Article Text

Abstract
Objective To examine levels of support for comprehensive smoke-free policies in six large Chinese cities.
Methods Data from Wave 1 of the International Tobacco Control (ITC) China Survey (April–August 2006) were analysed. The ITC China Survey employed a multistage sampling design in Beijing, Shenyang, Shanghai, Changsha, Guangzhou and Yinchuan (none of which has comprehensive smoke-free policies in place). Face-to-face interviews were conducted with 4815 smokers and 1270 non-smokers. Multivariate logistic regression models were used to identify factors associated with support for comprehensive smoke-free policies.
Results About one in two Chinese urban smokers and four in five non-smokers believed that secondhand smoke (SHS) causes lung cancer. The majority of respondents supported comprehensive smoke-free policies in hospitals, schools and public transport vehicles while support for smoke-free workplaces, restaurants and bars was lower. Levels of support were generally comparable between smokers and non-smokers. Support for comprehensive smoke-free policies was positively associated with knowledge about the harm of SHS. Respondents who worked in a smoke-free worksite or who frequented smoke-free indoor entertainment places were more likely to support comprehensive smoking restriction in bars and restaurants.
Conclusion Considerable support for smoke-free policies exists in these six large cities in China. Greater public education about the dangers of SHS may further increase support. Experiencing the benefits of smoke-free indoor entertainment places and/or workplaces increases support for these policies and suggests that some initial smoke-free policy implementation may hasten the diffusion of these public health policies.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Secondhand smoke (SHS) exposure causes death, disease and disability.1 In China, the biggest tobacco producer and consumer in the world, SHS is a serious public health problem. The 2002 China national epidemiological survey on smoking behaviour suggested that 51.9% of the Chinese non-smokers were exposed to SHS for at least 15 minutes daily for more than one day every week.2 It was estimated that in 2002, more than 100 000 Chinese died from diseases associated with SHS exposure.3
Workplaces and public venues are common sources of SHS exposure; therefore, restricting smoking in these venues through smoke-free policies is an effective way to reduce SHS exposure and to protect health.4–6 The World Health Organization Framework Convention on Tobacco Control (FCTC) requires ratifying countries, which China ratified in October 2005, to “adopt and implement in areas of existing national jurisdiction as determined by national law and actively promote at other jurisdictional levels the adoption and implementation of effective legislative, executive, administrative and/or other measures, providing for protection from exposure to tobacco smoke in indoor workplaces, public transport, indoor public places and, as appropriate, other public places”. Studies suggest that to achieve the best SHS reductions the smoke-free policies must be comprehensive7—that is, all indoor workplaces and public places must be smoke-free without exception. In comparison, partial smoke-free policies that allow designated smoking areas or rooms do not offer adequate SHS protection. Today, 16 countries have comprehensive smoke-free indoor air laws at the national level; and some countries have substantial levels of comprehensive subnational smoke-free policies including Canada, Australia and the United States.7
China does not have a comprehensive smoke-free law at the national level. However, several national laws and policies regulate smoking in public places. For example, Regulations on the Sanitary Administration of Public Places bans smoking in gymnasiums, libraries, museums, art galleries, marketplaces, bookstores, public transport waiting rooms, trains, passenger liners and aeroplanes. Law of the People’s Republic of China on Tobacco Monopoly “bans or restricts smoking in public transportation vehicles and public venues”. Law of the Peoples Republic of China on the Protection of Minors bans smoking in the classrooms, dorms and activity rooms of middle or primary schools, kindergartens and nurseries. No national level laws restrict smoking in workplaces, restaurants and bars, which are all common venues for SHS exposure. Although these national level laws are not comprehensive and not well enforced,8 they were the first smoke-free laws in China and became the templates for subsequent local level smoke-free laws and policies. About half of the Chinese cities have city level smoke-free policies, although most of these policies are just mirroring the national level laws and the enforcement is limited.8 9 Only a few cities’ local laws are more stringent than the national laws. For example, Guangzhou’s local smoke-free law bans smoking in workplaces and restaurants with air conditioning, which is beyond the scope of the national laws.
