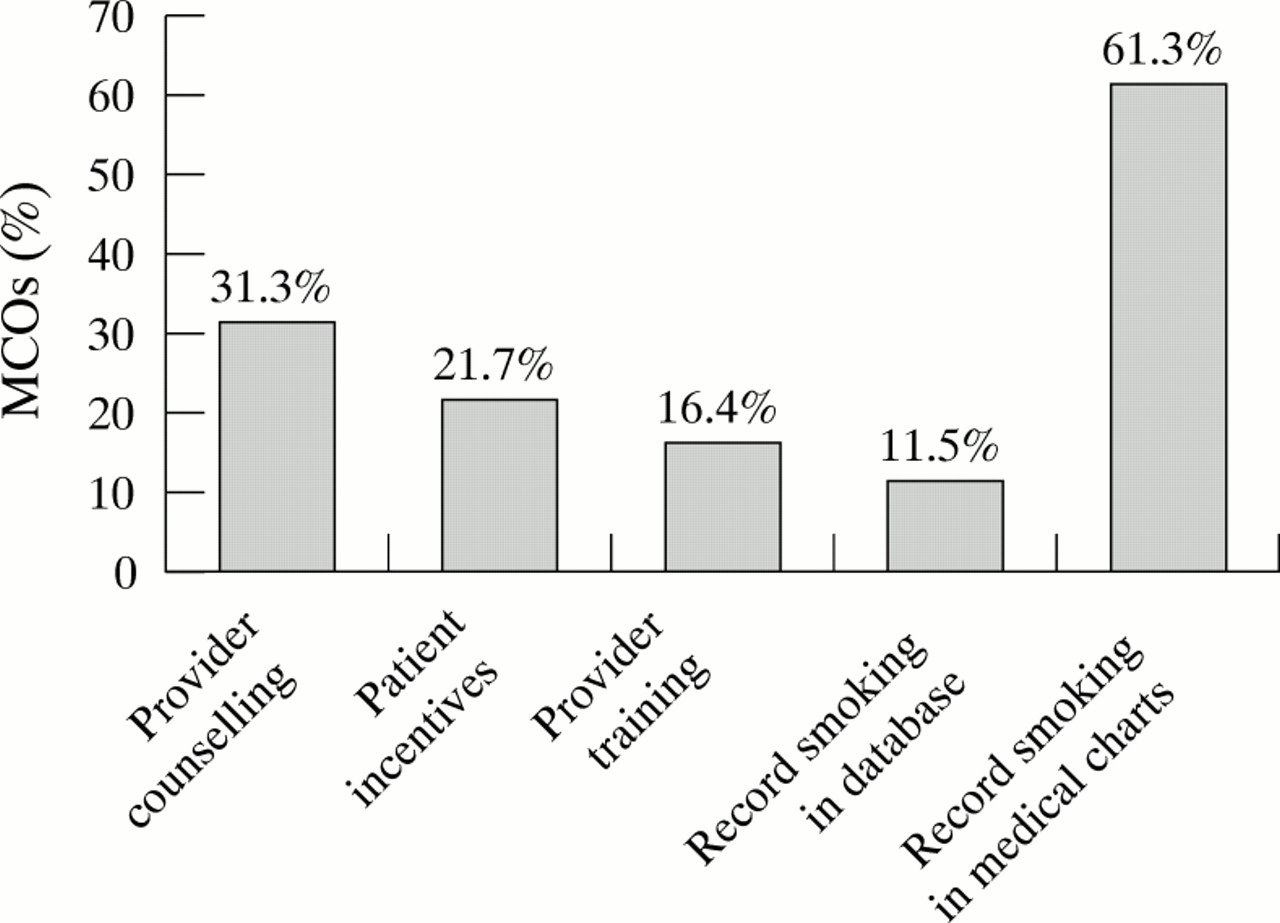
As stated earlier, the first objective was to determine the knowledge of, and practices related to, the AHCPR smoking cessation guideline. Over 71% of MCOs responding to the survey were aware of the guideline. Fifty-one per cent (164) of the MCOs had reviewed the guideline, and among those, 9% had fully implemented the recommendations, whereas 39% had partially implemented the recommendations (figure 1). There was substantial variation in the extent to which MCOs implemented specific practices and policies recommended in the guideline. Although most MCOs (61.3%) record smoking status in medical charts, few (11.5%) record smoking status in computerised databases.
