Article Text

Abstract
East Asia is one of the world's largest tobacco epidemic regions. Although several international studies have evaluated the status of tobacco control in this region, the findings have not been integrated with knowledge on domestic activities at the national and municipal levels. We analysed the current tobacco control situation in three East Asian countries, Japan, China and the Republic of Korea, using both international and domestic data sources. We collected data between 2008 and 2011 in each country according to the framework of WHO's MPOWER (Monitoring, Protect, Offer, Warn, Enforcement and Raise) approach for guiding implementation of the WHO Framework Convention on Tobacco Control. Analysis revealed that 37–53% of adult men were current smokers and that smoking prevalence among middle-aged men reached 63%. Less than 20% of male smokers plan to quit and the use of nicotine replacement drugs was 14% at maximum. Forty-six percent or more of men and 20% or more of women were exposed to passive smoking at workplaces and at home, respectively. Many tobacco industry activities remain unrestricted and prevalent. Our findings indicate an urgent need for the following set of policies: raise cigarette prices to increase the quit attempt rate, particularly among adult men; develop a multi-component quitting assistance system to provide adequate assistance for smoking cessation; implement effective smoke-free policies in workplaces and public places to reduce exposure to passive smoking; and rebuild the administrative structure to denormalise tobacco industry activities. The importance of these standard approaches should be reaffirmed by all tobacco control policymakers in East Asia.
- Global health
- Public policy
- Surveillance and monitoring
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
East Asia is one of the world's largest tobacco epidemic regions. Nearly half of men in this region are cigarette smokers (38.2% in Japan, 52.9% in China and 47.7% in the Republic of Korea).1 China and Japan are the largest and fifth largest tobacco-consuming countries, respectively, with China alone accounting for approximately 38% of total global tobacco consumption.1 Due to these factors, the estimated number of smoking-attributable deaths in China and Japan is 670 000 and 130 000 per year, respectively.2–4 In China, the number of cancer deaths attributable to smoking was recently estimated to be 495 000 annually.5 If tobacco smoking in China continues at the current rate, the annual number of smoking-attributable deaths is estimated to reach 3 million by the middle of the twenty-first century.6
Despite the large health burden of tobacco use in East Asia, comprehensive and comparative information on the present status of tobacco control in this region is scarce. Although several international studies have provided valuable data related to tobacco control in individual countries,7–11 no study has integrated the data with domestic activities at the national and municipal levels to build region-specific strategies. The present study aimed to analyse the current status of tobacco control in three countries in East Asia (Japan, China and the Republic of Korea) to develop policy strategies for changing the world's largest tobacco epidemic region.
Methods
We defined East Asia as a geographical area including Japan, mainland China, Taiwan, the Republic of Korea, and the Democratic People's Republic of Korea. The present study analysed data from three countries (Japan, mainland China and the Republic of Korea). We have discussed the status in Taiwan based on the available literature. In the following sections (including tables and figures), we refer to mainland China as China and the Republic of Korea as South Korea, for simplicity.
We set six themes (Monitoring, Protect, Offer, Warn, Enforcement and Raise) in accordance with the MPOWER package for implementation of the Framework Convention on Tobacco Control (FCTC).7 ,8 FCTC ratification occurred in 2004 for Japan and 2005 for China and South Korea. One or two researchers collected data for the six themes between 2008 and 2011 for each of the three countries examined (Japan: KK; China: JY; South Korea: MKL and SHP). Survey data were selected according to the following criteria: publicly available in a quotable form (mandatory); variables clearly defined to allow for comparative analyses (mandatory); and highly representative of the population (national representative data preferable). For information other than survey data, official information, such as governmental publications, was consulted. Data for the prevalence of adult smoking,12–18 youth smoking,19–21 passive smoking,13 ,14 ,18 ,21–25 and cessation behaviours13 ,14 ,26 were obtained from representative surveys conducted at the national level in each country. Data for cigarette prices, taxes and sales were collected from governmental or official publications.27–31 Information on the availability of pharmacotherapy was obtained from clinical guidelines for each country,32–35 and information on the health warning labels was obtained from laws or official reports of each country.36–38 For collected survey data, those related to active smoking prevalence, passive smoking prevalence and smoking cessation were classified as Monitoring, Protect, and Offer, respectively. Collected data were descriptively analysed and priority issues for tobacco control were extracted through discussion between authors.
