Cancer Prevention in Primary Care: Smoking and cancer: smoking cessation
BMJ 1994; 308 doi: https://doi.org/10.1136/bmj.308.6942.1478 (Published 04 June 1994) Cite this as: BMJ 1994;308:1478
- J Austoker,
- D Sandersa,
- G Fowler
- aCancer Research Campaign Primary Care Education Research Group, Department of Public Health and Primary Care, University of Oxford, Oxford OX2 6PE
- Department of Psychiatry, University of Oxford, Warneford Hospital, Oxford OX3 7JX
- Imperial Cancer Research Fund General Practice Research Group, Department of Public Health and Primary Care, University of Oxford, Oxford OX2 6PE
- Correspondence to: Dr
Smoking is the single most important cause of cancer. The risk of developing cancer is reduced by stopping smoking and decreases substantially after five years. Reduction in smoking must be central to any programme aimed seriously at the prevention of cancer. An individual approach, based in primary care, has the potential to bring about modest but important reductions in risk. Many randomised trials have shown the effectiveness of various smoking cessation interventions in primary care. Given resource limitations in primary care, individual effort should be focused on those at highest risk who are motivated to stop smoking. A population strategy has considerable advantages over the high risk approach as the potential for reducing morbidity and mortality in the whole population is much greater. The government must acknowledge its major responsibility; the outstanding example of its failure to do this is its persistent refusal to ban outright all forms of advertising and promotion of tobacco. There is clear evidence that a ban would contribute to a reduction in smoking prevalence and especially in the uptake of smoking by children.
Each year about 110 000 deaths in England alone are related to smoking, representing 17% of all deaths. Diseases caused by smoking include cardiovascular disease, respiratory diseases, and some cancers.
Smoking is the single most important cause of cancer, being significantly more important than all other causes. Many types of cancer are caused by tobacco. Approximately 30% of all deaths from cancer - that is, over 50 000 deaths from cancer a year - are attributable to tobacco smoking. This includes between 80% and 90% of deaths from lung cancer; a proportion of deaths from cancers of the oral cavity, bronchus, trachea, pharynx, larynx, oesophagus, and bladder; probably some deaths from cancer of the pancreas; and possibly some deaths from cancer of the kidney. To these, recent research suggests that we probably need to add a small proportion of deaths from leukaemia and from cancers of the nose, stomach, and cervix uteri.
Trends in smoking
The percentage of male cigarette smokers has decreased from 65% in 1948 to 29% in 1992, becoming a habit of the minority by 1973. The decrease for women has been less dramatic, from 41% to 28%, so that the difference between the percentage of men and women who smoke has been eliminated. Currently, around 14 million people smoke in the United Kingdom.
Age of smokers
Smoking is most common in men and women aged 20-24 and men aged 20-49. The percentages of smokers in all age groups have declined in the past decade, with bigger decreases being seen in the older age groups. In all age groups the decrease in the percentages of smokers among males is greater than that among females. Most adult smokers have acquired the habit by the time they are 19 years old.
The proportion of children who smoke regularly (defined as smoking at least one cigarette a week) increases with age. Few 11 and 12 year olds smoke, but by the age of 15, one in four children is a regular smoker. Of the regular smokers, 32% of boys and 26% of girls smoke over 71 cigarettes a week.
Children who smoke regularly are far more likely to smoke as adults, whereas non-smoking children are less likely to start smoking in adulthood. By the age of 19 years 30% of the population are smokers. The adolescent years are therefore extremely important in establishing a person's lifetime smoking or non-smoking pattern. Children are far more likely to smoke if other people at home smoke - brothers or sisters who smoke have more influence on their siblings beginning to smoke than has a parent who smokes. Surveys have also shown that children, unlike adults, prefer to smoke the most heavily advertised brands of cigarettes. The government receives an estimated pounds sterling 70 million per annum in tax on cigarettes sold illegally to children under the age of 16.
