Article Text

Abstract
Background In 2009, China changed its health warnings on cigarette packs from side-only text warnings to two text-only warnings on 30% of the bottom of the front and back of the pack. Also in 2009, Malaysia changed from similar text warnings to pictorial health warnings consistent with Framework Convention on Tobacco Control (FCTC) Article 11 Guidelines.
Objective To measure the impact of the change in health warnings in China and to compare the text-only health warnings to the impact of the pictorial health warnings introduced in Malaysia.
Methods We measured changes in key indicators of warning effectiveness among a longitudinal cohort sample of smokers from Waves 1 to 3 (2006–2009) of the International Tobacco Control (ITC) China Survey and from Waves 3 to 4 (2008–2009) of the ITC Malaysia Survey. Each cohort consisted of representative samples of adult (≥18 years) smokers from six cities in China (n=6575) and from a national sample in Malaysia (n=2883). Generalised Estimating Equations (GEE) were used to examine the impact of the health warnings on subsequent changes in salience of warnings, cognitive and behavioural outcomes.
Findings Compared to Malaysia, the weak text-only warning labels in China led to a significant change in only two of six key indicators of health warning effectiveness: forgoing cigarettes and reading the warning labels. The change to pictorial health warnings in Malaysia led to significant and substantial increases in five of six indicators (noticing, reading, forgoing, avoiding, thinking about quitting).
Conclusions The delay in implementing pictorial health warnings in China constitutes a lost opportunity for increasing knowledge and awareness of the harms of cigarettes, and for motivating smokers to quit.
- Packaging and Labelling
- Low/Middle income country
- Global health
Statistics from Altmetric.com
Introduction
Approximately 300 million people smoke cigarettes in China including 52.4% of men and 2.3% of women.1 Tobacco-related diseases including cancer, stroke and chronic obstructive pulmonary disease (emphysema, chronic bronchitis), kill 1.4 million people in China each year2 and this number is expected to rise to more than 5 million by 2050 if current rates continue. The precipitous rise in tobacco-related illness and death in China is contrasted by the limited impact of tobacco control policies in China to date.3
Increasing knowledge and awareness of the harms of cigarettes is a key objective for tobacco control. Although such knowledge has increased in China,2 there remain substantial gaps among Chinese smokers in knowledge of the major health consequences of smoking. For example, findings from the 2009–2010 International Tobacco Control (ITC) China Survey indicate that only 36% of Chinese smokers knew that smoking is a cause of heart disease and 16% knew that smoking causes stroke,4 the lowest levels among 18 ITC countries.5 Similar findings have emerged from the 2010 Global Adult Tobacco Survey (GATS) in China.6
Health warnings constitute a powerful intervention for increasing knowledge about the specific harms of tobacco use7 and for increasing thoughts and motivations to quit smoking among smokers in many countries including Thailand, Malaysia, Uruguay, Mauritius, Mexico, Australia and Canada.8–14 Health warnings also have the potential to prevent smoking initiation among non-smokers, including youth.15 Smokers rate health warnings on cigarette packages as a prominent and credible source of information about the harms of tobacco use.7 Further research has demonstrated that pictorial health warnings are more effective than text-only health warnings.16–19
In 2005, China ratified the WHO's Framework Convention on Tobacco Control (FCTC) which came into force in 2006. Under FCTC Article 11, China was obligated to implement health warnings that occupied at least 30% at the top of the front and back of cigarette packages. At the time of the FCTC ratification, China had a small text-only warning located on the side of the package. In October 2008, China announced that it would change its warnings to text-only warnings that would occupy 30% of the bottom of the front and back of all cigarette packages (see Figure 1). These new warnings met the minimum standards of the FCTC treaty text, but did not meet the Article 11 Guidelines,20 which called for Parties to implement pictorial health warnings on at least 50% of the top of the front and back of the package. These Guidelines were adopted at the Third Conference of the Parties in November 2008, 1 month after China's announcement of the text-only revision of their warnings.
