Article Text

Abstract
Introduction Even prior to 2018, electronic nicotine delivery systems (ENDS) began to dramatically change the landscape of tobacco products and product use patterns in the USA.
Methods Using a Markov multistate transition model accounting for complex survey design, transition rates between never, non-current, cigarette, ENDS and dual use states were estimated for 23 253 adult participants in waves 1–4 (approximately 2013–2017) of the Population Assessment of Tobacco and Health study. We made short-term transition projections and estimated HRs for age, sex, race/ethnicity, education and income.
Results Cigarette use was persistent among adults, with 89.7% (95% CI 89.1% to 90.3%) of exclusive cigarette users and 86.1% (95% CI 84.4% to 87.9%) of dual users remaining cigarette users (either exclusive or dual) after one wave. In contrast, ENDS use was less persistent, with 72.1% (95% CI 69.6% to 74.6%) of exclusive ENDS users and 50.5% (95% CI 47.8% to 53.3%) of dual users remaining ENDS users (with or without cigarettes) after one wave. Exclusive ENDS users were more likely to start cigarette use after one wave than either never users (HR 25.2; 95% CI 20.9 to 30.5) or non-current users (HR 5.0; 95% CI 4.3 to 5.8). Dual users of ENDS and cigarettes were more likely to stop using cigarettes than exclusive cigarette users (HR 1.9; 95% CI 1.6 to 2.3). Transition rates varied among sociodemographic groups.
Conclusions Multistate transition models are an effective tool for uncovering and characterising longitudinal patterns and determinants of tobacco use from complex survey data. ENDS use among US adults was less persistent than cigarette use prior to 2018.
- electronic nicotine delivery devices
- non-cigarette tobacco products
- surveillance and monitoring
- disparities
Data availability statement
Data are available in a public, open access repository. Data from the PATH study are available for download as Public Use Files in a public, open access repository (https://doi.org/10.3886/ICPSR36498.v10). Conditions of use are available on the website above.
Statistics from Altmetric.com
- electronic nicotine delivery devices
- non-cigarette tobacco products
- surveillance and monitoring
- disparities
Introduction
The introduction of electronic nicotine delivery systems (ENDS) has dramatically changed the landscape of tobacco products and patterns of use in the USA and other high-income countries.1 2 Policymakers and researchers are struggling to understand whether ENDS should be seen as a lower risk alternative to cigarettes (ie, a modified risk product)3 4 or a product that interferes with smoking cessation by continuing nicotine addiction,5–7 and whether ENDS serve as a catalyst for—or diversion from—youth and young adult tobacco use initiation.8 Estimating the population-level impact of ENDS will require a nuanced systems approach to estimate how multiple, interdependent factors give rise to future patterns of use and health outcomes.9 10 Moreover, for tobacco control and public health policy to be more effective, a better understanding of transitions between cigarettes and ENDS is needed.
Nationally representative cross-sectional surveys, such as the Tobacco Use Supplement to the Current Population Survey and the National Health Interview Survey, are able to tell us how prevalence of ENDS and other tobacco product use is changing over time, but their design precludes reconstruction of individuals’ tobacco product use histories. The Population Assessment of Tobacco and Health (PATH) study,11 on the other hand, offers repeated observations of an individual’s product use over multiple years. PATH’s design also provides the opportunity to examine differences in transition rates between sociodemographic groups, which may lead to large disparities in short-term and long-term product use and downstream health effects.12 13 While these transitions in PATH have been empirically analysed, providing a basic description of the data,14–16 a systems approach allows us to understand the underlying transition rates that give rise to the observed use patterns.
Markov multistate transition modelling is a mathematical framework that can be used to estimate underlying transition rates between states from longitudinal data on individuals, which can in turn be used to assess, for example, whether use of one product impacts initiation or discontinuation of another product or to make predictions of future patterns. These models can be further specified to estimate the effect of sociodemographic factors on the transition rates. Although Markov multistate transition modelling has only relatively recently been introduced to the field of tobacco control research, it has been applied to estimate product use transitions in several longitudinal surveys,17–20 enhancing our understanding of patterns of product use, particularly among youth and young adults. However, there has thus far been uncertainty over how to implement these methods on complex survey data that require use of sample weights, clustering, strata, and so on, limiting the applicability and impact of this method so far.
