Article Text

Abstract
Telephone based tobacco cessation services, or quitlines, have become central components of many comprehensive tobacco control programmes. This paper provides an overview of their history, noting milestones in the growth of quitlines. Key factors in their worldwide adoption were solid evidence from clinical trials with large community samples and strong backing from public health officials. Quitlines are now available throughout most of North America, Europe, Australia and in many other locations around the world. The paper also offers several recommendations for future directions in quitline practice and research. Benchmarks should be established for key areas of quitline implementation, such as accessibility, quality and cost efficiency. Advances in pharmacotherapy, telephony and web based applications should be investigated for opportunities to expand service offerings. Research and development are needed to determine how best to serve a diverse clientele in the most cost effective manner. Funding should be expanded and diversified to enable quitlines to serve much larger numbers of users. Healthcare providers should be targeted for quitline promotion, to engage them in a broad effort to increase the number of patients receiving cessation messages from clinicians. The goal of quitline promotion should expand to include an increase in unaided quit attempts in the population. Early research findings were quickly adopted in quitline practice, and future research to answer questions that have arisen through the implementation of quitlines will probably also find quick adoption.
- tobacco cessation
- quitlines
- cessation policy
Statistics from Altmetric.com
A prominent recent development in tobacco control is the worldwide proliferation of telephone based tobacco cessation programmes, commonly referred to as quitlines.1–8 Most such programmes are government funded and free of charge to callers. They are best known for providing behavioural counselling to help callers develop and follow a plan to quit smoking, but may also offer self help cessation literature, referral to local treatment programmes and, in some cases, low or no cost pharmacotherapeutic cessation aids.1 7
There are many reasons quitlines have been so widely adopted. They are an efficient means of delivering evidence based treatment to large numbers of tobacco users.3 They are easy to promote and meet with broad acceptance by the public.2 They eliminate barriers to access, such as lack of transportation, child care challenges, and inability to pay for treatment.9 They can help to reduce tobacco related health disparities by reaching people underserved by more traditional programmes.10 For these and other reasons, quitlines have been assigned a central role in many government sponsored tobacco cessation campaigns, and serve as key components of comprehensive tobacco control programmes.11
This paper provides an overview of the development of quitlines to date, and offers several recommendations for future practice and research, focusing in particular on ways to increase the population impact of quitlines.
LOOKING BACK
Milestones in the development of quitlines
For many years, the telephone has been a medium for helping tobacco users quit. In the early 1980s, a toll-free cancer hotline in the United States, the Cancer Information Service, found that many callers wanted information on quitting smoking, and responded by providing the first telephone based cessation service.12 13 Limited in the depth and intensity of assistance provided, and not formally tested for efficacy, the service nevertheless demonstrated a demand for telephone counselling for tobacco cessation. In 1985 and 1988, call-in services were established in the Australian state of Victoria and in England, respectively.7 14 Quit Victoria and UK Quit were the first broadly accessible telephone lines dedicated exclusively to helping smokers quit, and had roles in the later development of quitlines in Australia and Europe. In 1992, the California Department of Health Services established the first publicly funded quitline using a counselling protocol that had been proved to be efficacious in a clinical trial.15 The California smokers’ helpline has been in continuous operation ever since. Also in 1992, Group Health Cooperative, a health plan based in Seattle, Washington, USA, implemented a private quitline for its members, using another validated protocol.16 It would later become Free & Clear, Inc, the quitline operator for numerous states and private companies. Over the remainder of the decade, quitlines were established in several parts of the United States, Australia and Europe.7 Then in the 2000s a period of very rapid growth ensued, with quitlines suddenly becoming prevalent across North America, Europe, Australia and New Zealand. There are now scores of publicly supported quitlines around the world. They exist in all states and provinces of the United States, Canada and Australia, in most European countries, and in several other parts of the world. Figure 1 shows a world map indicating where quitlines are currently available.