By ratifying the FCTC, China has agreed that all workplaces and public places should be smoke-free by 2011. Recently, efforts have been made in China to expand smoke-free places. At the national level, the central government is revising the Regulations on the Sanitary Administration of Public Places. At the local level, many cities are also strengthening smoke-free policies. For example, in March 2008, Beijing released its new regulations on the scope of banning smoking in public places, which restrict smoking in workplaces though they are not comprehensive and designated smoking rooms are still allowed. In addition, the new regulations require restaurants to set up non-smoking areas, which makes Beijing the third city (along with Guangzhou and Shenzhen) in China that partially bans smoking in restaurants. Just like in the United States where the first smoke-free policies were incremental but they laid the framework for subsequently stronger policies, the new Beijing regulations are considered an important step towards the fulfilment of Article 8 of the FCTC and will lead the way for the rest of China.
Despite the progress being made, China is still far from 100% smoke-free in public venues and workplaces, though the deadline to fulfil the country’s commitment to Article 8 in FCTC is very close. We expect that China will formulate stronger smoke-free policies in the coming years. Thus, to study China's attitudes towards smoke-free policies and factors associated with support for smoking bans is valuable and has important policy implications. Previous studies suggest that comprehensive smoke-free policies are popular,7 10 well complied with7 11 12 and that support for smoke-free policies is associated with knowledge about the adverse health effects of SHS.11 There is also evidence that public support for smoke-free policies increases after the smoke-free policies are implemented.13 14 However, all of these studies were conducted in Western countries with different cultural norms about smoking, and it is unclear if these findings will generalise to China, where one-third of the world smokers live.
The current study uses data from six cities in China to address three research questions: (1) what are the smoke-free policies in six large Chinese cities; (2) what percentage of smokers and non-smokers support comprehensive smoke-free policies in different public venues and workplaces; and (3) what factors are associated with support for comprehensive smoke-free policies?
Methods
Participants
The ITC China Survey is a prospective cohort survey in six large cities in China: Beijing, Shanghai, Guangzhou, Shenyang, Changsha and Yinchuan. The Wave 1 survey was conducted between April and August 2006. About 800 smokers and 200 non-smokers were interviewed in each city for a total of 4815 smokers and 1270 non-smokers completing the Wave 1 survey across cities. Subsequent waves of data collection are being performed in this cohort, but for the purposes of this paper only data from the baseline 2006 survey are analysed.
In this paper, a smoker refers to a respondent who had smoked more than 100 cigarettes in lifetime and smoked at least weekly at recruitment, and a non-smoker refers to a respondent who had not smoked 100 cigarettes in lifetime or who didn’t smoke weekly at recruitment.
Sampling design
The six cities were selected based on their size, diverse geographic location and level of economic development (see fig 1). Table 1 shows the population size and the smoke-free policies in the six cities at the time the survey was conducted in 2006. The registered population in each city is 11 million in Beijing, 5 million in Shenyang, 13 million in Shanghai, 2 million in Changsha, 6 million in Guangzhou and 1 million in Yinchuan.15 In 2006, all the six cities had comprehensive or partial smoke-free policies for hospitals, conference rooms, public transportation vehicles and schools. However, for restaurants and workplaces, only Guangzhou had partial smoke-free policies (places with air conditioning are required to be smoke-free), and the other five cities had no restrictions on smoking in these two kinds of venues.

The geographical distribution of the ITC China cities.
Population size and the smoking policies in different venues in the six cities in 2006
In each city, the ITC China Survey employed a multistage cluster sampling design where 10 street districts (Jie Dao) were randomly selected, with probability of selection proportionate to the population size of the Jie Dao. Within each of these Jie Dao, two residential blocks (Ju Wei Hui) were selected with probability proportionate to the population size of the Ju Wei Hui. Within each selected Ju Wei Hui, a complete list of addresses of the dwelling units (households) was compiled and a simple random sample without replacement of 300 households was drawn from the list to construct the sampling frame.
Each of these 300 households was visited to attempt to complete a survey(s), and information on age, gender and smoking status for all adults living in each household was collected. The enumerated 300 households were then randomly ordered, and adult smokers and non-smokers were then approached face to face following the randomised order until 40 adult smokers and 10 adult non-smokers were surveyed. Because of low smoking prevalence among women, one male smoker and one female smoker from every selected household were surveyed whenever possible to increase the sample size for women. At most one non-smoker was interviewed per household. Where there was more than one person in a sampling category to choose from in a household, the next birthday method was used to select the individual to be interviewed.