Social class, smoking, and lung cancer
Smoking is undoubtedly associated with the problems of poverty, unemployment, and other kinds of deprivation, but most smokers in the United Kingdom are light smokers (<20 cigarettes a day) and do not live in poverty. There is a strong reverse gradient between smoking and social class. Men and women in social class V are nearly four times more likely to be smokers than are those in social class I. Working class men are three times more likely to die of lung cancer than are those in middle class occupations. Among women death rates from lung cancer have increased in social classes IV and V and decreased in social classes I and II. There are also important geographical variations in smoking prevalence and mortality from lung cancer in the United Kingdom.
Type of tobacco
Tobacco is generally much more harmful when smoked as cigarettes than when smoked in pipes or cigars. Tobacco smoke is a weak carcinogen that causes cancer in a high proportion of smokers only after regular exposure for 30 to 40 years.
Type of cigarette smoked
In 1961 most smokers bought plain cigarettes (83% men, 64% women), but these percentages fell rapidly so that by 1981, 92% of men and 97% of women smoked filter cigarettes, which have lower tar and nicotine yields than plain cigarettes.
At the same time the tar, nicotine, and carbon monoxide yields of both plain and filter cigarettes have been substantially reduced. Between 1965 and 1988 the tar content of both plain and filter cigarettes was halved, nicotine yields fell by a third, and the carbon monoxide content was reduced by almost a quarter.
The evidence suggests that tar contains the carcinogens causing lung cancer. In 1992 almost no one smoked high tar cigarettes (defined since 1985 as >=18 mg tar/cigarette), and only 4% smoked middle tar cigarettes (15.0-17.9 mg) compared with 40% in 1986. Most smokers in every age group preferred “low to middle” tar cigarettes (10.0-14.9 mg). Nineteen per of men and 30% of women smoked low tar cigarettes (0-9.9 mg) in 1992.
Risk and life expectancy
The risk of lung cancer from smoking is summarised in box 1. The table shows the relative risk of lung cancer in relation to the number of cigarettes smoked. Smoking 10 cigarettes a day reduces life expectancy by an estimated 2-3 years, smoking 20 a day reduces it by 5-7 years, and smoking 40 a day reduces it by 8-10 years.
Box 1 - Risk of lung cancer from smoking1
Smoking cigarettes carries a much higher risk than smoking other forms of tobacco
Risk is directly related to the number of cigarettes smoked - that is, the higher the consumption the higher the risk
Risk is more dependent on duration of smoking than on consumption -for example, smoking one packet of cigarettes a day for 40 years is eight times more hazardous than smoking two packets a day for 20 years
Risk is reduced by ceasing to smoke - after 10 or more years of giving up smoking an ex-smoker has nearly the same risk as a non-smoker
Lower tar cigarettes appear to carry a lower risk of lung cancer than higher tar cigarettes
Relative risk of lung cancer in relation to number of cigarettes smoked2
Measures to reduce the risk of cancers produced by smoking
Reduction in smoking must be central to any programme aimed seriously at the prevention of cancer. A population strategy has considerable advantages over the high risk approach as the potential for reducing harm in the whole population is much greater. This approach uses effective measures such as price increases, control of tobacco promotion, enforcement of smoke free environments, and a national health promotion programme. The government strategy, as part of Health of the Nation, is to reduce both smoking prevalence and the consumption of tobacco among those who cannot stop smoking by focusing on all of these measures. Box 2 shows the targets for lung cancer and smoking in the Health of the Nation. Without effective controls on cigarette advertising and sponsorship, much of the focus of attempts to reduce cigarette smoking falls on individuals. A high risk approach, which targets the smoking behaviours of those at risk of health problems, is needed to complement the population based approach. Health professionals, in particular primary care teams, therefore have an increasingly important part to play in public education. The government strategy for smoking cessation includes:
Box 2 - Health of the Nation targets3
To reduce the death rate for lung cancer by at least 30% in men under 75and by 15% in women under 75 by 2010 (from 60 per 100 000 for men and 24.1 per 100 000 for women in 1990 to no more than 42 and 20.5 respectively) (baseline: 1990)
Lung cancer
To reduce the prevalence of cigarette smoking in men and women aged 16 and over to no more than 20% by the year 2000 (a reduction of at least 35% in men and 29% in women, from a prevalence in 1990 of 31% and 28% respectively)
In addition to the overall reduction in prevalence, at least a third of women smokers to stop smoking at the start of their pregnancy by the year 2000
To reduce the consumption of cigarettes by at least 40% by the year 2000 (from 98 bn manufactured cigarettes per year in 1990 to 59 bn)
To reduce smoking prevalence among 11-15 year olds by at least 33% by 1994 (from about 8% in 1988 to less than 6%)
Smoking reduction
Patients being asked routinely about their smoking habits - general practitioners are encouraged to record quantified information on their patients' smoking habits, which can then be aggregated in practice profiles
Increasing the number of smokers who receive advice about stopping smoking either opportunistically or in separate clinics when they visit their general practitioner
A high priority being given to the provision of advice on smoking and support for those wishing to stop
Many questions arise about how to increase the effectiveness of interventions to stop smoking.
