Article Text

Abstract
Background Heated tobacco products (also called ‘heat-not-burn’ products) heat tobacco at temperatures below that of combustion, causing nicotine and other compounds to aerosolise. One such product, IQOS from Philip Morris International, is being marketed internationally with claims of harm reduction. We sought to determine whether exposure to IQOS aerosol impairs arterial flow-mediated dilation (FMD), a measure of vascular endothelial function that is impaired by tobacco smoke.
Methods We exposed anaesthetised rats (n=8/group) via nose cone to IQOS aerosol from single HeatSticks, mainstream smoke from single Marlboro Red cigarettes or clean air for a series of consecutive 30 s cycles over 1.5–5 min. Each cycle consisted of 15 or 5 s of exposure followed by removal from the nose cone. We measured pre-exposure and postexposure FMD, and postexposure serum nicotine and cotinine.
Results FMD was impaired comparably by ten 15 s exposures and ten 5 s exposures to IQOS aerosol and to cigarette smoke, but not by clean air. Serum nicotine levels were similar to plasma levels after humans have smoked one cigarette, confirming that exposure conditions had real-world relevance. Postexposure nicotine levels were ~4.5-fold higher in rats exposed to IQOS than to cigarettes, despite nicotine being measured in the IQOS aerosol at ~63% the amount measured in smoke. When IQOS exposure was briefer, leading to comparable serum nicotine levels to the cigarette group, FMD was still comparably impaired.
Conclusions Acute exposures to IQOS aerosol impairs FMD in rats. IQOS use does not necessarily avoid the adverse cardiovascular effects of smoking cigarettes.
- non-cigarette tobacco products
- electronic nicotine delivery devices
- harm reduction
- nicotine
- smoking caused disease
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- non-cigarette tobacco products
- electronic nicotine delivery devices
- harm reduction
- nicotine
- smoking caused disease
Introduction
Heated tobacco products (also called ‘heat-not-burn’ tobacco products) heat tobacco at temperatures that avoid combustion but cause the nicotine to aerosolise. Philip Morris International’s (PMI’s) heated tobacco product IQOS is now marketed in at least 30 non-US countries and has been considerably more successful than similar products introduced at various times over the last three decades.1 In 2017, Philip Morris Products S.A. submitted modified-risk tobacco product (MRTP) applications to the FDA to market IQOS in the USA with reduced risk claims.2
IQOS is composed of three main parts: HeatStick, holder and pocket charger (figure 1). HeatSticks, which contain long strips of processed and reformed tobacco packed together (figure 1), are inserted in the holder for use. The holder contains an electronic heating blade that is activated by pressing a side button on the holder and heats the mixture of tobacco and other compounds in the HeatSticks to 350°C. Aerosol is generated as the user inhales through the HeatStick/holder combination.

IQOS. IQOS is composed of three main parts: HeatStick, holder and pocket charger. HeatSticks are inserted in the holder, which contains an electronic heating blade to heat tobacco and release aerosol. HeatSticks contain strips of processed and reformed tobacco. Photos by MLS and PN.
Despite harm reduction claims by the tobacco industry and the clinical and basic research reported by PMI researchers,3–23 the cardiovascular health effects of IQOS and similar products are incompletely understood. Notably, industry-supported studies of potential cardiovascular consequences of IQOS aerosol exposure published to date have not included some common measures of adverse effects of smoke exposure, such as vascular endothelial function tested in vivo. As IQOS has been marketed widely, it is important to study the health effects of this product so that regulatory agencies such as the FDA and consumers can make informed decisions.