Procedure
After providing the potential respondent with information about the survey they completed the consent form, the average time to complete a survey was 31.4 minutes for smokers and 10.6 for non-smokers, with respective interquartile ranges of approximately 10 minutes and 5 minutes, respectively.
Interviewers followed a strict protocol in their interview session with each respondent. Up to four visits to a household were made in order to interview the target person(s) within that household. The Wave 1 cooperation rates, defined as the proportion of all respondents interviewed of all eligible subjects ever contacted, ranged from approximately 80% in Beijing and Guangzhou to 95% in Changsha. The response rates, defined as the proportion of all cases interviewed of all subjects that we tried to reach, ranged from 39.4% in Yinchuan to 66.0% in Guangzhou. All materials and procedures used in the ITC China Survey were reviewed and cleared for ethics by the research ethics board at the University of Waterloo and by the institutional review boards at the China National Centers for Disease Control and Prevention.
To understand the current smoke-free law in each city, during the field work we collected the local smoke-free law in each city. These laws were reviewed to address the first research question.
Measures
The dependent variable in this study is support for comprehensive smoke-free policies in various public places. In the survey, respondents were asked, “for each of the following public places, please tell me if you think smoking should not be allowed in any indoor areas, should be allowed only in some indoor areas, or no rules or restrictions.” Venues being asked include hospitals, workplaces, conference rooms, restaurants or bars, public transportation vehicles, and schools.
The major independent variables and control in this study include:
City (Beijing, Shenyang, Shanghai, Changsha, Guangzhou, Yinchuan)
Gender (male, female)
Age (18–34 years, 35–44 years, 45–54 years, 55 years or older).
Highest level of education (low = no education or elementary school, medium = junior high school or high school/technical high school, high = college, university or higher)
Household income per month (low: <1000 yuan per month, medium: 1000 yuan to 2999 yuan, high: >3000 yuan, don’t know/cannot say)
Ethnicity (Han, others)
Whether respondents believe that “smoking causes lung cancer in non-smokers from second hand smoke” (yes, no)
Self-reported smoking rules at workplaces: In the survey respondents were asked, “Which of the following best describes the smoking policy where you work?” Response options include smoking is not allowed in any indoor areas, smoking is allowed only in some indoor areas, no rules or restrictions, and others.
Self-reported smoking rules in indoor entertainment places that the respondents go most often: In the survey respondents were asked, “Which of the following best describes the rules about smoking in indoor entertainment places such as restaurants, coffee shops, and karaoke lounges that you go most often?” Response options include smoking is not allowed in any indoor areas, smoking is allowed only in some indoor areas, no rules or restrictions, and others.
Cigarettes smoked per day (1–10, 11–20, 21–30, 31+, only used in the analysis of smokers)
Weighting procedures
Sampling weights were constructed to provide the best possible prevalence estimates. The weights were constructed separately for male adult smokers, female adult smokers, and adult non-smokers. Wave 1 weights were constructed by taking into account the four levels of sample selection: Jie Dao, Ju Wei Hui, household and individual. The final weight for a sampled individual was the number of people in the city population and the sampling category represented by that individual. A full description of the weighting methodology is available at http://www.itcproject.org. All results reported in this paper are weighted statistics unless otherwise noted.
Statistical analyses
SPSS for Windows version 13.0 was used for all analyses. The percentages of respondents who support comprehensive smoke-free policies in different venues were computed. Multivariate logistic regression models were developed to examine factors associated with comprehensive smoke-free policies. The analyses were conducted with the SPSS complex samples module to account for the possible nested effects within cities. All the analyses were stratified by smoking status.
Results
Table 2 describes the sample characteristics and the belief about the adverse health effects of SHS. The majority (94.9%) of the smoking respondents are male, but among non-smokers, females represented a majority of the sample. More than 30% of the study respondents were aged 55 years or older. Over 90% of both non-smokers and smokers belonged to the Han ethnic group. A key group difference was noted for knowledge of SHS effects—53.6% of the smokers and 81.4% of the non-smokers endorsed the belief that SHS causes lung cancer in non-smokers.