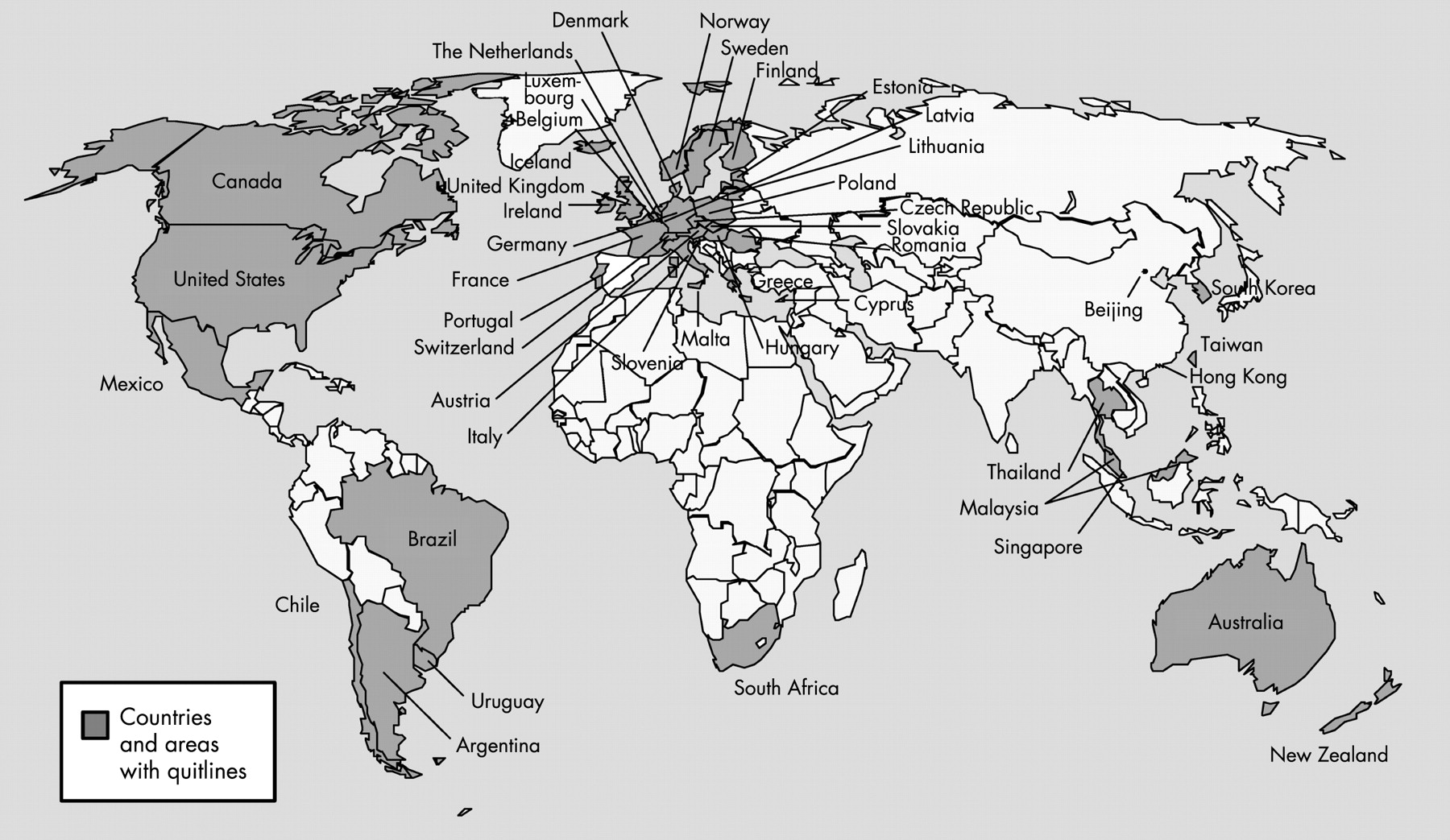
{kind=link}
Training conferences and other information sharing activities helped foster the proliferation of quitlines. In response to frequent requests for technical assistance on setting up a quitline, the California Department of Health Services and the American Cancer Society in 1998 hosted an international quitline training conference in San Diego. In 1999, UK Quit hosted a similar event in London, in response to a corresponding need in Europe. Participants formed the European Network of Quitlines to facilitate the exchange of information on quitlines among member nations. The network has been active ever since and has facilitated several international meetings. In 2002, North Americans held a conference in Phoenix, Arizona, bringing together quitline operators, researchers and funders from across the United States and Canada, as well as delegates from state health departments that had not yet established quitlines. Discussions at that conference led to the launch of the North American Quitline Consortium in 2003. Public health officials from Asia and Latin America also attended some of these meetings, and quitlines have recently been established in those parts of the world as well. As this paper goes to press, Taiwan, one of the early adopters of quitlines in Asia, is hosting a training conference for that region.