In this analysis, we develop a Markov multistate transition framework to incorporate complex survey data and analyse transitions between subsequent waves between cigarette, ENDS, dual, non-current and never use states for adults in waves 1–4 of the PATH study, and estimate transition rate ratios by age, sex, race/ethnicity, education and income. This study period is largely prior to the ENDS market changes precipitated by JUUL products in late 2017 (end of wave 4).
Methods
Data and tobacco use state definitions
We used data on adults in waves 1–4 (September 2013 to January 2018) of the PATH study.11 We consider only adults here because youth have distinct patterns of use and transitions that we believe should be analysed separately. Time between follow-up for each participant was approximately 1 year. We restricted our analysis to participants who completed an adult interview in wave 4. We further restricted the individual data to only those waves in which participants were adults (some participants were youth in earlier waves), and we removed any participants from the sample who had only a single tobacco state observation, since single observations are uninformative for the transition model. In addition to the questions informing our tobacco use state definitions (see below), we used information on age (18–24, 25–34, 35–54, 55+), sex (male, female), race/ethnicity (non-Hispanic (NH) White, NH Black, Hispanic, other), educational attainment (less than high school, high school or equivalent, some college or associate’s degree, bachelor’s degree or higher) and income (<$25 000, $25 000–$50 000, >$50 000). We used baseline values of sex and race/ethnicity but used age, educational attainment and income reported in the most recent wave. We defined educational attainment only for those ages 25+ because many people aged 18–24 are still completing their education. We used PATH imputations of missing sex, race and ethnicity values at waves 1 and 4. After incorporating this imputation, we removed participants still missing information for any covariate in a given wave (4% of participants); we analysed 23 253 participants with 84 887 total observations and 7461 transitions. Participant weights were normalised to the number of participants. Descriptive characteristics of the sample are given in the online supplemental table S1.
Supplemental material
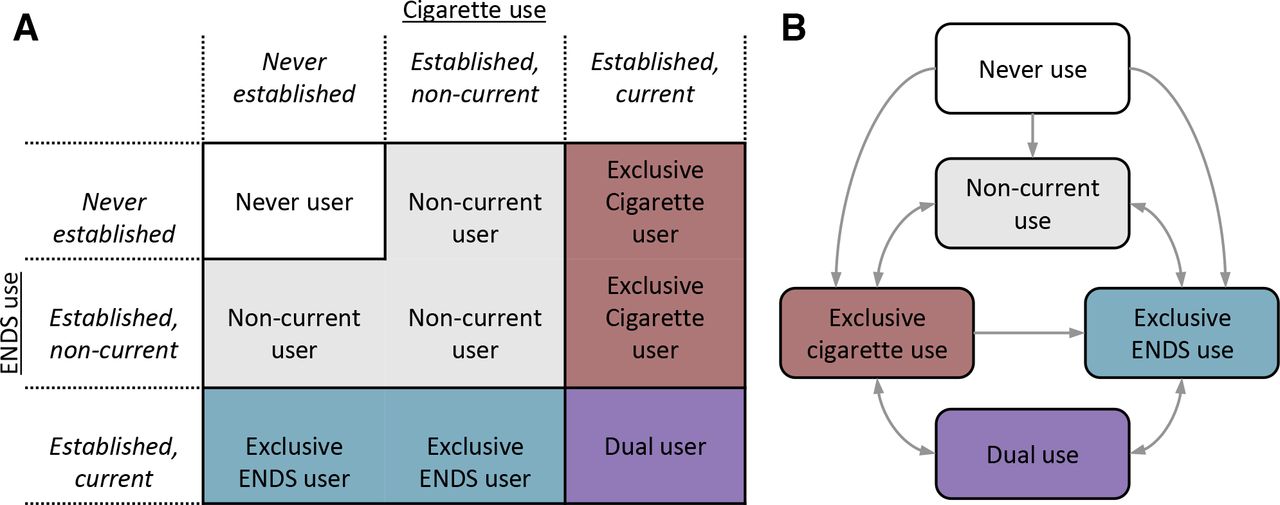
We assigned each PATH participant to a tobacco use state in each wave based on answers to questions about established use of cigarettes (100+ lifetime cigarettes) and ENDS (ever fairly regular ENDS user) and past 30-day use. See the online supplemental material for further information and variable coding. We considered five tobacco use states: never user, non-current user, exclusive cigarette user, exclusive ENDS user and dual user (figure 1A). The sociodemographic characteristics of the participants in each use state are provided in the online supplemental table S2. These data show substantial demographic differences among these groups. For instance, cigarette users tended to be older than ENDS or dual users and to be somewhat lower in income. Non-current use refers to at least 30-day abstinence, which includes ‘former’ users, but we refer to transitions to this state as ‘stopping’ use as opposed to ‘quitting’, since the terms ‘former’ and ‘quit’ generally refer to longer term cessation. Similarly, we use ‘start’ to indicate use after a period of non-use, capturing both initiation and relapse.