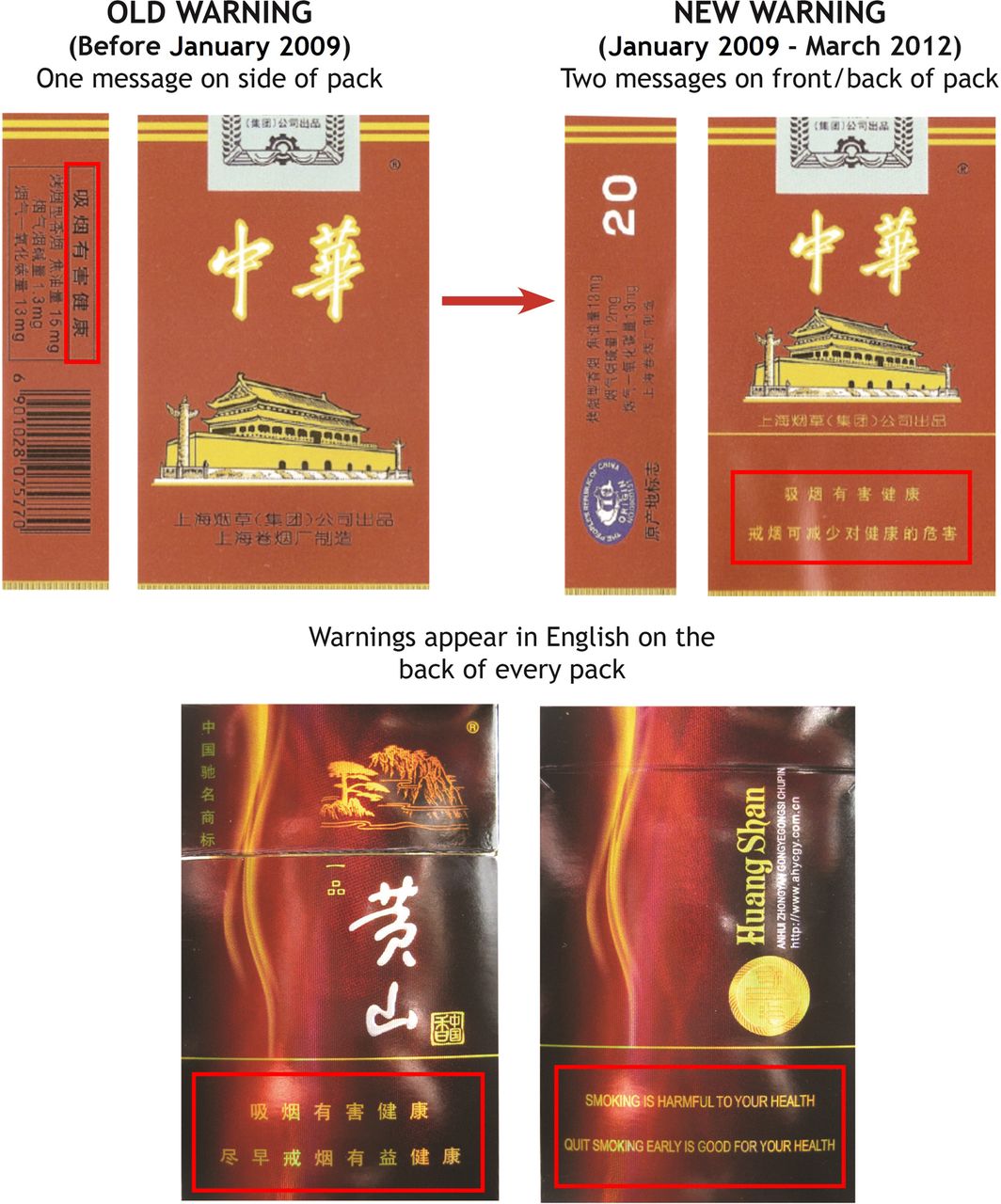
The text-only change in China's health warnings, announced October 2008 and implemented January 2009.
A few studies have suggested that the new warning labels would not be effective. A convenience sample survey of Chinese adult smokers and non-smokers in Jiangsu province found that few respondents thought that the new warning labels provided adequate information about the health risks of smoking, and few respondents indicated that the new warning labels would made them think about quitting smoking.21 An experimental study of smokers and non-smokers in four Chinese cities found that the warning labels were not effective in motivating smokers to quit and convincing youth not to start smoking. The study also found that picture warnings were rated as more effective.16
The present study is the first representative cohort survey to evaluate the impact of the 2009 text-only change in health warnings in China. Data are from the ITC China Survey, a longitudinal cohort survey of smokers in six cities (Beijing, Shenyang, Shanghai, Changsha, Guangzhou and Yinchuan). In addition, we compare the impact of the text-only revision in China with Malaysia, which had health warnings similar to China (text-only on the side of the pack), but instead introduced pictorial health warnings consistent with the FCTC Article 11 Guidelines. Malaysia's pictorial health warnings implemented in June 2009, consisted of six rotating images printed in Malay and English, covering 40% of the front and 60% of the back of all cigarette packages.