In 2003, the US Department of Health and Human Services published its national action plan for tobacco cessation.17 This ambitious plan urged creation of a national network of quitlines to provide universal access to effective tobacco cessation treatment, along with a federal tobacco tax increase of $2 per pack, in part to support the promotion and operation of quitlines. The tax increase has not been enacted, but the federal government has established a national toll-free “portal” to statewide quitlines and has modestly augmented states’ budgets for quitlines. The portal, 1-800-QUIT-NOW, began operation in November 2004, routing English speaking callers directly to their state quitlines.
A strong evidence base
Randomised, controlled trials demonstrating the efficacy of quitlines facilitated their widespread adoption.15 16 18–20 Several meta-analytical reviews have summarised these studies.21-24 Many of the studies showing efficacy had large and diverse community samples, suggesting the broad appeal of quitlines and creating confidence in the generalisability of their results. Some of the more recent trials were directly embedded into the ongoing, real world operations of quitline services.18 20 25 26
Controlled trials have shown that telephone counselling for tobacco cessation can significantly increase the long term quitting success of adult smokers who take the initiative to call.21 24 Research has also found a dose-response relation between telephone counselling and long term abstinence, with a single session of counselling producing better outcomes than no counselling, and multiple sessions producing outcomes that are better still.15 The strongest evidence to date has been for multisession, proactive protocols, in which a counsellor initiates all calls except for the tobacco user’s first call to the quitline.24
Leadership from public health officials
Notwithstanding the strength of the scientific evidence for quitlines, their adoption into practice was not guaranteed. Behavioural research often ends with the publication of findings rather than the quick translation of those findings into practice.27 28 Even new drugs found to be effective in clinical trials generally require intense promotional efforts to gain recognition. Mounting such a promotional campaign can be expensive, and may occur only when there is a significant potential for profit. Perhaps for this reason, awareness within the medical field of effective behavioural treatments tends to be limited. This may explain why quitlines escaped the notice of the medical establishment until quite recently.29 30
Quitlines owe their quick adoption in the United States and elsewhere to key figures in public health. In the early 1990s, officials in the California Department of Health Services were quick to appreciate not only that a statewide quitline could provide an effective clinical service, but that its promotion could support the broader campaign to change social norms around tobacco use. Officials in the Massachusetts Department of Public Health realised that a quitline could serve as the hub of an integrated network of cessation services, and that it could be used to unite all of the state’s health plans and healthcare systems behind the common goal of addressing tobacco in healthcare settings.31 Officials in the Arizona Department of Health Services recognised that the expertise of a quitline operator could be tapped to train health educators throughout the state on tobacco cessation. Through their embrace of the scientific evidence and the innovation with which they approached the development of their own programmes, such early adopters created useful models for later quitlines.
LOOKING AHEAD
As operators of one of the oldest evidence based quitlines, and close observers of the development of quitlines around the world, we offer several recommendations on future directions. These reflect our priorities for the field, but are not meant to be exhaustive. For another perspective on some of these issues, readers may wish to read the paper by Borland and Segan.32
The recommendations that we outline in this paper address, firstly, the need to consolidate recent gains in the development of quitlines by focusing on quality, through the establishment of benchmarks for quitline implementation. We then suggest ways to increase the range of services offered and the range of users served. Finally, we highlight opportunities to increase the population impact of quitlines, by increasing and diversifying their funding, engaging healthcare providers in their promotion, and leveraging the availability of quitlines to produce both aided and unaided quit attempts in the population. We highlight areas where research is needed.