Endothelial function assessed by arterial flow-mediated dilation (FMD) is a validated measure of cardiovascular health effects and is defined as the per cent by which the arteries vasodilate in response to an increase in blood flow.24 Endothelial cells lining the vessel sense increases in flow and respond by producing nitric oxide, which triggers the artery to grow in diameter to accommodate the increased demand. In humans, FMD is determined by temporarily interrupting and restoring blood flow to the forearm, and using ultrasound to measure the increase in brachial artery diameter caused by the resulting sudden increase in flow. FMD is a clinical prognostic indicator of endothelial function and cardiovascular health.25–27 Acute and chronic exposures to secondhand smoke and active smoking impair FMD in humans.28–31 While such studies have typically focused on exposure to smoke, one group has reported that exposure to e-cigarette aerosol can impair FMD,32 raising the possibility that this effect is not limited to smoke from combustion and suggesting that inhalation of other non-combustible tobacco products may also have similar consequences.
We previously developed and validated an in vivo rat model for FMD measurements using high-resolution ultrasound and microsurgical techniques.33 We showed that exposure of rats to sidestream smoke (from the smouldering tip; an accepted approximation of secondhand smoke) of cigarettes, little cigars and marijuana impairs FMD in an endothelium-dependent manner (endothelium-independent vasodilation induced by nitroglycerin is not impaired).34–36 The consistent responses of humans and rats to smoke and non-combustion aerosols from multiple sources led us to hypothesise that IQOS aerosol can similarly cause endothelial dysfunction. We report here that exposure to IQOS aerosol impairs FMD to the same extent as mainstream cigarette smoke.
Materials and methods
Animals
We used male Sprague-Dawley rats (Charles River, MI) at 8–10 weeks of age with body weights of 200–250 g as has been the standard condition for our previous studies on smoke exposure. Rats were anaesthetised with intraperitoneal injection of ketamine (100 mg/kg)/xylazine (5 mg/kg) for these experiments. During all procedures, rats were kept on a heating pad to prevent hypothermia. Frequency and depth of respiration were closely monitored to ensure full anaesthesia and supplemental intraperitoneal (IP) anaesthetic was given if necessary.
Mainstream smoke/aerosol generation and exposure
Russian IQOS Parliament branded HeatSticks and an IQOS device from Ukraine were used for the first part of the project. Due to heating blade breaking incidences during cleaning, IQOS devices obtained from Japan and subsequently from South Korea were used for later exposures.
We exposed rats (n=8/group) via nose cone to IQOS aerosol, Marlboro cigarette mainstream smoke or clean air as control. The exposure regimen consisted of a series of consecutive 30 s cycles, each consisting of 15 or 5 s of exposure followed by removal of the nose cone for the rest of the 30 s interval. Each rat was exposed to either 10 cycles over 5 min or 3 cycles over 1.5 min, depending on the experiment, to approximate the consumption of a single IQOS HeatStick or less. To generate the aerosol and mainstream smoke, we used a manual syringe pump system for the initial experiment and then purchased a Gram Universal Vaping Machine version 5.0 (Gram Research, Oakland, California, USA) for the subsequent experiments (figure 2). The vaping machine contains an automatic syringe pump and has been shown to reproducibly generate aerosols from e-cigarettes under controlled conditions.37 Both systems generated 35 mL of aerosol over 2 s and the vents on the side of the cigarette filters remained unoccluded. Separate sets of syringe pump, nose cone and connecting tubes and valves were used to avoid cross-contamination. The IQOS holder was fully cleaned and recharged after each use.

Aerosol generation and exposure systems. (A) Manual exposure system. (B) Analytical vaping machine made by Gram Research. (C) IQOS aerosol coming out of nose cone. (D) Rat’s nose placed in the nose cone. Photos in A, C and D by PN; photo in B from Gram Research with permission.
Endothelial function measurements
We used our previously established living rat model33 to measure FMD before and after each exposure in individual animals.
We made a 1 cm incision on the rat’s groin and surgically dissected around the common iliac artery. We then placed an arterial loop occluder consisting of a 5–0 Prolene filament under the artery and passed it through a 15 cm PE–90 tubing to enable transient occlusion of blood flow after suturing the skin. A series of diameter images of the femoral artery and accompanying Doppler blood flow images were recorded with a 35 MHz ultrasound transducer (Vevo660; VisualSonics, Toronto, Canada) before transient surgical occlusion at baseline. We induced a transient limb ischaemia for 5 min and obtained ultrasound imaging immediately after reperfusion, and then every 30 s for 5 min.