Smoking cessation
Many randomised trials have evaluated various interventions in primary care for stopping smoking. These have mainly concentrated on general practitioners offering opportunistic advice during general consultations. The studies provide a wealth of information about interventions for use in general practice, but drawing definite conclusions about the effectiveness of different interventions is confounded by methodological differences between studies. A summary of potential interventions is given in box 3. When trying to help patients stop smoking, it should be remembered that not all smokers will be receptive to help at all times although many report that they want to stop.
Box 3 - Interventions in primary care for smoking cessation
Offering brief advice to stop smoking
Offering more intensive advice or counselling supplemented by written information and self help booklets
Offering nicotine replacement to reduce withdrawal symptoms
Offering patients follow up appointments specifically to discuss smoking
Advising patients that they will be asked about smoking at future appointments
Setting a date to stop smoking, including written contracts between patient and doctor to stop smoking by a set date
Showing the patients the physiological effects of smoking - for example,by showing carbon monoxide levels in expired air
Effectiveness of brief advice by general practitioners
The overall conclusion from several reviews of the literature is that brief advice from general practitioners during routine consultations is more effective than no advice in helping a few smokers to stop smoking and remain non-smokers for at least a year. For patients given brief advice cessation rates sustained for one year are about 5% compared with about 1% in non-intervention control groups. Although the rates at which people stop smoking after receiving brief advice seem to be low, the effects are magnified by the large number of contacts with the general population and the large number of general practitioners and must be compared with “background” cessation in the population. If all general practitioners gave brief advice to all their patients who smoked and achieved a permanent cessation rate of 5% an estimated half a million smokers would give up smoking each year in the United Kingdom.
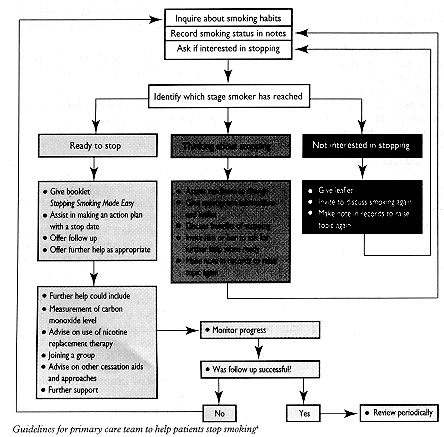
Brief advice is more effective when it emphasises the short term benefits of giving up rather than the long term dangers of smoking and when general practitioners follow a defined protocol. A simple protocol that can be integrated into daily practice increased the quantity, quality, and effectiveness of smoking cessation counselling by North American doctors. Further study is required to develop simple protocols for use in British practices. The figure shows an example of a protocol, based on the concept of readiness to change.
Long term cessation rates improve as more smoking education methods are used and when individual subjects are offered more help and support in giving up smoking. Using health education materials and self help booklets on smoking to supplement brief advice produces higher cessation rates. Advising smokers that they will be asked about smoking at subsequent visits also affects cessation rates.