Establishing benchmarks
Most current quitlines are no more than a few years old. With trade organisations facilitating information sharing among them, and with competition for quitline contracts keen in some parts of the world, it is perhaps inevitable that benchmarks for key areas of quitline implementation will emerge, and will then rise over time. These fluid standards have the potential to drive a continuing improvement in quitline quality.
A basic premise of quitlines is that they are highly accessible, yet commonly accepted standards addressing just how accessible they should be do not exist. There is no consensus on how many hours per week a quitline should be open, on the percentage of tobacco users who should be able to access it in their preferred language or on how low the literacy level of programme materials should be to meet the needs of the quitline’s target population, though each of these factors has a bearing on the accessibility of services. Benchmarks addressing such factors would help to eliminate or reduce barriers to treatment.
Standards are also needed to gauge the quality of the service itself, though quality is more difficult to measure than accessibility. Appropriate elements for benchmarking include the percentage of incoming calls answered by live agents during operating hours, the percentage of new registrants who agree to receive counselling, the percentage of those opting for counselling who actually receive it, the percentage of counselled clients setting a quit date and the number, length and timeliness of counselling sessions. Benchmarks for counsellor training and continuing education would be helpful, as they affect the quality of services provided. Standards for the percentage of counselled clients making a serious quit attempt and successfully quitting would also be useful, although these outcomes must be interpreted in context, as population differences can account for some of the difference in outcomes among treatment providers.11
Other indicators of the effectiveness or cost efficiency of quitline promotion and operation could also benefit from benchmarking, such as the degree to which the population using the quitline is ethnically representative of the tobacco users in the quitline’s service area, the amount of promotional money spent per registered caller, the percentage of calls generated by healthcare provider referrals or other word of mouth and the amount of operational money spent per registered caller or per person counselled. Such considerations are vital, as tobacco control programmes strive to obtain the maximum decrease in tobacco use with limited resources.
Expanding the menu of service offerings
In a trend that seems likely to continue, many quitlines have expanded their menus of offerings beyond the core services of counselling, printed materials, and referral.1 Many quitlines now provide free or discounted nicotine patches. Providing callers with medication in addition to behavioural counselling can significantly increase quit rates.25 33 Given that quitlines sometimes provide less than the full regimen of pharmacotherapy (for example, a two weeks’ supply of nicotine patches), because of cost considerations, research establishing the most cost effective dosing for quitline callers would be helpful. It has also been shown that patch give-aways can outperform media campaigns in driving large numbers of callers to a quitline, at least in the short term.34 35 However, considering only the number of calls generated creates a risk of overlooking other possible benefits of media promotions. Research investigating whether, over the long term, there are differences in population impact between these two promotional methods would be useful. There is also a concern that give-aways simply transfer the cost of quitting aids from health plans or individuals to the quitline. Careful research to help elucidate all of the costs and benefits of the provision of pharmacotherapy through quitlines is needed.
Telephony is another area in which the menu of service offerings may continue growing. Some quitlines, such as Rokeninfo-Lijn in the Netherlands, have long offered the option of listening to recorded messages about quitting. Other possibilities are text messaging,36 automated reminder calls and a range of opportunities associated with interactive voice response. Quitlines may also experiment with video telephony, either for two-way video conversations or for transmitting video clips and other visual information. Telecommunications technology changes rapidly, and new opportunities for intervention arise whenever a new technology gains acceptance. Embracing these changes could help quitlines to serve more people, and to do so more cost efficiently. It could also help them reach younger tobacco users. Evaluation of these new services using experimental designs where feasible would be helpful to the field as it considers how best to keep pace with developing technology. Such evaluation should address either the efficacy of these services per se, or the effect they may have on the use of other validated services (for example, by appealing to new groups of users or by decreasing attrition).