We used an automated program (Brachial Analyzer 5; Medical Imaging Applications, Coralville, Iowa, USA) to measure baseline artery diameter and peak postischaemia diameter during diastole. FMD was calculated as the per cent increase in the diameter of the artery after the transient ischaemia. FMD was measured before and after exposures to smoke or IQOS aerosol, as summarised schematically in figure 3A,B. The investigator was blinded to exposure conditions during FMD procedure, analysis of ultrasound images and subsequent calculations.

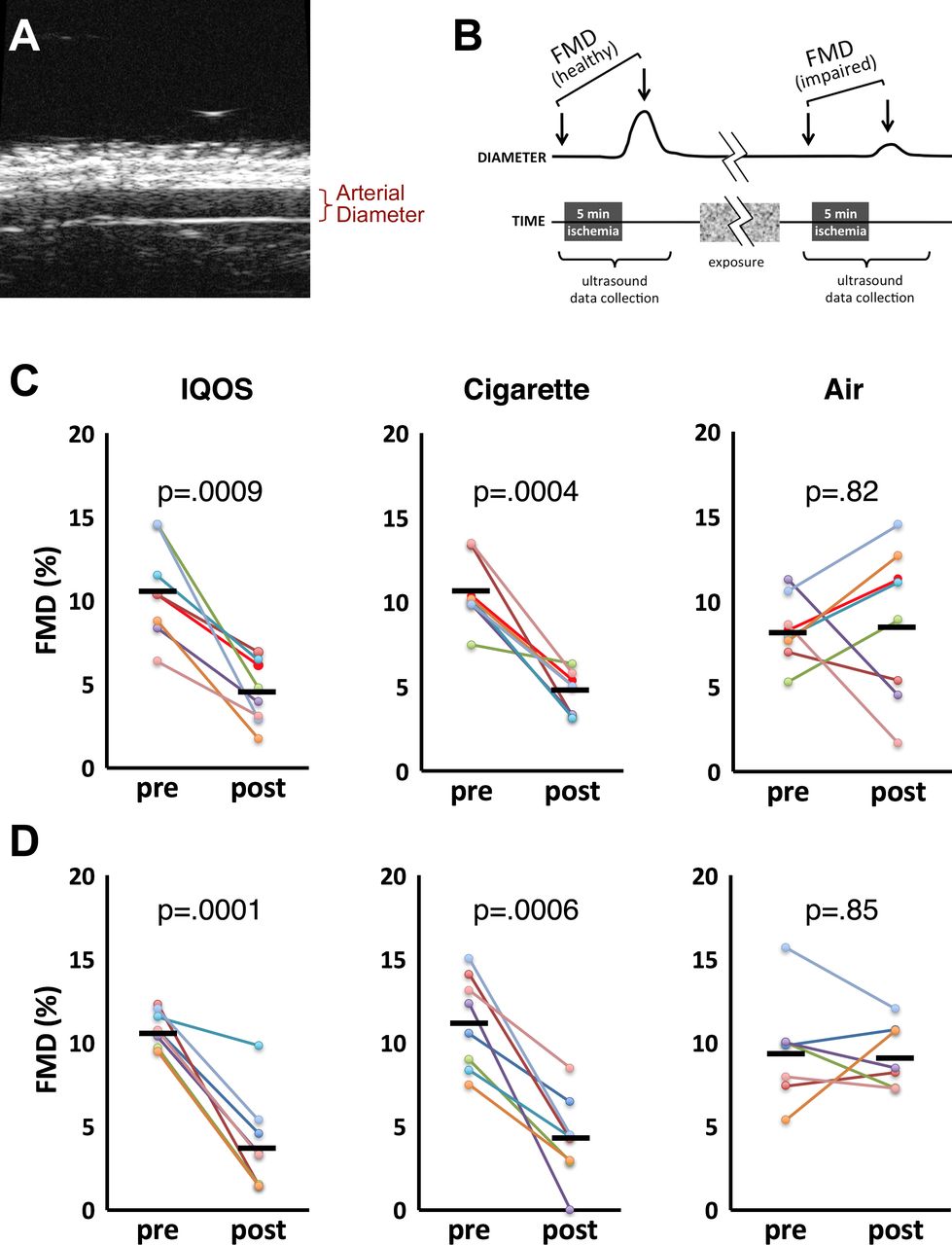
Arterial flow-mediated dilation was impaired by mainstream cigarette smoke and IQOS aerosol. (A) Ultrasound imaging of rat femoral artery. (B) FMD experimental design: FMD was measured pre-exposure and postexposure in each rat. (C) FMD after 10 cycles of 15 s exposure +15 s break. (D) FMD after 10 cycles of 5 s exposure +25 s break. Coloured lines denote individual rats pre-exposure and postexposure; bars denote group means; p values are derived from paired 2-tailed t-tests. FMD, flow-mediated dilation.