The effectiveness of brief advice, with or without other interventions, is increased by offering smokers follow up appointments in which problems with giving up smoking can be discussed and the importance of stopping smoking can be reinforced. Follow up appointments could be provided by either the general practitioner or the practice nurse. Follow up appointments and support may well be most effective when targeted at smokers who do not have outside support from family or friends and at people whose partner smokes as these people are more likely to find stopping smoking difficult.

Guidelines for primary care team to help patients stop smoking4
{kind=link}
Sustaining cessation is an important part of programmes to stop smoking. The amount of support necessary to achieve it remains a research issue.
Nicotine replacement therapy as an adjunct to brief advice
Nicotine replacement therapy as an adjunct to offering brief advice and support has a role in general practice when used selectively by smokers who are motivated to stop and who are dependent on nicotine.
Two recent meta-analyses (systematic overviews), one of which was of 53 randomised trials in nearly 18 000 subjects, have shown that nicotine gum and patches are effective in helping motivated smokers to stop smoking. Overall, nicotine replacement therapy roughly doubles the cessation rate when compared with placebo. As with any intervention for stopping smoking, initial success is often associated with relapse, but a cessation rate of 10% or more sustained for a year or longer can be achieved in general practice, even by heavy smokers. The efficacy of nicotine gum, especially, increases with nicotine dependence: simple measures of this are cigarette consumption per day and smoking within half an hour of waking. In highly dependent smokers 4 mg gum seems to be the more effective form of nicotine replacement therapy. However, for average smokers, it has been calculated that for every 29 who use gum, and every 12 who use patches, one will achieve sustained cessation attributable to the use of these products.
We emphasise that all studies have included doctors, nurses, or other support as well as nicotine replacement therapy and that gum or patches are not an easy option or a medical or miracle cure. Box 4 gives guidelines for the use of nicotine replacement therapy.
Box 4 - Guidelines for use of nicotine replacement therapy
Use as an adjunct to brief advice and support
Encourage use in those showing evidence of nicotine dependence, the most discriminant indicators being time to the first cigarette after waking and the number of cigarettes smoked a day
Use with those motivated to stop smoking
Highly dependent smokers
Use nicotine gum (4 mg rather than 2 mg)
Give instructions on the use of gum
Use gum regularly rather than intermittently
Withdraw gradually after three months of use
Give continuing support
Less dependent smokers
Use nicotine patches
Use for up to three months
Begin with a higher dose and reduce at intervals
Give continuing support
Intensive versus brief intervention
Higher rates of stopping smoking are reported in studies using more intensive interventions than brief advice. A review of 28 major trials of advice from North American physicians to stop smoking found that cessation rates one year after brief advice were 3-13%, while those for more intensive interventions increased to 19-38%. A meta-analysis of trials of smoking cessation interventions in primary care concluded that the more intensive the intervention - that is, the more elements it contained - the more likely it was to be effective.
The fact that the more effective intensive interventions require more time has led to many arguments about whether to advocate intensive or brief interventions. Although intensive interventions are more effective, brief advice will probably have more impact on smoking rates because more general practitioners are likely to use brief rather than intensive interventions. The hypothesis however, that brief advice is better than intensive interventions because of greater use has never been tested: no clinical trials have been conducted relating the uptake of interventions in general practice to the intensity of the intervention. This has clear implications for the efficacy of different antismoking interventions in general practice and requires further investigation.
Methods of increasing smoking interventions in general practice
Regardless of the intensity of intervention, the rate at which general practitioners routinely discuss smoking has in the past been low: only 22% of smokers report that their general practitioner has advised them to stop smoking. Routinely advising smokers is not perceived as either rewarding or effective. Only 3% of general practitioners believe that they are successful in helping patients to stop smoking. There is no doubt that an intervention with a success rate of one in 20 does not produce immediate rewards or incentives for those trying to help patients stop smoking. Also for every successful intervention, many episodes of advice about stopping smoking will be met with at best disinterest and at worst active resentment from patients who either do not want or perceive it as too difficult to stop smoking. As a result, ways of motivating and helping doctors to be more active in smoking cessation interventions have been investigated. These include the need to consider the role of practice nurses and the potential effectiveness of other members of the primary care team.