Results
Collected data items and their information sources are summarised in the supplementary appendix.
Monitoring (active smoking)
Nearly half of adult men in China and South Korea were active smokers in 2010 (52.9% and 48.3%, respectively, table 1). Smoking prevalence among men in Japan was as high as 37%, even after the price increase in 2010 (from 300 to 410 JPY/pack). When divided into age groups, smoking prevalence in men was over 60% in those aged 50–59 years in China and aged 30–39 years in South Korea.
Comparisons between Japan, China and South Korea in the status of active smoking
The prevalence of ever smokers, that is, current or former smokers, among men in the three countries reached 70–80% among middle-aged men (50–59 years). Average age at smoking initiation among this age group was around 20 years. Specifically, men younger than 40 years started smoking at even younger ages, as low as 17.5 years in Japan.
Smoking prevalence among women was highest in Japan (10%). Average age at smoking initiation among women in the three countries was lower among younger women; for example, the average initiation age was 32.7 years among women in Japan in their 60s and 18.7 years among women in their 20s.
In Japan, teenage smoking prevalence was substantially lower than among adults; only 13% of men and 5% of women aged 18 years said they had smoked 1 day or more during the past month. The smoking prevalence among Japanese male teenagers was approximately half of the corresponding rates in China and South Korea (26% and 27%, respectively), even though the Chinese data excluded those who reported trying to smoke or having smoked only one cigarette if they did not currently smoke.
Protect (passive smoking)
Prevalence of passive smoking exposure in China was remarkably high. Over 70% of adult men and 50–60% of adult women were exposed at home and in workplaces (table 2). Although the absolute prevalence of exposure was lower in Japan and South Korea, the pattern of exposure was similar. Passive smoking was also prevalent among youths, with 35% or more exposed to passive smoking at home in each of the three countries.
Comparisons between Japan, China and South Korea in the status of passive smoking
Currently in Japan, there is no national legislation prohibiting indoor smoking. At the prefectural level, an ordinance to prevent passive smoking in public places exists in only Kanagawa Prefecture, which has a population of 9 million and is located adjacent to Tokyo. However, the ordinance does not mandate a completely smoke-free environment in public places, and does not cover workplaces. None of the three countries has enacted national legislation for smoke-free workplaces. In Japan, revision of the Occupational Safety and Health Act had been scheduled to take place in 2011, and was supposed to include an obligation for employers to prevent exposure to second-hand smoke; however, as of August 2012 the proposed revision has been postponed. Moreover, the bill drafted by the former ruling party did not actually include a provision concerning employers’ obligations. Remarkably, a higher percentage of the Japanese population was supportive of a partial rather than a complete ban, even among non-smokers (54% vs 35% for workplaces, and 56% vs 43% for public places), despite the fact that partial bans have been shown to be ineffective for protecting non-smokers from exposure.39
Offer (smoking cessation)
The percentage of smokers planning or thinking of quitting smoking within 1 year was lower than 20% in the three countries (table 3). Quit attempt rates during the past year among men and women were lower in Japan (21% and 34%, respectively) than in China and South Korea. The percentage of smokers who had attempted to quit smoking without assistance was 77% or higher in the three countries. Use of nicotine replacement drugs (prescription or over the counter) was reportedly only 14% in Japan and 5% or lower in China and South Korea.
Comparisons between Japan, China and South Korea in the status of smoking cessation and quit assistance
The use of smoking cessation drugs is partially covered by health insurance in Japan. However, as of 2011, the coverage is restricted to outpatients and heavy smokers (using the Brinkman index; the number of cigarettes smoked per day multiplied by the number of smoking years ≥200), and a quitline system has not been implemented.