The integration of telephone counselling with web assisted tobacco interventions is another promising area for expansion. Conceivably, some of the content of telephone counselling sessions could be transferred to an online format. Quitline users could visit an online site to post information about their progress and receive automated feedback or a callback from their counsellor. While so far there is insufficient experimental evidence for tobacco control programmes to rely heavily on the use of online services, they have the potential to reach large numbers of tobacco users at comparatively little cost.37 38 Therefore, the value of future research findings indicating the efficacy of such services, either alone or in combination with telephone counselling, is difficult to overstate.
Adapting protocols to the range of quitline users
For certain groups of quitline callers, specialised counselling protocols may be needed. Identifying these groups and developing protocols to serve them are activities that command much attention from quitline funders and operators. Each language group to be served by a quitline needs a protocol in its own language, though researchers have so far published evidence of efficacy only for callers who speak English and Spanish.24 Chewing tobacco users, adolescents, pregnant smokers and those with serious mental health conditions are other groups that require specialisation, because of important differences from other quitline users. There is some evidence of efficacy for tobacco chewers,39–41 but more evidence is needed to support the use of specialised protocols for other groups.42–46 More definitive studies with these populations are clearly needed.
In a second category are callers who can be grouped demographically, but for whom the appropriateness of specialised protocols is unclear. Protocols selected on the basis of ethnicity alone run the risk of stereotyping callers, because there may be as many important differences within ethnic groups as between them. The same may be said about socioeconomic status, education, age (among adults), sex and sexual orientation. To our knowledge, a coherent system for determining when specialisation is appropriate has not been proposed. A good starting point would be the idea that all members of a group should share one or more distinct characteristics that have a bearing on quitting success, in order to be considered for development of a specialised protocol. Determining what those characteristics are, what the appropriate protocol modifications are and whether the resulting protocols are efficacious will require thoughtful development and testing.
For a third category of callers, many quitlines do not have formal protocols, though they would clearly be useful. This category includes tobacco users who do not want to complete an intake call, former quitline users who call back after relapsing, non-smokers who call on behalf of a friend or family member and healthcare providers and other professionals who are trying to decide whether to make referrals. Studies have not shown whether assisting these callers leads to increased quitting, but from a customer service standpoint it is not really possible to do otherwise. Such calls may go unreported because they are “off protocol,” though they represent a significant portion of the total call volume. It would be helpful to the field if efforts were made to describe and evaluate some of the approaches taken with these callers, so that a more complete picture of how quitlines are actually used would emerge. Such an effort may highlight opportunities that have not yet been fully realised. For example, a quitline might use its experience with repeat callers to develop a campaign to proactively re-enrol former participants in the service.
A fourth category of callers to be considered for adapted protocols consists of tobacco users who may need less help than most other callers. Many quitlines receive large number of calls and are generally underfunded in the sense that they do not have enough resources to provide comprehensive counselling to everyone who calls. This may mean that they must choose between providing multiple sessions to a smaller number of callers, providing a single session to a larger number, or some combination of the two, using procedures that match the intensity of treatment to the needs of each caller. There are known factors that predict relapse,47 and quitlines may design protocols that are adapted to the varying levels of risk. Those with multiple risk factors would receive comprehensive cessation counselling, while callers with few or no risk factors would receive a briefer service. This has the potential to achieve greater cost efficiency than providing the same comprehensive service to all callers regardless of need. Such an approach would need to be carefully evaluated to ensure that treatment decisions are made appropriately, and that the goal of maximising the quitline’s overall impact on quitting is met.48
Funding the continued growth of quitlines
