Article Text

Abstract
Objectives A four-stage model of the cigarette epidemic was proposed in 1994 to communicate the long delay between the widespread uptake of cigarette smoking and its full effects on mortality, as had been experienced in economically developed countries where cigarette smoking became entrenched decades earlier in men than in women. In the present work, the question of whether qualitative predictions from the model have matched recent trends in smoking and deaths from smoking in countries at various levels of economic development is assessed, and possible projections to the year 2025 are considered.
Methods The proportion of all deaths attributed to tobacco was estimated indirectly for 41 high-resource and medium-resource countries from 1950 to the most recent year for which data were available, generally about 2005–2009. The trends in tobacco-attributed mortality in later middle age were then projected forward to 2025, based on recent trends in tobacco-attributed mortality in early middle age.
Results In developed countries the prevalence of smoking has continued to decrease in both sexes, although the rate of decrease has slowed and is less than that predicted by the original version of the model. Over the past 20 years the proportionate contribution of smoking to all deaths has decreased in men while continuing to increase or plateau among women. Although the proportion of all deaths at ages 35–69 that are attributed to smoking is still generally greater in men than in women, the male and female proportions are converging and will probably cross over in some high resource countries. Projections through to 2025 suggest that male and female smoking prevalence and smoking-attributed mortality will decrease in parallel in most developed countries towards lower limits that are not yet defined. In developing countries the model seems generally applicable to men but cannot predict whether or when women will begin smoking in large numbers. Modified criteria that describe the stages of the epidemic separately for men and women would be more generalisable to developing countries.
Conclusions The four-stage model of the cigarette epidemic still provides a reasonably useful description in many developed countries. Its relevance to developing countries could be improved by describing the stages of the epidemic separately for men and women.
Statistics from Altmetric.com
Introduction
Almost 20 years ago in this journal, Lopez et al1 suggested a four-stage model for describing the effects on mortality of the cigarette epidemic in economically developed countries. This model (shown in its original form in figure 1) illustrated that in high resource Western countries such as the USA, UK and Australia, the rise and fall in female smoking and in smoking-attributed mortality lagged behind that in men by about 20–30 years. In both sexes the main increase in smoking-attributed mortality in middle age came several decades after the main increase in smoking among adolescents and young adults. By depicting the epidemic as a continuum spread over many decades rather than as a series of isolated episodes, the model allowed countries to see themselves as being at a particular stage of an understandable process, spread over a whole century. In particular, it showed that even if cigarette consumption started to fall substantially while the steep rise in smoking-attributed mortality was still in progress, the rise in mortality would often be expected to continue for some time, as a delayed consequence of increases decades earlier in cigarette consumption by young adults.

Schematic diagram proposed in 1994 for economically developed countries.1 The criteria used to define the stages of the epidemic are based on the comparative levels of smoking prevalence and smoking-attributed mortality in men and women.
The original model1 was intended to provide a schematic (qualitative) diagram of the course of the epidemic in developed countries for which indirect estimates of smoking-attributed deaths had recently been published.2 3 No corresponding model was proposed for developing countries, since at the time there were virtually no nationally representative surveys of smoking prevalence in these countries nor were there reliable estimates of smoking-attributed mortality. The criteria used to define the four stages of the epidemic were based on the comparative levels of smoking prevalence and smoking-attributed mortality in men and women. Stage 1 was the beginning of the epidemic when the prevalence of cigarette smoking was less than 20%, principally involved men and cigarettes had, as yet, caused few deaths. Stage 2 was characterised by a rapid increase in male smoking prevalence towards a peak of 40% to 80%, the start of the main increase in female smoking and the start of the main increase in mortality from cigarettes (which, however, at the end of that stage still accounted for only about 10% of male deaths and few female deaths). Stage 3 involved a flattening or downturn in smoking among men and some convergence of male and female smoking prevalences, while smoking-attributed mortality rose steeply from under 10% to perhaps 30% of all deaths, most of these being in men. In stage 4, although prevalence was decreasing in both sexes, deaths attributed to smoking continued to rise for a time, peaking at about one-third of all male deaths (more in middle-aged men) and a smaller proportion of all female deaths, before beginning to decline.