Warn
The package labels of tobacco products are similar in the three countries (figure 1). The labels fulfil only one or two items (‘location’ and ‘language’) of the warning standards recommended by the FCTC (table 4). The health warnings were characterised by small size (30% area of the front and back labels), lack of pictorial use, ambiguous expressions, muted colours, and conveying the impression of reduced harm.
Compliance of warning labels on tobacco products in Japan, China and South Korea with the FCTC requirements

Representative warning labels on cigarette packages in Japan, China and South Korea. Japan front (in Japanese): Smoking increases the risk of worsening your emphysema. (Detailed information is available at the MHLW website, http://www.mhlw.go.jp/topics/tobacco/main.html). Back (in Japanese): Smoking among minors increases adverse health effects and tobacco dependence. You should not smoke even if urged to do so by the people around you. China front (in Chinese): Smoking is harmful to your health. Quitting smoking early is good for your health. Back (in English): Smoking is harmful to your health. Smoking can cause respiratory diseases. South Korea front (in Korean): Warning: Smoking is harmful to your health. Once you start, it is very difficult to quit. Tobacco smoke includes carcinogens such as naphthylamine, nicotine, benzene, arsenic, and cadmium. Back (in Korean): Same as the front label.
Enforcement
The activities of the tobacco industry are largely unrestricted in the three countries (table 5). Particularly in Japan, the regulation of advertisements and sales promotion by the tobacco industry has been enforced only on a voluntary basis. In addition, a large number of corporate advertisements on television, product advertisements in magazines, and sponsorships of sports and social activities remain unrestricted. Legal regulation of advertisements and promotion of tobacco products has been enacted in China and South Korea, although the restrictions are only partial. For example, in Sichuan, China, elementary schools were built under the sponsorship of the tobacco industry as part of the 2008 great earthquake recovery efforts, and in those schools, huge pro-tobacco banners are posted.40 ,41