Governments are increasingly aware of the importance of providing effective treatment for tobacco dependence, as the proliferation of publicly supported quitlines has shown. Yet most spend very little on direct provision of cessation services, even when there is a seemingly logical funding source, such as tobacco taxes or revenues from the Master Settlement Agreement.30 49 Consequently, quitlines reach only a small fraction of the target population each year. For example, US quitlines serve about 1% of the tobacco users in their respective states per year, on average.1 They will need to serve a much larger proportion of tobacco users to have an appreciable population impact.50 In comparison, the national action plan sets a target of 16% of the nation’s tobacco users receiving quitline services each year. It has been estimated that a national effort of this magnitude could result in approximately one million tobacco users quitting annually.17 Such a commitment from the federal government would have a dramatic, positive effect on the nation’s public health, and would generate significant savings for federal health insurance programmes, despite the initial cost.17 Until such an effort is implemented, states should continue to fund their tobacco control programmes, including quitlines, as aggressively as possible. Research in the United States has shown that quitline utilisation is positively correlated with the level of funding.1
The private sector could do more to support quitline services. The fact that many health plans and employers have the resources to cover effective tobacco cessation medications suggests that they can also cover evidence based behavioural treatments, and some of them already do provide quitline services to their members and employees. With telephone counselling, as with nicotine replacement therapy, a positive return on investment can be demonstrated.51 52 Yet few quitlines receive any support from the private sector.1 Commercial quitline operators such as Free and Clear, Inc, who may be more accustomed than public health officials to making the business case for tobacco cessation, have shown it is possible to market quitline services to corporations and health plans.
Cost sharing between the public and private sectors may be a practical and reasonable way to increase quitline funding. Public funds could be used to establish a basic quitline infrastructure, to promote it, and to pay for service for the uninsured and publicly insured, while health plans or employers pay the cost of their members’ or employees’ services. Reports of such innovative quitline funding mechanisms that successfully leverage a public investment to obtain participation by the private sector would be very useful to the field.
Engaging healthcare providers in promoting quitlines
With or without a funding relationship, many health systems and healthcare providers have become solid partners with quitlines, and refer patients regularly. Courting referrals from healthcare providers makes sense; it has been reported in the United States that they see about 70% of tobacco users each year, often in circumstances that create a “teachable moment” concerning the need to quit.53 54 By giving providers a place to send their patients for effective cessation treatment, quitlines make it more likely that providers will ask all patients whether they use tobacco and advise the ones who do to quit.4 Clinicians’ advice is itself an effective intervention which, if applied on a population level, would dramatically decrease the prevalence of tobacco use.22
Some healthcare providers may be more willing to refer to quitlines under a proactive enrolment model, in which the names and telephone numbers of patients agreeing to be contacted by a counsellor are forwarded to the quitline. This approach helps patients over the threshold of ambivalence about seeking help to quit, and gives clinicians greater confidence that their patients will follow through with the intended treatment. It has been tried in several settings and is clearly feasible.55 56 It can dramatically increase the use of quitline services among referred patients, by a factor of 10 or more, relative to simply telling patients to call the quitline on their own.55 56 The question of whether quitline services are as effective for tobacco users enrolled in this manner as for those who call on their own has not been answered, and should be researched. If proved to be effective and broadly implemented, this approach could have an enormous effect on quitline utilisation.
All of the healthcare professions are credible sources of information on health and tobacco, and patients may need to hear from more than one of them before deciding to quit. For any given patient, it is difficult to predict which clinician will tip the decisional balance in favour of cessation. Increased efforts to promote quitlines through all healthcare systems and all providers could lead not only to increased quitline utilisation, but also to increased quitting in the population, amplifying the effect of a quitline working alone.
Promoting both aided and unaided quit attempts
The notion that a quitline could have a population impact beyond what it achieves through the provision of direct service becomes clearer when one considers quitline promotion separately from the service itself. Just as the promotion of quitlines in healthcare settings may induce providers to intervene with their patients who smoke (and to refer some of them to quitlines), it may also have a beneficial effect on the behaviour of others in the community.