Sample characteristic, belief about the harm of secondhand smoke (SHS) of the ITC China baseline respondents
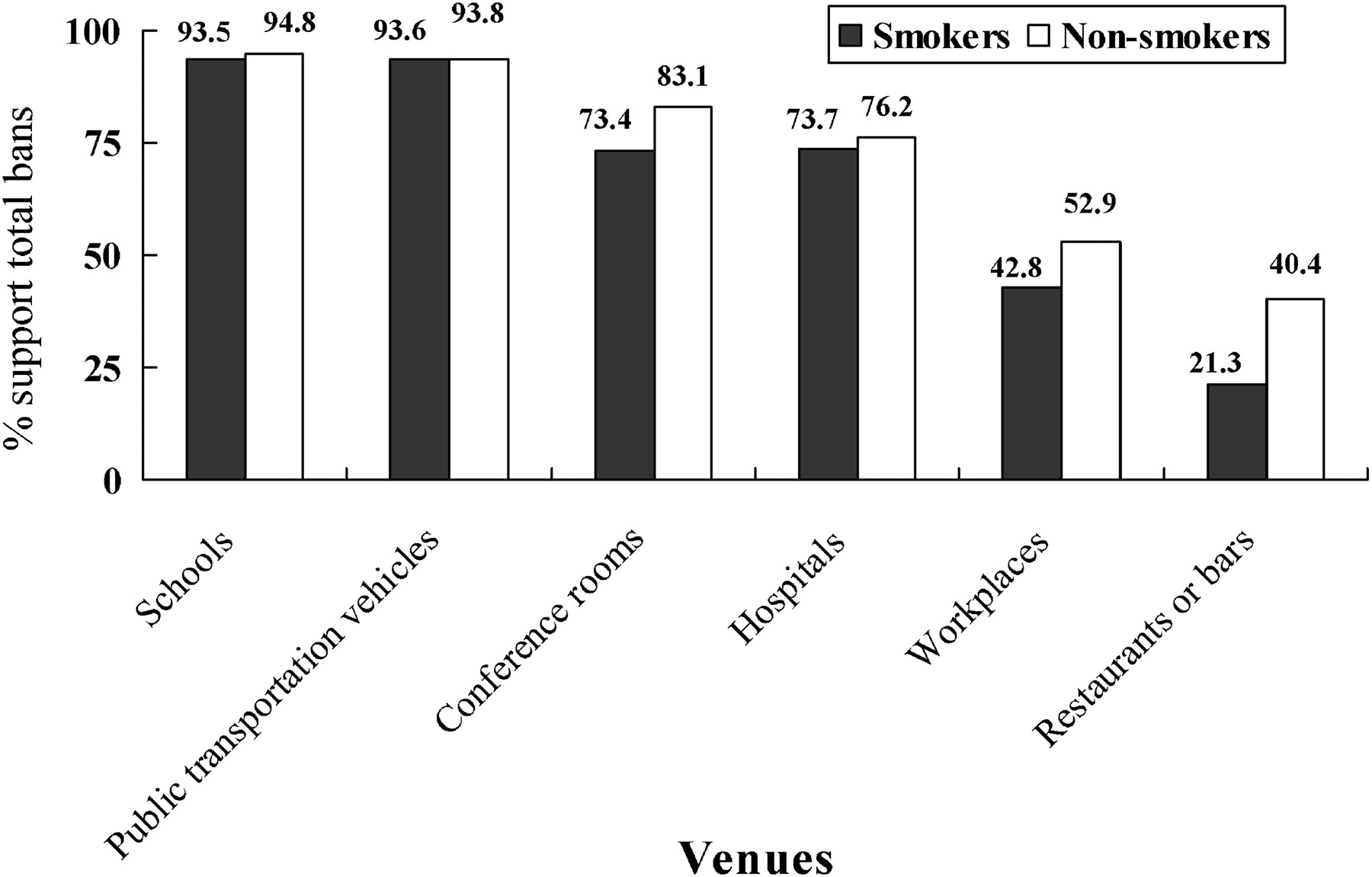
Figure 2 shows the percentages of support for comprehensive smoke-free policies in different venues among smokers and non-smokers. Smokers’ support is highest for public transportation vehicles (93.6%) and schools (93.5%), followed by hospitals (73.7%), conference rooms (73.4%), workplaces (42.8%) and restaurants or bars (21.3%). Non-smokers’ support tends to be higher than smokers, but shows similar patterns.