Current situation of the regulations on tobacco advertisement, promotion and physical sales in Japan, China, and South Korea
Sale of tobacco to minors is legally prohibited in all three countries. In Japan, however, vending machines are widely available nationwide and access is only restricted by their proximity to retailers. Although minors’ access to vending machines is restricted by the requirement for an identification card (eg, the TASPO system in Japan), the system has reportedly been ineffective.19 Tobacco vending machines are also not prohibited in South Korea. In addition, Japan and South Korea do not restrict the proximity of tobacco retailers to schools.
Raise
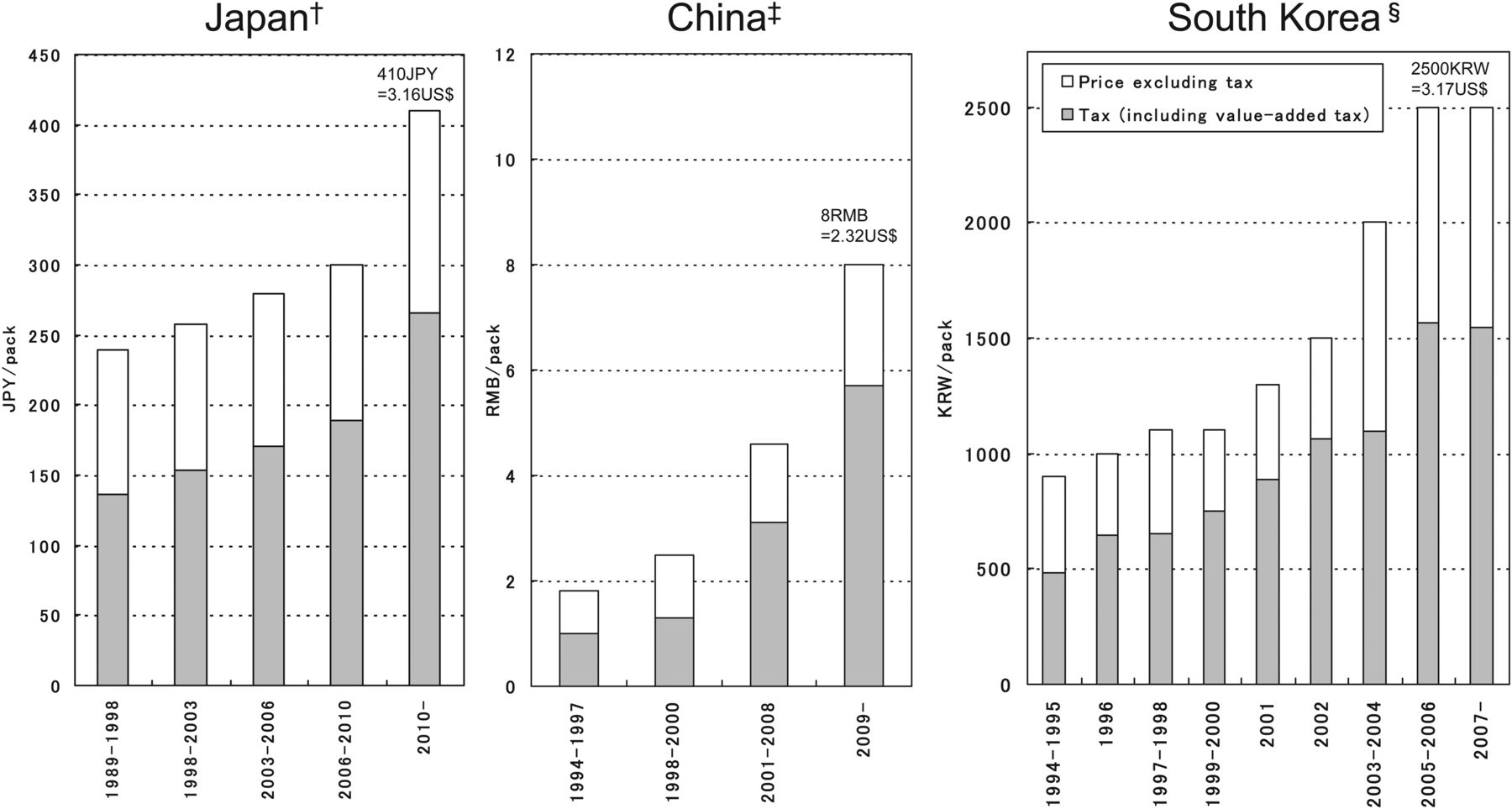
The tax rate of cigarettes in Japan is currently 65% of the retail price (figure 2). The average retail price of cigarettes was raised from 300 to 410 JPY/pack in 2010. However, the current price corresponds to US$3.16 according to the purchasing power parities (PPPs) in 2005,42 which is approximately 33% of the PPP-converted price in the UK (£6.3=US$9.68, according to the identical PPP conversion). Tax rates in China and South Korea are 71% and 62% of the retail price, respectively, which are comparable to the Japanese rate. The PPP-converted price in South Korea (US$3.17) is nearly the same as that in Japan, whereas the converted price in China (US$2.32) is only approximately 73% of that in Japan.

Average price and tax of cigarettes in Japan, China and South Korea. *The figures on the bar for the most recent price and vertical scales were adjusted according to the purchasing power parities: 1 JPY=US$129.55, 1 RMB=US$3.45, 1 KRW=US$788.92 (International Comparison Programme 2005). †For Japanese data, ‘tax’ includes tobacco tax and value-added tax. ‡For Chinese data, ‘tax’ includes tobacco consumption tax and value-added tax. §For South Korean data, ‘tax’ includes tobacco consumption tax, local education tax, fee for health promotion, value-added tax, and other additional fees. Sources: Japan: Ministry of Finance, Japan; China: Potential Effects of Tobacco Taxation, the Chinese Association of Tobacco Control etc; South Korea: National Statistical Office, South Korea.