Serum nicotine and cotinine measurements
For measurement of nicotine and its metabolite cotinine, we collected blood immediately after exposure (from IQOS-exposed and cigarette-exposed rats not being used for FMD measurement; n=5/group) and 20 min later (from IQOS-exposed and cigarette-exposed rats after the final FMD measurement; n=8/group) via thoracotomy and cardiac puncture using a 23G blood collection set (BD Vacutainer) and untreated tubes. We centrifuged the blood samples at 800 rcf for 15 min and immediately stored the serum samples at −80˚C. Concentrations of nicotine and cotinine were determined by gas chromatography—tandem mass spectrometry.38 The limits of quantitation were 1 ng/mL for nicotine and 10 ng/mL for cotinine.
Aerosol and mainstream smoke nicotine measurements
We measured nicotine in both gas and particle phases of the IQOS aerosol and mainstream smoke from Marlboro Red cigarettes and 1R6F research cigarettes using the method described above. Particle phase nicotine was captured in mainstream aerosol and smoke on Cambridge filter pads placed downstream of the cigarette/IQOS filter, using modified ISO conditions of one 35 mL puff every 30 s for a total of 10 puffs (n=3/group). The filtered aerosol went through an impinger filled with 0.036 N HCl to trap the gas phase nicotine. We also analysed the postuse residual material in the HeatSticks as well as unused HeatSticks for nicotine levels. The filters and the contents of the HeatStick were extracted with 20 mL of an extraction buffer containing 25% by volume of t-butanol, 0.5 M citric acid and 20 mM ascorbic acid by sonicating for 60 min at 60°C. The tubes were centrifuged at 3000 g for 5 min and aliquots of the supernatant were analysed. Liquid chromatography-tandem mass spectrometry37 was used to measure the nicotine levels in the samples.
Statistics
We used paired t-tests to compare the FMD values in each group before and after exposures. Errors are presented in this report as SD. A two-way repeated measures analysis of variance (ANOVA) was run to examine the effect of type and duration of exposure on per cent FMD reduction. P value of <0.05 was considered statistically significant. Calculations were done using Stata V.13.1.
Results
Comparable impairment of FMD by exposure to IQOS aerosol and cigarette mainstream smoke
Exposure in the first experiment (figure 3C) consisted of 10 cycles of 15 s exposure +15 s break (out of the nose cone). A subsequent experiment (figure 3D) used the more realistic regimen of 10 cycles of 5 s exposure +25 s break.
FMD was reduced comparably by ten 15 s exposures to IQOS aerosol (10.6±2.9% pre-exposure vs 4.5±1.9% postexposure, p=0.0009) and cigarette smoke (10.6±2.0% pre-exposure vs 4.6±1.3% postexposure, p=0.0004). FMD was not affected in the clean air control group (8.3±1.9% vs 8.8±4.5%, p=0.82).