Past quasi-experimental evaluations of warnings by the ITC Project have compared pictorial revisions in one country to another ‘control’ country whose warnings did not change over the same period of time—a kind of ‘no-treatment control’. However, in the present study, both countries started with the same warnings and each implemented a different intervention. The fact that both countries implemented an intervention controls for the possibility that any significant increases in warning effectiveness after pictorial health warnings were introduced might be due in part to novelty effects. A further advantage of the comparison between Malaysia and China is that the difference between the effect size achieved by the Malaysian pictorial revision and the effect size achieved by the Chinese text-only revision can be used to estimate what China lost in effectiveness in their decision to implement text-only warnings rather than pictorial health warnings, a strategy that is much less appropriate when one of the countries did not change its warnings at all.
Methods
Data and sample design for China
The data was collected from six cities in the first three waves of the ITC China Survey. Wave 1 (conducted between April and August 2006) and Wave 2 (October 2007 to January 2008) data were collected prior to the implementation of the new health warnings, and Wave 3 data collection (May to October 2009) was conducted after the January 2009 health warnings were implemented.
At Wave 1, a multistage cluster sampling design was used to select a representative sample of 800 smokers and 200 non-smokers in each city. Participants were recontacted and interviewed again whenever possible in each subsequent wave. To maintain the sample size over time, respondents lost to attrition were replaced in the subsequent waves using the same sampling frame constructed in Wave 1. A total of 6513 smokers participated in at least one of the three waves. Participation by survey wave is presented in Table 1. The retention rates for Waves 2 and 3 were 81.6% and 80.4%. To measure the impact of the health warnings on smokers, we limited the sample to current smokers (had smoked at least 100 cigarettes in their lifetime and are currently smoking at least once a week). Detailed descriptions of the methodology and sampling design of the ITC China Survey are given in Wu et al.22 ,23
Sample characteristics at recruitment in China and Malaysia
Survey methods used in Malaysia
The results of the pre- and post-implementation of pictorial health warnings in Malaysia came from a cohort of 2883 adult smokers (selected using a stratified multistage sampling design) who had participated in Wave 3 to Wave 4 of the ITC Surveys in Malaysia. The retention rate from Wave 3 to Wave 4 was 61%. Wave 3 was conducted between February and September 2008, five months before the implementation of pictorial health warnings. The majority of adult interviews in Wave 3 were conducted by telephone and remaining interviews were face-to-face. Wave 4 was conducted by telephone between July and November 2009, seven months after the implementation of pictorial health warnings. The survey methods are described in greater detail by Yong et al8 and the ITC Malaysia National Report.10
Measures
Health warning effectiveness
The present study employed six measures that have been identified as key indicators of warning effectiveness in the International Agency of Research on Cancer (IARC) Cancer Prevention Handbook, Methods for Evaluating Tobacco Control Policies.24 The measures described below were used in China and Malaysia unless otherwise stated.
Health warning salience was measured by two questions: (1) ‘In the past month, how often, if at all, have you NOTICED health warnings on cigarette packages?’; and (2) ‘In the past month, how often, if at all, have you read or looked closely at the health warnings on cigarette packages’. Responses (‘never’, ‘once in a while’, or ‘often’, and in Malaysia only ‘very often’) were dichotomised where 0=‘never or once in a while’ and 1=‘often/very often’. Only respondents who reported having noticed the health warnings at least ‘once in a while’ were included in the analyses for the subsequent five indicators.
Cognitive reactions were measured by two questions: (1) ‘To what extent, if at all, do the health warnings on cigarette packs make you more likely to think about the health risks (health danger) of smoking?’; and (b) ‘To what extent, if at all, do the health warnings on cigarette packs make you more likely to quit smoking?’i Response options (‘not at all’, ‘a little’ or ‘a lot’) were dichotomised where 0=‘not at all/a little’ and 1=‘a lot’.
Behavioural reactions were measured by two questions: (1) Forgoing: ‘In the past month, have the warning labels stopped you from having a cigarette when you were about to smoke one?’ Response options (‘never’, ‘once’, ‘a few times’ or ‘many times’) were dichotomised where 0=‘ never’ and 1=‘once/a few times/many times’; and (2) Avoidance: ‘In the past month, have you made any effort to avoid looking at or thinking about the warning labels?’ Response options were 0=‘no/don't care about the health warning’ or 1=‘yes’.