Most general practitioners are currently seeking information about smoking status as part of the requirements for the new health promotion bands. As these bands also require information about interventions to be recorded, this provides an incentive for an increase in smoking cessation activities.
Various methods have been shown to increase general practitioners' participation in smoking interventions. Flagging patients' notes to remind the general practitioner to discuss smoking and having a defined protocol to follow increased not only the rate at which general practitioners discussed smoking but also cessation rates.
Several studies have investigated the effects of giving general practitioners training in how to help people stop smoking. Training is particularly important because counselling patients on healthy living is radically different from clinical training, where clear directive advice and instruction are important. Helping people change addictive behaviour entails appraising a person's readiness to change and, if motivated, what his or her particular difficulties are in stopping smoking and remaining an ex-smoker. General practitioners who had attended a six hour training workshop and had patient education materials available significantly increased the rates of antismoking interventions during routine consultations. The evidence strongly suggests that training and support increases motivation and the effective use of interventions, and the development of short, accessible training schemes for primary care staff, backed up by continuing support, should be a priority for primary health care facilitators and district health promotion departments.
Practice nurses
Studies on the impact of health checks are few, and the attendance rate of smokers at health checks is low. Evidence suggests that interventions by nurses may not be as effective as those by general practitioners but that nurse follow up and support can be a useful supplement to minimal advice from a doctor and when nicotine replacement therapy is used.
Clinics for stopping smoking
Clinics recruit only smokers who are highly motivated to stop; they are not relevant for most smokers, even those who say they want to stop. In specialist smoking cessation clinics a high success rate can be achieved with various interventions, including nicotine replacement therapy, but such results are unlikely to be relevant to the situation in general practice. Nevertheless, such clinics have a useful role for a few highly motivated people and are a source of education and support for other health professionals involved in smoking cessation activities, as well as a base for research.
Conclusion
Whereas it should be considered a priority to encourage primary care teams to engage in smoking cessation activities, it should be seen in the broader context of the action being undertaken by government. To achieve the targets in the Health of the Nation the government has set out a clear strategy for action on stopping smoking, focusing on price, health education, protecting non-smoking members of the public, and controls on tobacco advertising and promotion. Disappointingly, the last does not include a ban on tobacco advertising. The Smee report found a significant link between advertising bans and reduced tobacco consumption. The studies reviewed showed conclusively that “advertising does have a positive effect on consumption” and suggested sizeable and important effects of tobacco advertising bans. The results imply that an advertising ban would cut consumption in Britain by 6%. This would lead to the avoidance of many more premature deaths than the combined national breast and cervical screening programmes are likely to achieve. In addition, an outright ban would have a far greater effect than the small changes primary care teams are likely to achieve.
Without effective controls on cigarette advertising and sponsorship, it is difficult to provide the public with a consistent antismoking message. Therefore opportunities for effective ways of helping people to stop smoking should be given full encouragement and support. Health professionals undoubtedly have a crucial part to play in this process. Overall, much of the research on interventions in primary care for stopping smoking, has already been done, the main conclusions being summarised in box 5. Implementing the findings is the problem. The relevant health professionals need to be targeted to increase their motivation in order to find ways of making the recommendations work in practice.
Box 5 - Smoking cessation in primary care: summary
Brief advice from a general practitioner is better than no advice
Nicotine replacement therapy is effective as an adjunct to brief advice in motivated smokers with nicotine dependence
Intensive interventions are more effective than brief advice but are less likely to be implemented
One to one contact is better than working in groups
One to one contact can be followed by working in groups if subject is motivated
An initial intervention by a general practitioner could be followed up by intervention by a practice nurse
Training may improve the effectiveness of general practitioners and other members of the primary care team
Simple protocols should be developed
Availability of health education literature significantly increases rates of antismoking interventions
Effectiveness can be increased by: - Assessing whether the person is motivated - Emphasising the short term advantages of giving up smoking -Offering nicotine substitutes to targeted people with nicotine dependence -Setting a target date to give up - Making health education literature available - Arranging follow up appointments (more attention, more support)
Acknowledgments
A complete list of references can be obtained from JA.