FMD was also impaired comparably by ten 5 s exposures to IQOS aerosol and cigarette smoke (10.8±1.0% pre-exposure vs 3.8±2.6% postexposure, p=0.0001; and 11.2±2.6% pre-exposure vs 4.2±2.3% postexposure, p=0.0006, respectively). FMD was not affected in the air control group (9.5±3.0% vs 8.1±1.8%, p=0.85).
A two-way repeated measures ANOVA revealed that there was not a significant interaction between type and duration of exposure on per cent FMD reduction, F (2, 41)=0.30, p=0.73. The per cent FMD impairment was not significantly different in groups exposed for 5 s compared with 15 s (p=0.27), which suggests that the endothelial response was saturated with a single HeatStick or cigarette.
Serum nicotine was comparable to that resulting from smoking by humans
To evaluate the accuracy of the exposure conditions in our rats and its relevance to real-world levels, we compared the postcigarette exposure serum nicotine levels in rats to that reported for humans (figure 4). In rats subjected to the 10 x (5+25 s) regimen, mean nicotine levels in samples immediately after exposure were 70.3±26.3 and 15.0±7.7 ng/mL in the IQOS and cigarette groups, respectively. Average nicotine levels immediately after exposure in the cigarette group was similar to the levels in humans after smoking one cigarette (~10–50 ng/mL),39 40 confirming that the exposure conditions were relevant to real-world smoking. In the serum samples taken 20 min after the exposure, mean nicotine levels were 39.7±18.9 and 5.6±2.5 ng/mL in IQOS and cigarette groups. Serum cotinine levels were 4.6±1.9 and 6.5±2.8 ng/mL in IQOS-exposed group immediately after exposure and 20 min later. In the cigarette-exposed group, cotinine was undetectable after exposure and 0.8±1.4 ng/mL after 20 min.

Serum nicotine and cotinine levels immediately and 20 min postexposure. Samples were taken after 10 cycles of 5 s exposure +25 s break. P values are derived from two-tailed Student’s t-tests. IQOS x10, 10 IQOS exposure cycles; cigarette x10, 10 cigarette exposure cycles; air x10, 10 air exposure cycles; IQOS x3, three IQOS exposure cycles; BLQ, below level of quantification.
Serum nicotine and cotinine levels were significantly higher in the IQOS-exposed group compared with the cigarette-exposed group at all times. Nicotine and cotinine were not detected in the air groups.
Comparable FMD impairment from lower level IQOS exposure
Because the nicotine levels in IQOS group were substantially higher than that in the cigarette group, impairment of FMD in the IQOS group could potentially be attributed to excessive nicotine exposure. Therefore, we titrated the IQOS exposure timing down to conditions that led to serum nicotine comparable with the cigarette group (three 5+25 s cycles rather than 10 cycles led to 14.8±11.6 ng/mL serum nicotine initially). Average FMD in a group of rats exposed to three cycles of IQOS aerosol decreased significantly from 11.0±4.2 to 4.5±1.5 (p=0.0019). A group of four air-exposed rats that was included for blinding purposes showed no significant change in FMD (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Reduced IQOS exposure to match nicotine absorption level of the cigarette group still impairs FMD to a comparable extent. Coloured lines denote individual rats pre-exposure and postexposure; bars denote group means; p values are derived from paired two-tailed t-tests. Exposure conditions were three cycles of 5 s exposure +25 s break. FMD, flow-mediated dilation.
Higher nicotine in Marlboro Red smoke than IQOS aerosol
To determine if the higher serum nicotine levels resulting from IQOS exposure than smoke exposure reflected higher nicotine concentrations in IQOS aerosol, we measured nicotine in both kinds of emissions, using both Marlboro Red cigarettes and 1R6F research cigarettes for comparison. Total nicotine levels in smoke from the Marlboro cigarettes were significantly higher than that in IQOS aerosol (1.07±0.05 vs 0.67±0.02, p=0.0006). Nicotine levels in the 1R6F smoke were similar to IQOS aerosol levels (table 1).