Support for more health information on warning labels Support for more health information on warning labels post implementation of the new health warnings was assessed at Wave 3. Respondents in China were asked ‘Do you think that cigarette packages should have more health information than they do now, less, or about the same amount as they do now?’ Response options were ‘less health information,’ ‘about the same,’ or ‘more health information’.
Demographics
Demographic variables included in the analyses were: gender, age (18–24, 25–39, 40–54, 55+), education level (China: low=no schooling/primary education only, moderate=secondary school, high=college or university education; Malaysia: low=no schooling/elementary, moderate=secondary/preuniversity/diploma, certificate, high=Bachelor degree and higher) and monthly household income (China: low=less than 1000 Yuan, medium=1000–3000 Yuan, high=3000+ Yuan; Malaysia: low=lower tertile of per capita annual household income, medium=middle tertile of per capita annual household income, high=higher tertile of per capita annual household income).
Smoking behaviours
Smoking behaviours were measured by four indicators: number of cigarettes smoked per day (CPD; 0–11, 11–20, 21–30, or over 30); time to first cigarette after waking up in minutes (<6, 6–30, 31–60, >60); and smoking status (daily/non-daily smokers). Intention to quit smoking (within the next month, within the next 6 months, beyond 6 months or no plan to quit, not stated) was coded as ‘yes’ if the respondent had any intention to quit, ‘no’ if the respondent had no plan to quit, and ‘not stated’ if the respondent did not provide a response.
Time in sample
Participants in the analyses were recruited at three different survey waves; therefore, a time-in-sample variable was constructed as number of waves since recruitment. Assuming that the impact of time-in-sample was non-linear, the variable is treated as a categorical variable.
Data analysis
The SAS callable SUDAAN (V.11) was used for all analyses. The prevalence of warning effectiveness was calculated at each wave using Generalised Estimating Equations (GEE).25 The six indicators of warning effectiveness are binary; thus, GEE models with the logit link were applied. The prevalence of support for stronger warnings at Wave 3 in China was calculated using a multinomial logit model. All analyses controlled for gender, age, income, education level, CPD, time to first cigarette, intention to quit, smoking status (daily/weekly) and time in sample. In China the analyses also controlled for city to reduce the sampling design effect. This was not necessary in Malaysia given its different sampling design frame. To accommodate a potential design effect resulting from the complex longitudinal survey design and within-individual correlations due to repeated measures at each wave, a nested structure that includes the strata (cities in China, states in Malaysia), the primary sampling units (neighbourhood or Ju Wei Hui in China, districts in Malaysia) and the respondent IDs (with repeated measures at each wave) were used to construct the models and the rescaled cross-sectional weights at recruitment were applied for each respondent. To detect significant changes in prevalence between Waves 2 and 3 in China and between Waves 3 and 4 in Malaysia for each of the six health warning effectiveness indicators, the data from both countries were combined and analyses used the same GEE logit model as above. The pred_eff statement in the model was applied to conduct the significance tests of the marginal per cent changes between countries and between waves. All CIs and statistical significance were tested at the 95% confidence level.
Results
Sample characteristics
Table 1 presents the sample characteristics for the ITC China Survey and ITC Malaysia Surveys at the recruitment wave for each respondent. Most smokers were male (94.6% in China and 98.8% in Malaysia), smoked daily (93.6% in China and 93.8% in Malaysia) and had no quit intentions (74% in China and 79% in Malaysia).
Changes in health warning effectiveness prior to new health warning introduction in China (Wave 1 to Wave 2)
Figure 2 presents the pattern over time for the six indicators of health warning effectiveness in China. Waves 1 and 2 were conducted prior to the January 2009 text-only health warnings change, and Wave 3 was post-health warning change. There were significant changes prior to the new health warning introduction (Wave 1 to Wave 2) in noticing (p<0.001) and reading (p=0.002) the health warnings. The percentage of smokers that ‘often’ noticed the health warnings decreased from 51.6% to 40.4% and the percentage of smokers that ‘often’ read or looked closely at the health warnings decreased from 29.1% to 19.8%. There were no significant changes for any of the other four measures between Waves 1 and 2.