A disadvantage of these 1994 criteria is that they cannot be applied to developing countries where cigarette smoking and smoking-attributed mortality are high among men but there is as yet no large increase in female smoking and little female smoking-attributed mortality. Such is the case in China and India where major studies conducted since the model was proposed have directly confirmed substantial hazards from smoking among men (particularly among those who started to smoke before age 20 years) and low smoking prevalence among women.4–7 Inability to apply the 1994 criteria to developing countries is an important limitation, since the WHO projects that by 2030 low and medium resource countries will account for 7 of every 10 deaths from smoking.8 Thus it is timely to reconsider how best to describe the evolution of the epidemic among men and women in different populations.
In this article we propose a modification of the original model to allow the different stages to be described separately for the male and the female epidemics in a particular country. The revised model, like the original version, illustrates the delay of many decades that always occurs between a widespread increase in cigarette smoking by young adults and its full eventual effects on mortality. It again suggests that women who smoke like men (the highest risk being in those who start young and do not quit) will die like men.9 The revised model makes no assumptions, however, about if or when an increase in cigarette smoking will occur among women in the country of interest. A minor further change is that the original model emphasised smoking-attributed proportions of all deaths, while the revised model chiefly emphasises smoking-attributed proportions of all deaths in middle age (defined as 35–69), although it does also provide links to estimates of smoking-attributed proportions at older ages, and at all ages.
Our analyses first update the indirect estimates of smoking-attributed proportions of deaths in middle age in 41 OECD countries or former socialist countries to the most recent year for which mortality statistics for those countries are available through WHO (usually somewhere in the range 2005–2009).10 We then discuss the implications of data on smoking prevalence recently collected in many developing countries by the Global Adult Tobacco Survey (GATS)11 and Global Youth Tobacco Survey (GYTS).12 Lastly we consider how best to describe changes in smoking prevalence and smoking-attributed mortality since 1950, and we suggest semiquantitative projections forward to 2025.
Methods
As in the original model, estimates of smoking-attributed mortality in developed countries are based on an indirect approach, in which absolute lung cancer death rates are used as an approximate guide to the smoking-attributed fractions of the deaths from various groups of other diseases.2 3 The argument is that if, in a developed country, lung cancer rates are low then smoking is causing few lung cancer deaths and hence it is probably causing only a small proportion of the deaths from other causes; conversely, if in a developed country lung cancer rates are high then smoking is probably responsible not only for most of these lung cancer deaths but also for many other deaths. The merit of this indirect method is that it does not require nationally representative data on smoking prevalence (or nationally representative prospective studies of smoking and mortality), but uses only routinely collected national mortality statistics to estimate the proportion of deaths attributed to smoking. The method is described in detail elsewhere.2 13
To calibrate the relationship between lung cancer rates and smoking-attributed proportions of other diseases, national lung cancer rates, stratified by sex and 5 year age group, are compared with the corresponding lung cancer mortality rates among current and never smokers in the million-person American Cancer Society Cancer Prevention Study II (CPS-II). The excess of the national lung cancer death rates in a particular country over the US non-smoker lung cancer death rates is used not only as a guide to the smoking-attributed fraction of lung cancer mortality but also as a guide to the smoking-attributed fractions of the national mortality from eight other categories of disease: upper aerodigestive tract cancer, other cancer, chronic obstructive pulmonary disease (COPD), other respiratory disease, vascular disease, cirrhosis (none attributed to smoking), other medical causes and non-medical causes (none attributed to smoking). The sum of these smoking-attributed numbers of deaths is then expressed as a proportion of all deaths in that particular country. For obvious reasons, trends in the fraction of all deaths attributed to smoking by this indirect method tend to parallel national trends in lung cancer mortality. For each developed country (and for various groupings of countries such as the European Union) the underlying data plus the updated estimates are appended electronically to this article's online Appendix. These and future updates will also be posted periodically on the Clinical Trial Service Unit (CTSU) website.10
In reconsidering how best to describe the stages of the epidemic in developing countries we also reviewed data on smoking prevalence collected in many developing countries by the GATS11 and GYTS.12 14 The revised model is used to help describe our indirect estimates of smoking-attributed deaths in the USA from 1950 to 200710 and the data on adult smoking prevalence in the USA from 1965 to 2010.14 The mortality projections from 2005 to 2025 were guided by recent trends in early middle age. The plots of smoking-attributed deaths before 1950 and adult smoking prevalence before 1965 were based on interpolation.