The number of cigarettes sold per capita in Japan reached a peak in the late 1970s (figure 3). After a second peak in the late 1990s, cigarette sales decreased, falling even more after the year 2000. The trend in per capita cigarette sales in South Korea was similar to that observed in Japan, also rapidly decreasing from 2000. Per capita cigarette sales in China temporarily decreased in the 1990s, but began increasing during the past decade.

{kind=link}
{kind=link}
{kind=link}
Trends in annual average cigarette sales per capita (≥15 years old) in Japan, China and South Korea. *1959–1965 for China; †1983–1985 for South Korea. Sources: Japan: Japan Health Promotion and Fitness Foundation (1920–2007 fiscal year); Annual Report of Japan Tobacco Inc (2008–9 fiscal year); Ministry of Internal Affairs and Communications (population data). China: Institute of Economics, National Agency for Tobacco Monopoly; World Population Prospects, 2008 Revision, United Nations, Department of Economic and Social Affairs (population data). South Korea (domestic sales alone): National Statistical Office, South Korea; World Population Prospects, 2008 Revision, United Nations, Department of Economic and Social Affairs (population data).
When we compared the number of cigarettes sold before and after the 2010 price increase in Japan, the total number of cigarette sales had decreased by 10% in 2010 compared with the value in 2009 (from 233.9 to 210.2 billion cigarettes, respectively).43 This rate of decrease was 2.5-fold higher than the average annual rate of decrease that had occurred during the previous 5 years (from 292.6 billion cigarettes in 2004 to 233.9 billion cigarettes in 2009).
Discussion
In the present study, we analysed the current status of tobacco control in three East Asian countries, based on quantitative data and published information from international and domestic sources.
Analysis
The high smoking prevalence among men in all three countries is a major concern. A peak of ever-smoker prevalence (70%) was observed among men aged 50–59 years, who will have an increased incidence of chronic diseases caused by smoking in later years due to the high accumulated exposure to active smoking.
Factors underlying the high smoking prevalence among men are the low quit attempt rate and poor support for smoking cessation. Among women in China and men and women in South Korea, more than half of each group had attempted to quit smoking. However, judging from the lack of a rapid decrease in smoking prevalence,1 ,44 their success rates are considered to be low.
Smoking cessation drugs are covered by the national health insurance programme in Japan and are freely available at public health centres in South Korea. However, use of these prescription drugs has not substantially increased across the time periods studied.14 ,45 Japan also lags in the effort to promote smoking cessation. The FCTC Parties’ report showed that there were no media campaigns promoting smoking cessation in Japan.46 In China, cessation support drugs are available as over-the-counter formulations and prescriptions, but the country has been slow in developing a medical care support system for cessation treatment. According to the FCTC Parties’ report, China mandates healthcare professionals to promote smoking cessation,47 but there is no systematic support for implementation of such a policy.
Youth smoking prevalence was high among boys in China and South Korea. In Japan, smoking prevalence among minors was low, which is thought to be a result of antismoking education. However, there is a large difference in smoking prevalence between the age cohorts of 18 years and 20–29 years, perhaps reflecting a lack of continuing antismoking education after high school. According to FCTC reports, all three countries stated that measures had been implemented in the area of education,46–48 but there is a problem in that none of the three countries had specific targets for their educational activities.
High exposure rates to environmental tobacco smoke were also common in the three countries. The lack of legislative measures, particularly for workplaces, poses a major challenge. The FCTC reports revealed that Japan lagged significantly behind in smoking bans,46 and this was reconfirmed by the present study.
Underlying the high prevalence of active and passive smoking in the three countries is a lack of effective containment of the tobacco industry activities that undermine tobacco control efforts. In the FCTC Parties’ reports, all three countries stated that they protected tobacco control efforts against interference from the tobacco industry.46–48 South Korea stated in the Parties’ report that the country had implemented comprehensive restrictions on tobacco advertisement, promotion and sponsorship.48 However, this study revealed that indirect advertising by tobacco companies remains prevalent in all three countries. In the Parties’ report Japan cited infringement of the Constitution as an obstacle to enforcing advertising restrictions,46 but there has been no court ruling declaring such restrictions unconstitutional. In South Korea, the legality of advertising restrictions has been affirmed. The support among Japanese people for partial rather than complete bans on workplace and public place smoking is likely to reflect the effects of the large-scale media campaigns by Japan Tobacco Inc (JT), emphasising the coexistence of smokers and non-smokers.