Impact of the 2009 health warning policy change on smokers’ perceptions and behaviours in the past month, International Tobacco Control (ITC) China Survey Waves 1–3.
Impact of the 2009 health warning policy change in China (Wave 2 to Wave 3)
To measure the impact of the introduction of the new health warnings in China, we examined changes in cognitive and behavioural responses among smokers between Wave 2 (prehealth warning change) and Wave 3 (post-health warning change). There was a significant increase in forgoing cigarettes: the percentage of smokers that reported the health warnings had stopped them from having a cigarette increased from 19.7% at Wave 2 to 26.8% at Wave 3 (p=0.002). There were no significant changes on any of the remaining five measures: the percentage of smokers that ‘often’ noticed health warnings (40.4–43.1%), the percentage who ‘often’ read or looked closely at the health warnings (19.8–23.4%), who made an effort to avoid looking at or thinking about the health warnings (12.8–14.4%) and who reported the health warnings made them more likely to quit smoking (4.9–6.5%). There was no change in the percentage of smokers reporting that the health warnings on cigarette packs made them more likely to think about the health risks of smoking (8.1% each wave).
Comparison of health warning changes between China and Malaysia
The comparison of the China text-only warning change to the Malaysia text to pictorial health warnings change for each of the six indicators of health warning effectiveness are presented in Figure 3A–F. These pooled analyses are different from the previous analyses because they are based on the pooled data for both China and Malaysia and therefore represent the average population composition of the two countries. In these analyses, forgoing cigarettes (p<0.001) and reading health warnings (p=0.02) increased significantly in China following the introduction of the health warnings. In Malaysia, five out of six measures of health warning impact increased significantly between Waves 3 and 4. There were significant increases in noticing the warnings (p<0.001), reading the health warnings closely (p<0.001), forgoing cigarettes (p<0.001), avoiding thinking about the health warnings (p=0.005) and in the percentage of smokers reporting that the health warnings made them ‘a lot’ more likely to quit smoking (p<0.001). Increases in thinking about the health risks of smoking ‘a lot’ (p=0.10) was not statistically significant.

(A–F) Impact of Health Warning Changes in China (Waves 2–3) and Malaysia (Waves 3–4).
Figure 3 shows that there was a significant impact of the warning labels in Malaysia compared to China for every variable except thinking about the health risks of smoking. The percentage of smokers who noticed the health warnings ‘often’ or ‘very often’ in Malaysia increased from 54.4% to 67% after the pictorial health warnings were introduced, an increase of 12.6%. In contrast, in China the percentage who noticed the warnings ‘often’ increased from 41.6% to 44.7%, an increase of only 3.1%. The net difference between Malaysia and China was 9.5% (p=0.02). Similarly, the net difference was 8.4% for reading or looking closely at the warnings (p=0.04; Figure 3B), 4.4% for thinking about the health risks of smoking (p=0.13; Figure 3C), 7.7% for health warnings making you more likely to quit smoking (p<0.001; Figure 3D), 17.6% for forgoing a cigarette (p<0.001; Figure 3E) and 6.4% for avoiding looking at or thinking about the health warnings p=0.02 (Figure 3F).
Support for more health information on warning labels among smokers in China
In Wave 3, 41% of Chinese smokers said they wanted more health information and 52% said they wanted the same amount of health information on cigarette packages. Only 7.1% of smokers indicated that they wanted less health information.
Discussion
This is the first longitudinal cohort study of a representative sample of adult smokers to evaluate the impact of enhanced text-only health warnings in China. The results demonstrate that the change in text-only warnings on the side to text warnings on 30% of the front and back of the package was minimally effective. A statistically significant change was observed for only two of six key indicators of warning effectiveness (forgoing cigarettes, reading the warning labels) in our pooled analysis compared to Malaysia. There were no other statistically significant changes in any of the five remaining indicators.
The comparison in health warning effectiveness between China and Malaysia, however, demonstrates both the greater effectiveness of pictorial health warnings over text warnings and the missed opportunity to implement effective health warnings in China. Malaysia started off with the same text-only health warnings on the side of the package as China. In 2009, Malaysia introduced pictorial health warnings on the cigarette pack in compliance with the Article 11 FCTC Guidelines whereas China introduced the minimum standard text-based health warnings on 30% of the pack. For every measure of health warning effectiveness, the impact of the new Malaysian pictorial health warnings was greater than that of the new text-only health warnings in China. The Malaysia health warnings demonstrated substantial increases in health warning effectiveness with significant changes in five of six outcomes.