{kind=link}
{kind=link}
Support for total smoking bans in different venues among smokers and non-smokers in six cities in China. Notes: National level smoke-free laws are in place for schools, public transportation vehicles, conference rooms and hospitals. No national laws restrict smoking in workplaces, restaurants and bars. According to the local smoke-free laws in the six cities, smoking is allowed in workplaces, restaurants and bars except that Guangzhou bans smoking in workplaces and restaurants with air conditioning.
Tables 3 and 4 show the results of logistic regression models predicting support for total smoking bans in workplaces (table 3) and restaurants/bars (table 4), the two venues with the lowest support level for total smoking ban. Several factors were associated with support for total ban in both venues. For example, knowledge about the adverse health effects of SHS was positively associated with smokers' support for total ban in both venues and non-smokers' support for total ban in restaurants/bars. Older and lighter smokers were more likely to support smoke-free policies in these two venues compared with younger and heavier smokers. Self-reported smoking rules at workplaces were associated with support for total ban at workplaces among both smokers and non-smokers. Compared to respondents who work at places without restrictions on smoking, those who work at places with total a smoking ban were more likely to support total ban. Similarly, self-reported smoking rules in indoor entertainment places that the respondents go to most often were also associated with support for a total ban in restaurants and bars among smokers. Respondents who went to indoor entertainment venues with total smoking bans were more likely to support total ban in restaurants or bars. Several factors differed in terms of the association with support for total ban in the two venues. Female smokers were more likely to support total smoking ban in workplaces, but this association only showed borderline significance for restaurants or bars (OR = 1.61, 95% CI 0.99 to 2.59). With regard to the differences between cities, smokers and non-smokers in Yinchuan were more likely to support a total ban in workplaces than those in Beijing; while for restaurants or bars, smokers in Shenyang and non-smokers in Guangzhou were more likely to support total ban compared to those in Beijing.
Results of multivariate logistic regression models predicting support for total smoking ban at workplaces
Results of multivariate logistic regression models predicting support for total smoking ban in restaurants or bars
Discussion
This study is the first to examine the support for smoke-free policies in different venues among urban residents in China. The major findings of the current study include: (1) in the six cities, support for total smoking ban in schools, public transportation vehicles, hospitals, and conference rooms was relatively high among both smokers and non-smokers, while support for a total ban in workplaces, restaurants and bars was present in a sizeable minority of respondents; (2) knowledge about the adverse health effects of SHS and the presence existing smoke-free policies was associated with increased support for a total smoking ban in workplaces, restaurants and bars.
Studies in other countries suggest that support for bans was strongest for those with bans already in place.11 In other words, despite some initial scepticism among the public, once they experience the benefits of smoke-free places they grow to adapt and support these policies. Two findings of the current study add evidence to this. First, we found that support for total smoking ban was high for venues covered by smoke-free policies in most cities, such as schools, public transportation vehicles, hospitals and conference rooms; in comparison, for workplaces, restaurants and bars where most cities had no restrictions on smoking, support for total ban was lower. Second, we found that if respondents’ workplaces or the indoor entertainment places that the respondents go most often had total smoking bans in place, they would be more likely to support total ban in these venues. These findings, combined with previous study results, suggest that comprehensive smoke-free policies grow in their popularity over time. Once implemented, smoke-free policies are likely to get extensive support from the public, even if the policy didn't get high levels of public support before it was implemented. For example, before Ireland made the national level comprehensive smoke-free law in 2004, support for total smoking ban in bars among Irish smokers was only 13%; while one year after the law was enforced, the number increased to 46%.13 In this study, 21.3% of the smokers in the six cities support total smoking ban in restaurants or bars (much higher than support among Irish smokers before the Ireland smoke-free policy). Therefore, although this study shows that support for total smoking ban in workplaces, restaurants and bars was relatively low among urban residents in China, it does not necessarily mean that China cannot enforce comprehensive smoke-free policies in these venues. On the contrary, the results of this study suggest that, like smokers in other countries, Chinese smokers are likely to adapt to and even eventually support smoking bans.