Similarities among the three countries are notable in warning labels. In the FCTC Parties’ reports, the three countries provided the same responses to almost all of the items in the area of Warn.46–48 In the lawsuit over Australia's plain packaging law filed at the High Court of Australia, JT was among the plaintiffs. Following the decision by the High Court to uphold the plain packaging law as constitutional, the EU is now considering adoption of plain packaging. This movement needs to be expanded to East Asia as well.
The price of cigarettes was highest in Japan until 2004, when the price was surpassed by that of South Korea. Although Japan increased cigarette prices by a large margin in 2010, its PPP-converted prices are only around the same as those of South Korea. The reason for cigarette prices in Japan being close to those in South Korea might be that both countries are presumably trying to keep cigarette demand from falling excessively. Smoking prevalence in Japan decreased after the 2010 price increase. However, the decline is not as sharp as that in the number of cigarettes sold. In the same period the proportion of light smokers increased while that of heavy smokers decreased.49 A similar phenomenon was seen in South Korea after cigarette prices were raised in 2005.50 Raising cigarette prices presumably encouraged people to smoke less rather than quitting in these two countries. When Japan's former ruling Democratic Party increased cigarette prices, they declared that it was to protect the health of the Japanese people, rather than to increase tax revenues.51 This marked a major turnaround in the Japanese government's tobacco policies. The Liberal Democratic Party, which returned to power at the end of 2012, has been taking a passive stance towards tobacco control. To prevent the major trend created by the Democratic Party from stalling or regressing, it is important to continue with advocacy efforts.
Proposed policies
Based on our findings, we suggest implementation of the following set of policies in East Asia in a cooperative manner. First, further raising the price of cigarettes is necessary. Tobacco tax policies have enormous potential to encourage quitting among smokers and simultaneously generate considerable tax revenue.52 The potential impact of this approach is particularly large in China,53 which has the lowest cigarette price of the three countries. Japan and China should consider earmarking the additional cigarette tax revenue for health promotion activities, as has already been implemented in South Korea.
Second, policies for increasing quit attempts should be combined with policies assuring adequate cessation support. A multi-component quitting assistance system that includes telephone support and guidance for cessation drugs, which has been shown to be effective in South Korea,54 should also be implemented in Japan and China.55 In addition, population-based approaches using existing healthcare systems are needed to increase successful quitting attempts. In Japan, for example, there are widely prevalent health check-up systems at worksites and community healthcare centres, with 30–40% or higher participation rates.56–58 Conducting brief smoking cessation interventions at health check-up facilities will lead to increased cessation rates.59
Third, effective smoke-free policies in workplaces and public places are required.60 Despite enactment of effective smoking bans at the municipal level (eg, workplaces in Hong Kong and public places in Seoul), national and other provincial governments have been slow in adopting such measures. In 2011, the Japanese Labour Policy Council proposed an ineffective revision of the Occupational Safety and Health Act, which allowed employers to build designated indoor smoking areas with ventilation. This amendment clearly falls below the standards of the WHO guidelines, which state that approaches other than 100% smoke-free environments, including ventilation, air filtration and designated smoking areas, have repeatedly been shown to be ineffective.39
Fourth, rebuilding of the administrative power structure is essential to protect tobacco control measures from interference by the tobacco industry. Each of the countries examined in the present study has a substantially state-owned tobacco company. The three counties have a history of promoting the tobacco industry as a national policy; each country has a legislative system to manage tobacco cultivation, production and sales. The Ministry of Finance of each country has authority over the whole industry. As previously reported for Japan,61 the tobacco industry in these countries is able to interfere in the drafting of new policies. The tobacco companies also promote a clean image of their activities through large-scale media campaigns, which counter efforts to denormalise the industry. However, in each country, government does hold majority control over the tobacco industry. Therefore, with sufficient political will it would be possible to use existing policy instruments to develop and implement long-term plans for reducing tobacco consumption and transforming the tobacco business. The three East Asian countries need to restructure their administrative frameworks, historically established to foster the tobacco industry, with the aim of improving their citizens’ health.