We estimated the magnitude of China's decision to implement text-only rather than pictorial health warnings by calculating the net difference in effect sizes and multiplying by the number of smokers in China. For example, the text-only revision in China led to an increase of 3.1% of smokers who reported noticing the warnings ‘often’. However, the pictorial revision in Malaysia let to a 12.6% increase in noticing. The 9.5% net difference×300 million smokers=28.5 million smokers. This huge number represents the lost opportunity—the estimated number of additional Chinese smokers who would have noticed the warnings if China had implemented pictorial health warnings rather than text-only warnings.
Using the same estimation method for the other key indicators yields these significant numbers: If China had implemented Malaysia-style pictorial health warnings, 25.2 million more Chinese smokers would have read the warnings, 13.2 million more smokers would have reported that the warnings made them think about the health risks of smoking, 23.1 million more smokers would have reported that the warnings made them think about quitting, 52.8 million more smokers would have reported that the warnings stopped them from smoking a cigarette, and 19.2 million more smokers would have reported that they had taken steps to avoid the warnings.
It is clear that the Chinese text-only warnings continue to be a lost opportunity for increasing the knowledge and awareness of the specific harms of cigarettes among the 300 million smokers in China as well as the many millions of youth who are not yet smokers, but who, with appropriate education, could avoid the uptake of the consumption of a product that kills over half of its regular long-term users.
The implementation of Article 11 Guidelines in China has always been under the direct control of the Ministry of Industry and Information Technology (MIIT). The State Tobacco Monopoly Administration (STMA) is part of MIIT and plays a key role in the implementation of the FCTC in China. STMA and the China National Tobacco Corporation (CNTC) are closely connected, sharing the same set of personnel, line of command and office. In China, tobacco control and the tobacco market are essentially run by the same organisation.26 The structural problems arising from CNTC being regulated by STMA have been well-documented.2 ,27
In addition to using text-based rather than pictorial health warnings and covering only 30% of the package, the China health warnings fail to meet other aspects of the FCTC Article 11 Guidelines, as shown in Figure 4. For example, the Guidelines call for multiple warning messages, but the two health warning messages introduced in 2009 are essentially the same message framed in slightly different ways: ‘smoking is harmful to your health’, and ‘quit smoking reduces health risk’. The Guidelines also call for rotation of the warnings. Indeed, the 2009 warnings had a message that was rotated but was not meaningful, as it rotated from ‘quitting smoking reduces health risk’ to ‘quit smoking early is good for your health’, which is again essentially the same message. The English warnings are presented verbatim (the warnings include a grammatical error).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of China's 2009 text-only warnings to the standards of the Framework Convention on Tobacco Control (FCTC).
Article 11 guidelines
Article 11 also specifies that warnings should be in the country's principal language. Although the 2009 health warnings did appear on the front and back of the package, the warning on the back was presented in English until April 2012. Among 1169 smokers across four cities in China, Fong et al16 found that only 26.8% of adult smokers could translate ‘Smoking is harmful to your health’ and only 10.1% could translate ‘Quit smoking early is good for your health’ into Chinese.
Facing the increasing pressure calling for the full implementation of the FCTC Article 11 Guidelines, in April 2012, CNTC self-imposed two minor enhancements to the 2009 health warning: replacing the English warning on the back of the pack with Chinese and the minimum text font size was increased to 4 mm.28 CNTC was willing to increase the size of the text and the display area, but was unwilling to introduce pictorial health warnings.
Recently, there have been positive developments in tobacco control policies in China. In November 2014, China's State Council issued a draft regulation on ‘Smoking Control in Public Places’ which calls for a comprehensive ban on smoking in all public places, workplaces and public transportation. The draft regulation also requires tobacco product manufacturers to print both text and pictorial health warnings of no smaller than half of the area of the package that state specific harms of tobacco use on tobacco packages. Thus, the Chinese government has indicated their intention to meet their obligations under the FCTC for pictorial health warnings. The current study clearly shows that smokers are supportive of putting more health information on cigarette packages.
It remains to be seen whether pictorial health warnings will indeed appear on Chinese packs, and if so, whether they will meet the Article 11 Guidelines. Given the weak implementation of the text-only warnings whose corresponding weak impact has been documented in this study, and the existing structural problems in FCTC implementation in China, it is difficult to be optimistic.