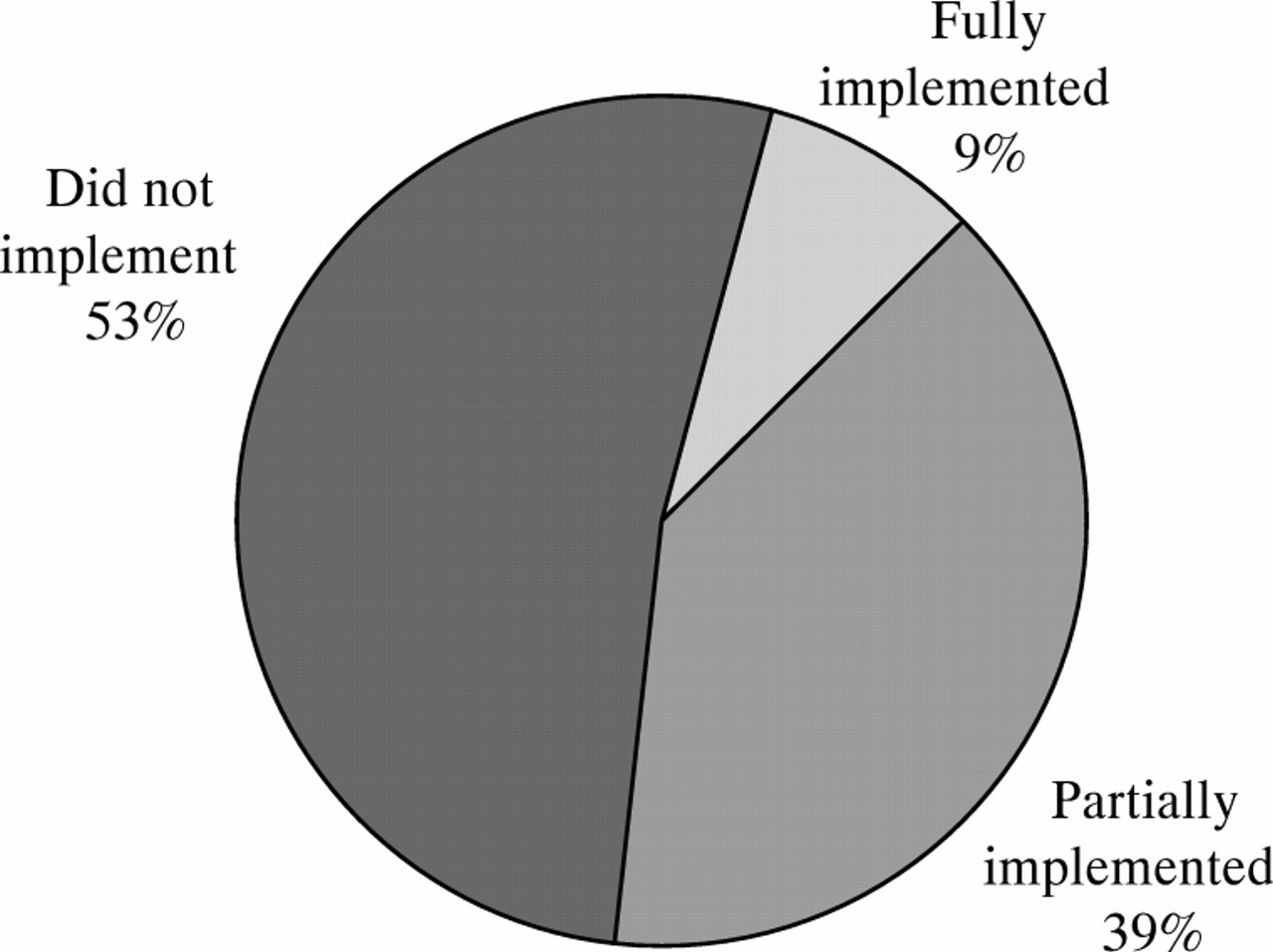
Implementation of AHCPR guideline reviewed by managed care organisations, among those who had reviewed the guideline (n = 164).