A model in East Asia is Taiwan. The tobacco epidemic situation in Taiwan is similar to those in the three countries analysed. A large-scale survey in Taiwan indicated that the smoking prevalence is higher among men than among women, and that low quit rates among men and the high exposure to passive smoking among women and young children at home are of particular concern.62 However, the Taiwanese government passed the Tobacco Hazard Prevention Act in 1997, through which indoor places became partially smoke free. In 2002, the government started the Outpatient Smoking Cessation Services programme, and levied a health and welfare surcharge on each pack of cigarettes.63 Amendment of the Act in 2009 strengthened the legislation by extending smoke-free areas to almost all enclosed workplaces and public places, adding graphic health warnings to cigarette packages, and totally banning tobacco advertising, promotion, and sponsorship as recommended by the FCTC.63
East Asian collaboration
Japan, China and South Korea have similarities in many aspects of their tobacco control efforts, suggesting the potential for policy coordination among these three countries in prioritising issues and target setting. The tobacco market in Taiwan was opened in 1987 and that in South Korea in 1988. Since then, JT has gained a considerable market share in Taiwan and South Korea.64 China joined the World Trade Organisation in 2001 and the China National Tobacco Corporation has since made inroads into overseas markets. In anticipation of the possible cigarette market opening of mainland China, JT is now developing a plan to form an alliance with the Chinese tobacco industry.65 For the public health of the East Asian region, collaboration has been promoted on a research basis,66 ,67 but not sufficiently in terms of policy development and advocacy efforts. The FCTC Parties’ reports showed that Japan, China and South Korea had been inactive in collaborating with each other.46–48 To take action against tobacco industry activities that extend beyond national boundaries, international collaboration is essential,68 from global and local perspectives.
Limitations
This study has several limitations. First, not all of the survey data were up to date or nationally representative. Second, the surveillance period and definitions of evaluated items were not necessarily consistent between countries. Not all of our arguments can be fully supported by quantitative data, particularly regarding the tobacco industry interference in government policies. Finally, we did not fully analyse the background and/or historical factors affecting the current situation in the three countries. Future research should explore why the observed similarities and differences exist.
Conclusion
Our analysis of quantitative data and information obtained from international and domestic sources indicates an urgent need for the following set of tobacco control policies in East Asia: raising cigarette prices in combination with media campaigns targeting adult men; developing a multi-component quitting assistance system that includes telephone support and provides free cessation drugs; legislation for smoke-free workplaces and public places; and rebuilding the administrative structure to protect proposed measures from tobacco industry interference. The importance of these four approaches should be reaffirmed by all policymakers in East Asia.
Key messages
-
East Asia is one of the world’s largest tobacco epidemic regions.
-
Our analysis indicates an urgent need for the following policies: raising cigarette prices in combination with media campaigns targeting adult males; developing a multi-component quitting assistance system that includes telephone support and provides free cessation drugs; legislating smokefree workplaces and public places; and rebuilding the administrative structure to protect proposed measures from tobacco industry interference.
-
The importance of these standard approaches should be reaffirmed by all policy makers in East Asia.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Contributors KK collected Japanese data, analysed all the data, and wrote the manuscript. JY collected Chinese data, SP and MKL collected South Korean data, and YLQ and MI organised the research group and provided overall discussion.
-
Funding This work was supported by grants-in-aid for the Third-Term Comprehensive Ten-Year Strategy for Cancer Control from the Ministry of Health, Labour, and Welfare, Japan (grant numbers: 201118014, 201220044).
-
Competing interests None.
-
Provenance and peer review Not commissioned; internally peer reviewed.