For tobacco users themselves, quitline promotion has the potential to motivate not only calls to the quitline, but also attempts to quit—with or without service. Advertising a quitline conveys to tobacco users that help is available for those who want it, that it is being used and that other tobacco users must therefore be choosing to quit. Thus, advertising a quitline helps to establish a norm of quitting. Under the influence of such messaging, many tobacco users who do not feel they need help themselves, or who are not sure they want it, may try to quit on their own. Though only a small percentage are likely to succeed in that attempt, if the number trying is large, the number succeeding will also be large.57 If they are encouraged to attempt quitting more often, successful quit attempts will also occur more often. Promoting quit attempts that are aided by a quitline may therefore leverage additional unaided quit attempts in the population. There is some evidence that quitline promotion can significantly increase success in unaided quit attempts,19 but more research substantiating this effect would be very helpful to those who plan media and other promotional strategies. Since the goal of a cessation campaign is to reduce the prevalence of tobacco use across the whole population, not just among those who receive services, the potential of quitline promotion to increase both aided and unaided quit attempts should be fully exploited.57
Quitline promotion can have a positive effect on non-smokers in the community, as well. It has been shown that quitline referrals increase when advertising increases.58 Quitline promotion appears to motivate friends, family and others to encourage tobacco users to quit.59 This suggests that quitlines can increase their population impact by enlisting community members in actively promoting quitting among the general tobacco using population. Deliberate efforts to enlist such support are likely to be fruitful, given the public’s increasing awareness of the health consequences of tobacco use and secondhand smoke. Reports of such efforts would be very useful to the field.
CONCLUSION
An ongoing dialogue between quitline research and practice
Early telephonic cessation programmes had few research results to guide the provision of service. Perhaps in consequence, they provided only brief service, and only on a reactive basis. Subsequent studies showed that a comprehensive planning session before quitting could increase users’ chances of making a successful attempt, and that multiple sessions proactively delivered after the quit attempt could help them avoid relapse, or restart the process if they did relapse. The next generation of telephonic cessation programmes operationalised these findings and, in so doing, shaped how quitlines are generally thought of today, as comprehensive, proactive, multisession behaviour modification counselling programmes. Practice has followed research to a large extent.
Quitline practice, in turn, now poses several key questions for research. For quitlines providing pharmacotherapy, what is the most cost effective dosing? Over the long term, are there differences in population impact between the approach of using pharmacotherapy give-aways to promote quitlines versus more traditional media campaigns? Will technological innovations in telephony or web based applications increase programme effectiveness? Can quitlines provide an effective service for special populations such as pregnant or adolescent smokers or tobacco users with mental illness? Can quitlines improve their overall cost effectiveness by triaging callers to different levels of service based on risk factors? Are quitlines as effective for proactively enrolled participants as for those who call a quitline on their own initiative? To what extent can quitline promotion increase both aided and unaided quit attempts and lead to increased cessation across the population? Solid evidence addressing these questions would probably find quick application in quitline practice.
What this paper adds
Since the first studies of telephone counselling for tobacco cessation began appearing in the early 1990s, there have been many published reports on the operation and effects of quitlines. None has traced the development of quitlines from their origins to their likely future directions and mapped the shifting line between quitline research and practice.
This paper provides an overview of events that led to the widespread adoption of quitlines as central components of tobacco control programmes, and offers recommendations for further development. In illuminating some of the areas where decisions are needed, it indicates where evidence for making such decisions is lacking. The paper can be read as a dialogue between research and practice, with research contributing findings that can be used to shape quitline practice, and practice articulating what it needs from future quitline research.
Acknowledgments
The authors’ thinking on quitlines was shaped in large part by our experience operating the California Smokers’ Helpline, supported by the California Department of Health Services, Tobacco Control Section, under contracts 90-10961, 92-15416, 96-27049, 00-90605, and 05-45834, and First 5 California, under contract CCFC-6810. We are especially gratefully to Ms. April Roeseler and colleagues in the Tobacco Control Section (now a part of the California Department of Public Health), who were the first to see the potential of statewide, evidence based quitlines before they even existed. We would like to thank the reviewers for their detailed comments and Linda Bailey and Julie Wang for their help with the quitline map.
REFERENCES
Footnotes
Competing interests: The authors operate the California Smokers’ Helpline, and conduct government funded quitline research there.