Results
Among men, recent trends in smoking prevalence and in the proportion of all deaths at ages 35–69 attributed to smoking have generally been flat or downward in developed countries. This smoking-attributed proportion is not yet decreasing much in Spain, Portugal, Greece, Bulgaria, Romania, Hungary, Norway and Japan, but elsewhere it is; the most extreme decreases are in Finland (down from 38% of all male deaths at 35–69 in 1970 attributed to smoking to 15% in 2009) and the UK (down from 47% in 1970 to 22% in 2009 and still falling: figure 2). This report emphasises ages 35–69 years partly because the proportion of all deaths attributable to smoking is higher in this age range than at older ages, and partly because, other things being equal, premature death in middle age matters more for the individual and those around them than death in old age.
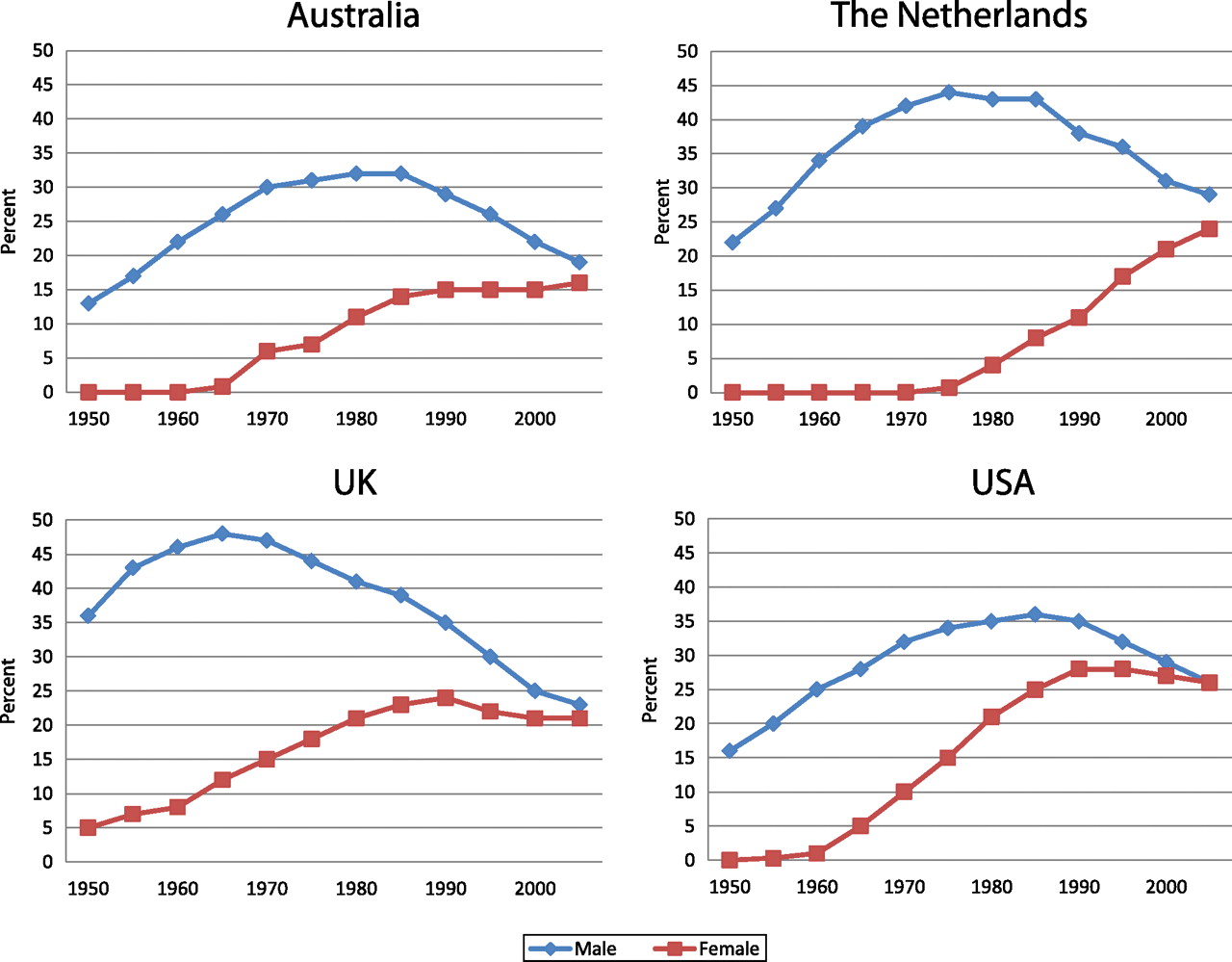
Among women in many developed countries smoking prevalence has also decreased, albeit more slowly than in men, but the proportion of female deaths at ages 35–69 that is attributed to smoking has not yet decreased much in any developed country, and in some it continues to increase rapidly (eg, The Netherlands: figure 2). It is currently highest (26% to 30%) in The Netherlands, Denmark, Hungary and Canada, but is also high (18% to 20%) in the USA and UK (figure 2) and in Norway, Sweden, Poland and New Zealand.