Knowledge about the adverse health effects of SHS is associated with support for total smoking ban in workplaces, restaurants or bars. This is consistent with previous studies.11 In the present study, only 53% of the smokers knew that SHS causes lung cancer, which is lower than in Western countries. For example, in the ITC four-country survey conducted in 2002, this statistics was 76.9% in Canada, 82.6% in the United States, 82.2% in United Kingdom and 72.1% in Australia. There is still room to increase Chinese urban smokers’ knowledge level about the health harm of SHS. We should educate the public knowledge about SHS as this may increase public support for smoke-free policies.
Differences between cities do not show a consistent pattern. One might have predicted that the highest levels of support for smoke-free bars and restaurants to be found in Guangzhou, where partial smoking restrictions were in place at the time the survey was conducted; however, this association was only observed among non-smokers. This may be attributed to the weak nature of the Guangzhou smoke-free policy. The Guangzhou smoke-free law is not comprehensive and exceptions are allowed in restaurants, and the enforcement of the law is also limited.9 Such a policy may only have very limited effects. Therefore, the Guangzhou public doesn’t truly experience a complete smoke-free environment. This finding indicates that a partial smoking ban may be ineffective and not as popular as comprehensive smoke-free laws in other countries.
We found some age and gender differences in this study. Generally, older people were more likely to support smoke-free policies in workplaces, restaurants or bars, a finding consistent with previous studies. Female smokers were more likely to support total smoking ban in workplaces, restaurants or bars, which is inconsistent with findings by Borland et al.11 One possible interpretation is the cultural differences between China and Western countries. However, because the number of female smokers is very small in this study, further studies with larger sample size of female smokers are needed to verify this finding. Heavier smokers are less likely to support comprehensive smoke-free policies. Future research is needed from longitudinal samples to determine whether the support for smoke-free policies in these population changes over time and what factors drive those changes.
The strengths of the current study include a large sample size, a representative sample of smokers and non-smokers in each city, and the multi-city design which allows us to do comparisons among cities. There are several limitations in the study. First, the study was conducted in only six Chinese cities. The study sample is not representative of the whole Chinese population, and the results cannot be generalised to the national level. The rural population, which represents 54.3% of the total population in China, was not examined in this study. Perhaps a similar study conducted in rural areas of China can help address this limitation. Second, because older people were more likely to be at home and to cooperate with the investigation, this study slightly oversampled older respondents, which may result in biased estimates. However, the weighting procedure used in the analyses may help reduce the bias. Third, because of the cross sectional feature of the baseline data, this study is not able to make causal links. Fourth, the cooperation rate and the response rate vary among cities. The reason might be the differences in culture and economic levels. It is not clear whether and how those who refused to participate in the study differ from those who completed the survey, and this may generate bias in the results. Lastly, there are minor differences among surveys in different countries, which made some comparison among countries hard to do. For example, the ITC China Survey asked for respondents’ attitudes towards smoking ban in “restaurants or bars”, while the ITC surveys in other countries asked about restaurants and bars separately.
Conclusion
Considerable support for smoke-free policies was observed in six cities in China. The current study suggests that smoke-free policies are popular. Once smoke-free policies are implemented, both smokers and non-smokers adapt and support these policies. The level of public knowledge about the adverse health effects of SHS was associated with support for smoke-free policies. The opportunity is ripe for public education to further boost awareness of SHS and support for smoke-free policies in China.
Acknowledgments
The authors would like to acknowledge the Chinese Center for Disease Control and Prevention and the local CDC representatives in each city for their role in data collection.
Supplementary materials
Chinese Version 19/Suppl_2/i40
Files in this Data Supplement:
Footnotes
Funding The ITC China Project was supported by grants from the US National Cancer Institute (R01 CA125116 and the Roswell Park Transdisciplinary Tobacco Use Research Center (P50 CA111236)), Canadian Institutes of Health Research (79551), Chinese Center for Disease Control and Prevention and the Ontario Institute for Cancer Research.
Competing interests None.
Provenance and oeer review: Not commissioned; externally peer reviewed.