Limitations
This study has several limitations. The study sample came from residents living in the well-developed urban areas of the large cities in China. The findings are therefore not generalisable to the Chinese population living in underdeveloped rural areas or small cities. The measures used were self-reported, which may be subject to response bias. The timing of the follow-up survey differed between China and Malaysia. To test whether the length of exposure to the warning labels could account for the differences in our outcomes, we conducted a separate analysis restricting our data to the same follow-up time period for both countries. Results were consistent with the reported findings. Comparisons between China and Malaysia were based on pooled analyses with standard covariates to control for differences in sociodemographic and tobacco use characteristics. However, these countries have different cultures which may limit the estimates of the effectiveness of the different types of warning labels. The current study evaluates the impact of the warning labels in China. The warning labels in China were not only weak because they were text only but they were also potentially weaker because they were smaller in size, lacked a contrasting background, were weakly worded, had minimal rotation and had few messages. Therefore, this study is not able to provide a direct comparison of the impact of text versus pictorial warning labels generally.
Conclusions
These findings demonstrate that the text-only health warning in China did not lead to significant changes in most of the key indicators of health warning effectiveness. A comparison with Malaysia which began with the same text-only health warnings but then introduced pictorial health warnings demonstrates the potential impact that pictorial health warnings could have in China.
What this paper adds
The 2009 enhancement of the text-only health warnings in China was weak, was not compliant with the Framework Convention on Tobacco Control (FCTC) Article 11 Guidelines and did not lead to significant changes in the indicators of health warning effectiveness.
In contrast, Malaysia, which began with the same text-only warnings on the side of the pack as China did, showed substantial increases in the measures of warning effectiveness after implementing pictorial health warnings on the cigarette packages in compliance with Article 11 Guidelines.
The contrast between China and Malaysia demonstrates both the power of well-designed pictorial health warnings as well as what could be achieved if pictorial health warnings are implemented in China.
Acknowledgments
The authors thank the Chinese Center for Disease and Prevention and the Beijing, Shanghai, Shenyang, Guangzhou, Changsha and Yinchuan CDCs for collecting and cleaning the data set, Dr Susan C Kaai for brainstorming about the interpretation of the research findings, Ms Dana Komer for editing the first draft and Mi Yan for her assistance with the initial draft. The authors thank Sue Steinback for her assistance with referencing.
References
Footnotes
Contributors TEM and GTF designed the study and defined the research methodology and analysis. TEM, GTF and SSW conducted the literature review and drafted the manuscript. GM conducted the data analysis. GM, ACKQ, GS, GF and YJ helped to interpret the analytical results and revised the draft. The final version of this paper has been reviewed and approved by all coauthors.
Funding The ITC China Project was supported by grants from the US National Cancer Institute (R01 CA125116 and P01 CA138389), the Roswell Park Transdisciplinary Tobacco Use Research Center (P50 CA111236), the Robert Wood Johnson Foundation (045734); the Canadian Institutes of Health Research (57897, 79551 and 115016), and the Chinese Center for Disease Control and Prevention. Additional support was provided to Geoffrey T Fong from a Senior Investigator Award from the Ontario Institute for Cancer Research and a Prevention Scientist Award from the Canadian Cancer Society Research Institute.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics approval was obtained from the Office of Research at the University of Waterloo (Waterloo, Canada) and the Institutional Review Boards at the Roswell Park Cancer Institute (Buffalo, USA), the Cancer Council Victoria (Victoria, Australia), and the Chinese Center for Disease Control and Prevention (Beijing, China).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from the International Tobacco Control Policy Evaluation (ITC) Project are available to approved researchers 2 years after the date of issuance of cleaned data sets by the ITC Data Management Centre. Researchers interested in using ITC data are required to apply for approval by submitting an International Tobacco Control Data Repository (ITCDR) request application and subsequently to sign an ITCDR Data Usage Agreement. To avoid any real, potential, or perceived conflict of interest between researchers using ITC data and tobacco-related entities, no ITCDR data will be provided directly or indirectly to any researcher, institution, or consultant that is in current receipt of any grant monies or in-kind contribution from any tobacco manufacturer, distributor, or other tobacco-related entity. The criteria for data usage approval and the contents of the Data Usage Agreement are described online (http://www.itcproject.org).
↵i In China Waves 2–3 “health warnings” was replaced by “warning labels” for this measure.