In many high-resource countries male and female smoking prevalences have converged, as have the smoking-attributed proportions of all deaths at ages 35–69. (Note, however that as male death rates are higher than female death rates, if smoking causes a quarter of all mortality at ages 35–69 in both sexes then the absolute rates are higher for men than for women; the electronically appended material gives absolute rates and proportions.) In a few countries such as Denmark and Sweden the male and female smoking-attributed proportions of deaths at ages 35–69 have definitely crossed over, and in some others (eg, The Netherlands, figure 2) they will do so in the early 2010s.
Although the four countries in figure 2 share many economic and cultural characteristics, and the patterns of the epidemics of death from smoking in each of them are broadly similar, there are some differences in timing and magnitude. Men in the UK were among the first to take up cigarette smoking in large numbers. By 1965 they had the highest lung cancer death rates of any major country, and smoking accounted for almost half of all UK male deaths in middle age. The maximum impact of smoking occurred approximately 10 years later among men in The Netherlands and 20 years later among men in Australia and the USA. Notably, the peak value in The Netherlands was almost as high as that in the UK whereas the peak value in Australia was appreciably lower. While no high resource country has managed to avert the epidemic in either sex, some have limited its magnitude more successfully than others.
In developing countries, the lack of nationally representative longitudinal data on smoking prevalence or smoking-attributed mortality limits what is known. In recent years, however, high quality prevalence surveys have been conducted by the GATS in 14 low-income and middle-income countries (the ‘BRIC’ countries (Brazil, Russia, India, China) and 10 others).11 In six of these countries (Bangladesh, China, Egypt, India, Thailand and Vietnam) the prevalence of female smoking remains low (<4%) despite prevalence rates for men (of age 15+ years) that range from 38% (Egypt) to 53% (China). Five other countries with recently collected GATS data (Brazil, Philippines, Russia, Turkey and Ukraine) also have large gender disparities. This illustrates the need to consider the stages of the male and female epidemics separately in these countries.