Nicotine concentration in IQOS aerosol, cigarette mainstream smoke and IQOS tobacco
Nicotine in the IQOS aerosol gas phase was below the detection limits. Analysis of HeatSticks before and after use also revealed that the nicotine in the aerosol is mainly in the particle phase.
Discussion
Historically, the tobacco industry has made a major effort to introduce their so-called heat-not-burn tobacco products to consumers as reduced-risk products. Unlike earlier generation products such as R.J. Reynolds’ Premier (1988), Eclipse (1996, 2003) and Revo (2015), and Philip Morris’ Accord (1998) and Heatbar (2006), IQOS has been successfully marketed in at least 30 countries.1 41 42 Although IQOS is currently not available in the USA, industry analysts are making optimistic predictions regarding successful future US marketing of IQOS.41 43 Our aim was to study the vascular effects of exposure to IQOS aerosol before this product achieves more widespread use. To our knowledge, this is the first study of the effects of IQOS aerosol on vascular endothelial function in a physiological model.
PMI strongly implies in publications21 23 44 and in their MRTP applications45 that IQOS causes less endothelial dysfunction than conventional cigarettes. Their conclusions were based only on cultured cell behaviour21 and circulating sICAM-1 protein23 that indirectly reflect processes relevant to vascular function, but do not directly assess endothelial function physiologically. PMI’s physiological cardiovascular studies were limited to the demonstration that long-term IQOS aerosol exposure led to less aortic plaque than cigarette smoke in transgenic mice predisposed to atherosclerosis.44 In contrast, our direct evaluation of IQOS aerosol’s acute effects showed that brief exposures to IQOS aerosol from a single HeatStick caused rapid impairment of vascular endothelial function in rats comparable with that caused by cigarette smoke. We assessed endothelial function with FMD, a validated measure of cardiovascular health effects24–27 that has been used by numerous groups to evaluate cardiovascular effects of smoke exposure in humans and animals.28–31 34–36 Therefore, our approach provides a robust readout of potential adverse effects of IQOS aerosol on endothelial function, and indicates that IQOS use is likely to have rapid adverse vascular effects comparable with those from cigarette smoking.
We chose to use a nose cone smoke/aerosol delivery system, rather than a whole-body exposure system, to prevent exposure via the ocular and oral routes and also to prevent subsequent oral exposure from licking fur and paws. Establishment of an exact relationship between our rat exposure conditions and human exposure is limited by differences in route of administration (rats are obligate nose breathers with complex nasal topography46 while humans inhale cigarette smoke orally), differences between human intentional aerosol inhalation volume and anaesthetised rat tidal (inhalation) volumes,47 48 and differences in airway clearance rates.49 Sophisticated models have been developed to convert inhalation dosimetry between rats and humans,49 but smoke does not present a straightforward situation due to the combination of gas and highly heterogeneous particles that behave differently in such models. Therefore, to assess whether our exposure conditions were relevant to real-world smoking, we measured serum nicotine levels and confirmed that nicotine in the rats that were exposed to cigarette smoke for ten 5+25 s cycles were similar to the levels found in humans immediately after smoking one cigarette, validating our exposure model for cigarettes.
However, the serum nicotine level in the IQOS-exposed group under identical conditions was more than four times higher than in the cigarette group. This was surprising; our results revealed that the nicotine content in the IQOS aerosol in our generation system was much lower than that in the Marlboro mainstream smoke (table 1). Moreover, nicotine content in the filler and aerosol is reported in the literature to be roughly comparable for HeatSticks and cigarettes.50 51 The underlying reason for this remains unclear and deserves further investigation. One potential explanation for this difference could be particle size difference which determines to what extent the particles reach the respiratory zone. Nonetheless, reducing the number of IQOS exposure cycles from 10 to 3, to result in comparable serum nicotine concentrations to the cigarette group still led to impairment of FMD. Of note, the extents of FMD impairment in the three IQOS and cigarette groups were quite similar, indicating an extremely rapid saturation of the response to mainstream levels of smoke and IQOS aerosol.