The survey was also designed to monitor the status of efforts to incorporate tobacco prevention and cessation interventions into routine care. Some MCOs offer provider counselling (31.3%), patient incentives (21.7%), and provider training (16.4%) as the means to reach this goal (figure 2).

Smoking cessation practices and policies implemented in managed care organisations (n = 323).
Over 67% of the responding MCOs had participated in tobacco prevention activities during the past year. These activities included: establishing policies for a smoke-free workplace (45.8%); participation in community-based activities (20.1%); use of media messages (15.2%); sponsorship of school-based programmes (14.6%); and involvement in legislative activities (13%).
Targeted cessation intervention strategies, aimed at specific population groups, were present in some of the organisations. Pregnant women were targeted as an intervention group by 45% of the organisations responding to the survey; patients with chronic illness by 22.6%; patients who had had a myocardial infarction by 21.7%; adolescent members by 17.6%; paediatric members by 15.8%; postpartum patients by 13.6%; and hospitalised patients by 11.5% of MCOs.
In terms of monitoring tobacco use among members, 25.1% of MCOs measured smoking prevalence, and 14.9% could identify individual smokers among their member populations. Sixty-two per cent had a budget for tobacco control activities. Of those MCOs with allocated funds, 12.4% had a part-time or fulltime tobacco programme coordinator.
Because providers are so important in effectively addressing tobacco use among members, the survey queried MCOs about barriers they perceived at the provider level. These barriers included: time constraints (57.3%); conflicting priorities (tobacco use was viewed as a relatively low priority agenda item) (42.7%); frustration with the low success (quit) rates (35.6%); and lack of reimbursement for cessation counselling (35.3%). MCOs implemented the following strategies to address some of the provider barriers: provider education (44.6%); use of prompts and reminders for providers (20.1%); increased reimbursement (3.7%); and use of incentives (2.5%).