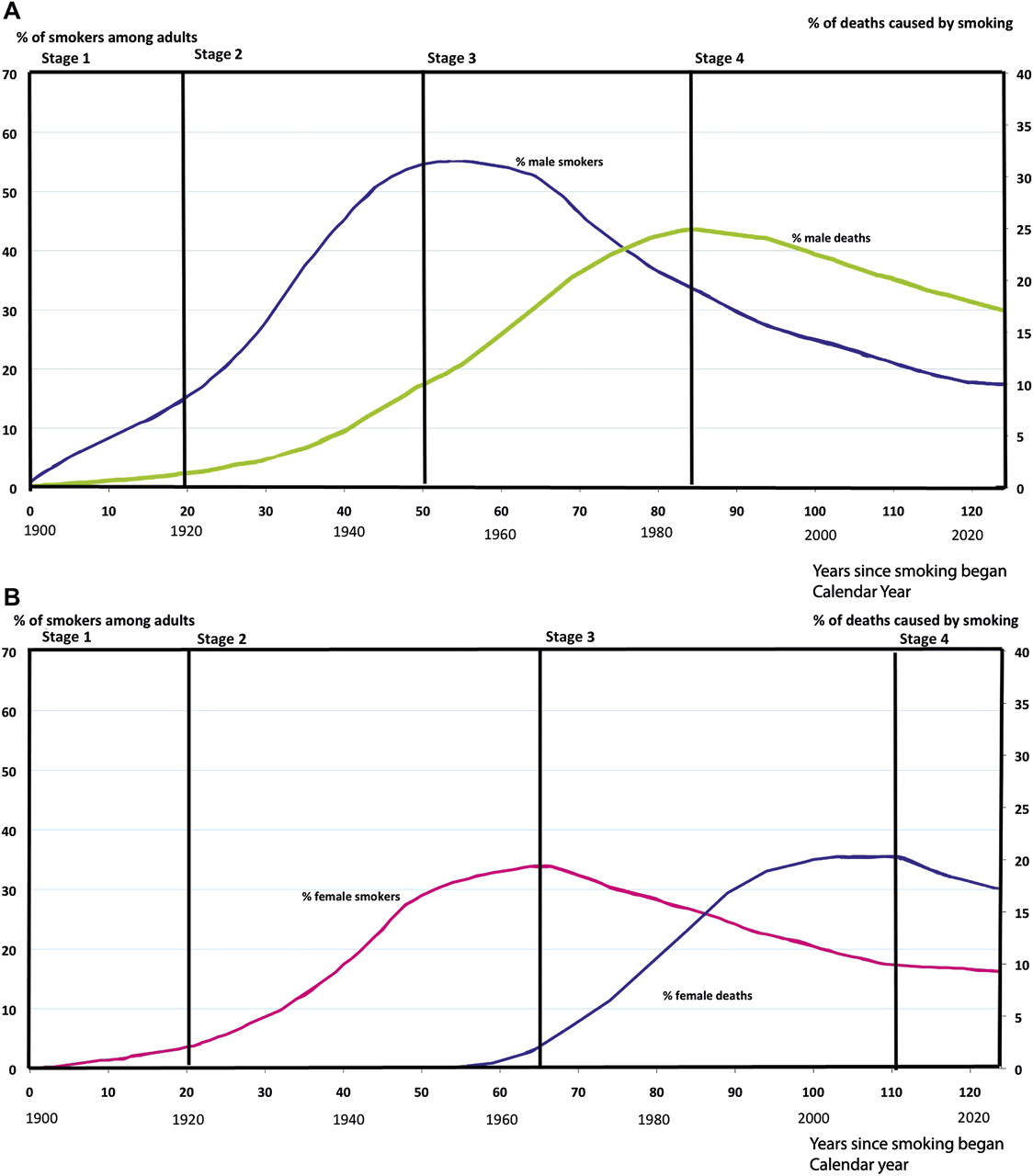
In figure 3 we sketch the hypothetical evolution of the epidemic among men and women in a country such as the USA with a fairly mature epidemic (without suggesting that these sketches accurately represent the USA past or future). These sketches assume that smoking prevalence will continue to decrease in both sexes towards lower limits that are not yet defined. Adult smoking prevalence in the general population might decline to about 15% or less by 2025 in men and women. (In the USA itself the prevalence among medical doctors is now only 2.5%,15 and adult prevalence in California had already declined to 14% in 2005.16) We have modified the criteria used to define the stages of the epidemic in one gender. Stage 1 represents the very beginning of the smoking epidemic when the prevalence of cigarette smoking has only just started to rise, and is still low (<15%) in the gender of interest. In stage 2, smoking prevalence increases rapidly. By the end of this phase, formally defined as the point when prevalence is no longer increasing much, cigarette smoking still accounts for only a limited proportion of all premature deaths; this proportion depends on the rapidity of the preceding increase in smoking. Stage 3 is the period in which although smoking prevalence is stable or decreasing, smoking-attributed mortality is increasing rapidly to an eventual maximum of perhaps 20% to 50% of all deaths at ages 35–69. By definition, stage 3 ends when this proportion is maximal. Finally, in stage 4 smoking prevalence and, eventually, smoking-attributed mortality as a proportion of all mortality decrease towards lower limits that are not yet defined in any population.
{kind=link}
{kind=link}
{kind=link}
(A,B) Data on smoking-attributed deaths represent updated indirect estimates in the USA from 1950 to 2007.10 Data on adult smoking prevalence from 1965 to 2010 represent measurements from the USA National Health Interview Survey. Projections through 2025 estimated based on current trends in early middle age. Estimates of smoking-attributed deaths before 1950 and of adult smoking prevalence before 1965 based on interpolation. Staging criteria modified to describe the stages of the epidemic separately for men and women (see text).