A limitation of this study is that all functional measurements were obtained in anaesthetised rats which was necessary for the FMD procedure to be carried out. However, as in our previous reports using ketamine/xylazine,34–36 as well as our prior study unrelated to smoke in which isoflurane was used,52 negative control groups showed no significant alteration of FMD from preintervention to postintervention, and the relative responses of experimental and control groups have been consistent and reproducible. Moreover, prospective human exposure experiments have shown similar impairment of FMD by smoke inhalation in conscious individuals.30 31 53
Regarding potential variability between experiments, we used a manual syringe-pump-driven system to generate smoke and IQOS aerosol for our initial experiment, and a commercially available automatic vaping system for our subsequent experiments. The manual system was modelled after the automatic system; that is, the relevant volumes and aerosol paths were the same in all experiments. The volume of air drawn through the cigarettes and HeatSticks, and the time over which the syringe pump plunger was moved, were the same in all experiments, although slightly more accurate with the automatic system. Similarly, due to broken heating blades as described in the Materials and methods section, we used IQOS holders from three different countries over the course of the project. The characteristics of these electronic devices are presumably highly controlled and would not be expected to vary greatly by country. We did not perform comparative analyses of aerosols generated from the three devices. When it was necessary to switch from a broken device to a new one, rats in both experimental and control groups were exposed to aerosol from the new device.
We conclude that mainstream IQOS aerosol from a single HeatStick can rapidly and substantially impair endothelial function in rats comparably to smoke from a cigarette. While these findings do not prove that inhalation of IQOS aerosol causes endothelial dysfunction in humans, the results underscore that integrative physiological assays of function can reveal adverse health effects not noted in PMI’s biomarker and cell culture studies,2 and suggest that at least some of the adverse health effects of cigarettes may not be avoided by using IQOS.
What this paper adds
IQOS is a new heated tobacco product from Philip Morris International that has been marketed in 30 countries and has been portrayed to consumers and regulatory agencies as modified-risk tobacco product.
Brief exposures to IQOS aerosol cause endothelial dysfunction, a well-established physiological measure of cardiovascular risk that is also caused by exposure to cigarette smoke, to the same extent as cigarette smoke in rats.
Acute exposure to IQOS aerosol impairs flow-mediated dilation in rats.
Use of IQOS does not necessarily avoid the adverse cardiovascular effects of cigarette smoking.
Acknowledgments
Gas chromatography-tandem mass spectrometry analyses were performed by Kristina Bello and Lawrence Chan in the Clinical Pharmacology Research Laboratory at UCSF, supervised by Peyton Jacob, III. We thank Dorie Apollonio and Minji Kim for helping us obtain some of the IQOS devices used in this study, and Stanton Glantz and Xiaoyin Wang for helpful discussions during the design of the project and critical comments on the manuscript.
References
Footnotes
Contributors PN, JL, CMH, SI and RD performed experiments and collected/analysed data. PN, CMH, PJ and MLS designed experiments, PN and MLS conceived of the project and wrote the paper.
Funding This work was supported by grant R01HL120062 from the National Heart, Lung, and Blood Institute at the National Institutes of Health (NIH) and the US Food and Drug Administration Center for Tobacco Products (FDA CTP), grant 25IR-0030 from the California Tobacco-Related Disease Research Program, and grant P50CA180890 from the National Cancer Institute at the NIH and FDA CTP. Laboratory resources for analytical chemistry were supported by grant P30 DA012393 from the National Institute on Drug Abuse at the NIH.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the FDA.
Competing interests None declared.
Patient consent Not required.
Ethics approval All animal procedures were approved by the University of California, San Francisco Institutional Animal Care and Use Committee.
Provenance and peer review Not commissioned; externally peer reviewed.