Finally, there is a great deal of interest in monitoring the extent to which MCOs provide benefit coverage for smoking cessation treatments. Coverage for smoking cessation interventions was available in 244 (75%) of the MCOs that responded to the survey. Although full coverage was often provided for self-help materials (54.1%) and less frequently provided for smoking cessation classes (35.7%) and telephone counselling (32.8%), pharmaceutical treatments for tobacco addiction were rarely covered in full by MCOs (figure 3).
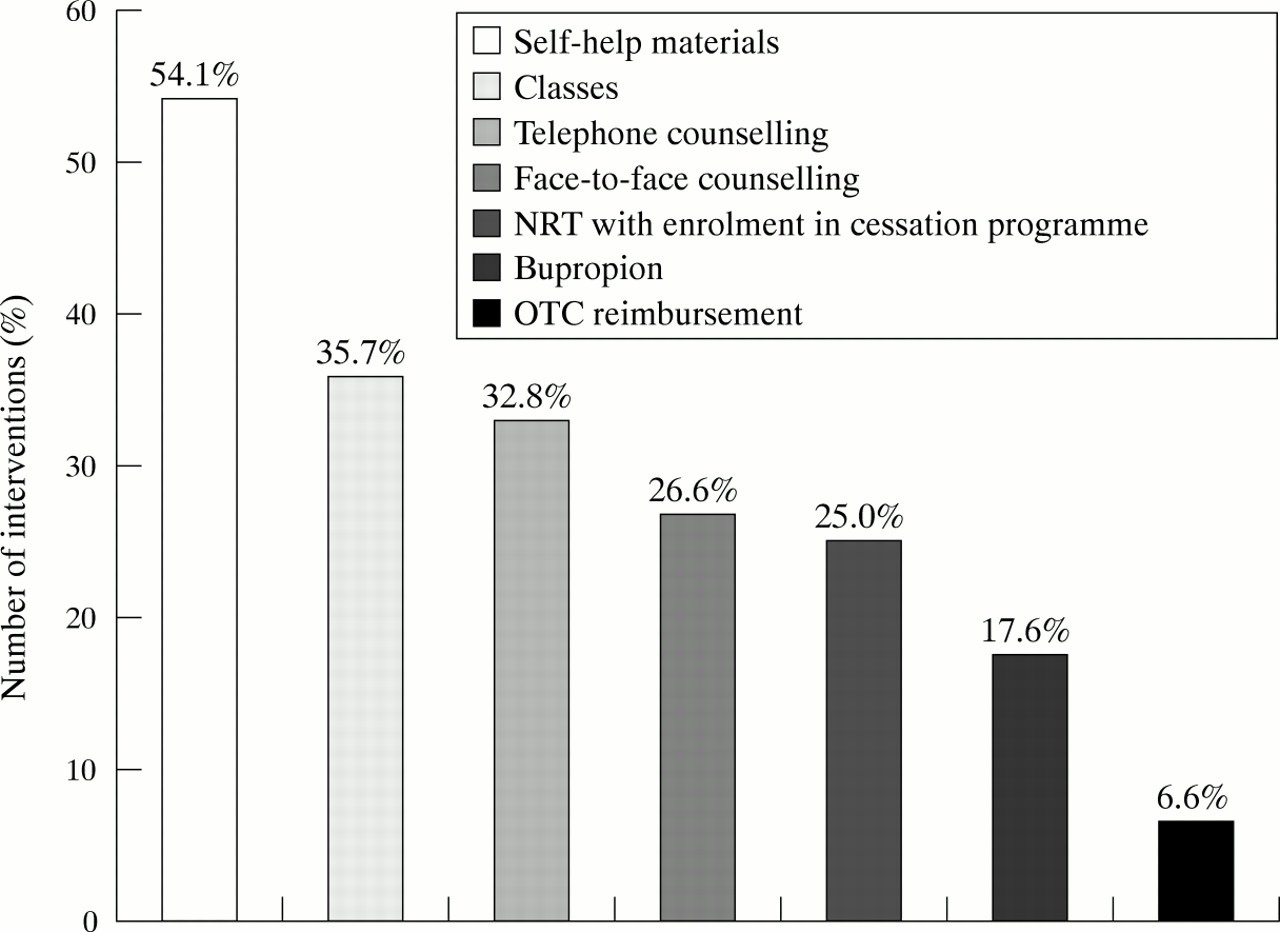
Smoking cessation interventions available with full benefit coverage (n = 244).
In addition to those MCOs that offer full coverage for various smoking cessation interventions, some offer partial coverage (figure 4). For example, whereas 35.7% of MCOs provide full coverage for smoking cessation classes, 20.5% provide partial coverage. Therefore, approximately 56% of MCOs provide some coverage for cessation classes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Smoking cessation interventions available with partial benefit coverage (n = 244).
Conclusions
The current state of smoking cessation interventions in managed care organisations leaves many opportunities for improvement. Among MCOs responding to the survey, 49% were unaware of the AHCPR smoking cessation guideline, and even among those that reviewed the guideline, only half have partially or fully implemented them. In addition, very few (14.9%) of the responding MCOs can identify individual smokers, which is a primary component of the guideline. Although a substantial proportion (44.9%) of MCOs cited strategies in place to address cessation during pregnancy, only 13.6% have programmes for postpartum patients. These are just a few of the areas with potential for improvement.
Managed care organisations are in a position to make powerful changes in the arena of tobacco control. There are many opportunities for increased success, such as the enhancement of systems to measure smoking prevalence, and the identification of individuals who smoke. Another important area is the barriers related to incentives and reimbursement. There is also a need for MCOs to increase their participation in community-based tobacco control activities. This is an exciting and challenging time for MCOs, particularly regarding tobacco control programmes. Managed care organisations should be in the forefront of the war against tobacco.
Acknowledgments
The author thanks Linda Schuessler for project management, Lisa Mahoney for assistance with data collection, Jennifer Peale for data analysis and Jeffrey Koplan for his invaluable input.