Discussion
Because it is difficult to predict when (or if) women in particular developing countries will begin smoking in large numbers, we recommend that the conventions for describing the stages of the tobacco epidemic in a population be changed to define the stages of the epidemic entirely separately for men and for women. This would allow medium and low resource countries to find themselves in relation to gender-specific continuums. More importantly, it would emphasise that the universal feature of the epidemic is the long delay between the uptake of persistent smoking in a population and its full effects on mortality, not the temporal relationship of these events between men and women. Gender-specific differences are influenced by economic, cultural and political determinants that differ greatly from one population to another.
For example, female smoking lagged behind male smoking by only 20–30 years in the USA and UK, because cultural prohibitions against women smoking largely collapsed during and after World War II.17 In Spain, these cultural prohibitions collapsed several decades later during political liberalisation, so tobacco-attributed mortality among Spanish women is only just beginning to rise. In China, the patterns are completely different; in some parts of China the overall prevalence of female smoking is appreciable among women born before the 1940s but throughout China it is extremely low among women born since the 1950s; hence, since the 1980s the nationwide prevalence of female smoking has halved in China, as those born before the 1940s comprise a diminishing fraction of the population. However, if current cultural prohibitions against smoking among young women erode, there could be a substantial increase in Chinese female smoking. Cultural taboos are vulnerable to social, political and economic changes that change social norms, and Asian women comprise a large untapped market for tobacco companies and governmental tobacco monopolies.
In developed countries as a whole the epidemic of smoking-attributed mortality among women continues to increase, offsetting the reduction in smoking-attributed mortality among men. The smoking-attributed proportion of deaths at ages 35–69 will, at least temporarily, be higher in women than men in some high-resource countries, as is already the case in Denmark and Sweden.10 Eventually male and female smoking prevalence and smoking attributed deaths should decrease in parallel in developed countries but at present sharp increases in the female smoking-attributed proportion of all mortality in middle age are continuing in some populations.
National surveys of adult and youth smoking conducted by GATS11 and GYTS12 over the past 20 years have improved our ability to monitor and modify the course of the epidemic in developing countries. GATS provides evidence of whether appreciable numbers of adult smokers have yet managed to stop, and cessation rates will substantially affect mortality rates over the next few decades. For, although the full hazards of smoking take many decades to emerge, and are therefore greatest among people who initiate smoking in adolescence and continue throughout middle age, the large majority of the excess risk of death due to smoking in middle and old age can be avoided by quitting before age 40, and, preferably, well before age 40.18 GYTS provides early warnings of changes in smoking behaviour in the young that will affect mortality rates several decades hence; currently, the highest levels of youth smoking measured are among boys age 13–15 in Indonesia and Kuwait and boys and girls in South Africa. (Other early warning signs involve the activities of tobacco companies.)
Although the mix of diseases by which smoking kills differs appreciably between different countries, these differences do not undercut the central conclusion that about half of all who start to smoke substantial numbers of cigarettes when young and do not stop will eventually be killed by smoking (although they would invalidate indirect estimation of smoking-attributable mortality in many developing countries from absolute lung cancer rates). For example, studies in China4 5 and India6 7 have found comparably high levels of mortality from smoking, suggesting in both cases that about half of those who start early are killed by smoking (even though, on average, lung cancer rates are much higher in China than in India, partly because there has been heavy domestic air pollution in many parts of China from cooking and heating).
Ultimately, the importance of any model of the epidemic is to help communicate the future health effects of current smoking. The original and the revised model emphasise the long delay between a large increase in smoking in a particular generation of young adults and the full increase in smoking-attributed mortality when that generation reaches middle and old age, and stage 3 of the revised model describes the apparently paradoxical period when cigarette consumption is falling yet smoking-attributed mortality is still rising as a delayed result of earlier increases in smoking. Despite this, however, it is still true that populations and individuals who smoke can by cessation greatly reduce the mortality rates they would otherwise have suffered.
What this paper adds
This paper updates the estimates of smoking-attributed mortality for 41 developed countries to the most recent year for which data are available and proposes a modification of the criteria that define the stages of the cigarette epidemic to allow different stages for men and women. The sex-specific criteria are more generalizable to developing countries than those proposed by the earlier model.
What is already known on the subject
A four-stage model of the cigarette epidemic in developed countries was proposed in 1994 to communicate the long delay between the widespread uptake of cigarette smoking and its full effects on mortality. This model defined the stages of the epidemic based on the comparative levels of smoking prevalence and smoking-attributed mortality in men and women, as had been experienced in economically developed countries.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- The tobacco epidemic today
- Editorial