(A) Tobacco use state definitions. (B) The direct transitions allowed between states in the model. ENDS, electronic nicotine delivery systems.
Transition modelling
We used a Markov multistate transition model to analyse the underlying transition hazard rates and HRs. The states and transitions in this model are represented in figure 1B. A Markov multistate transition model is a continuous-time, finite-state stochastic process that assumes that transition rates depend only on the current state and not on past states or transition history.21 We discuss the method generally here, but the full technical details are provided in the online supplemental material.
A Markov multistate transition model estimates transition hazard rates, that is, the instantaneous risk of transitioning from one state to another. These transition hazard rates collectively define the probabilities of being in each state at future times, thereby connecting the model to longitudinal data of the actual observed states. We illustrate an example of the connection between the continuous-time model and the observation process in figure 2. In general, the transition probabilities may depend on the observation year, but we found that variation and trends in estimates across waves were minor (see online supplemental figure S1). Accordingly, we assume that the transition probabilities depend only on the length of time between observations and not on the specific waves.

People transition between tobacco use states. We observe these states at fixed time points, but we do not know when the transitions occurred or if there were multiple transitions between observations. The multistate transition model estimates the underlying instantaneous transition hazard rates that best explain the observed data when they are combined to estimate probabilities of being in each state at future times.
Transition hazards may differ for different sociodemographic groups, so we determined transition HRs for each group for each covariate, denoting the relative transition intensity across groups. We estimated HRs for each sociodemographic group in univariable models.
Once the transition hazard rates are estimated, they can be used to make projections of future patterns of use. In this study, we used the transition rates to make 2- and 4-year projections as well as determine what the eventual long-term steady-state prevalence of use would be if these rates were to continue. While subject to error from future trends, this long-term calculation can provide a point of reference. We also used the transition hazards to estimate the relative rate of starting or stopping cigarette use for people who were or were not current ENDS users.
Incorporation of complex survey design
Complex survey design calculates sample weights that can be used to determine point estimates for quantities of interest, and replicate weights are a way to account for other complex survey design aspects, such as strata and primary sampling units, when estimating the variance of those point estimates. Without weights, estimates will be biased (online supplemental figure S2). Since survey weights cannot be incorporated in the widely used R package for Markov multistate transition modelling, msm,22 we adapted code from this package to incorporate weights. Our code is available at www.tcors.umich.edu. In this analysis, we incorporated PATH wave 4 adult all-wave longitudinal weights. Variance estimates were calculated using the 100 replicate weights provided by PATH, which are calculated by Fay’s method, a variant of balanced repeated replication.11 We recalculated the transition hazard rates and transition HRs for each replicate. Full technical details are provided in the online supplemental material.
Model reduction
Estimates of rates for rare transitions can be unreliable and uninformative and including them in the model can interfere with estimating the other parameters. Thus, we identified state transitions that were rare enough that they should be considered negligible. Using a Schwarz information criterion to compare model fits, it was appropriate to assume that there was no direct, instantaneous transition from never or non-current use to dual use, from dual use to non-current use, or from ENDS to cigarette use (figure 1B), similar to previous analyses.17 19 Individuals may still transition from never to dual use in just one wave but must first transition through at least one other (unobserved) state (eg, from never to cigarette to dual use).
Results
Transition probabilities
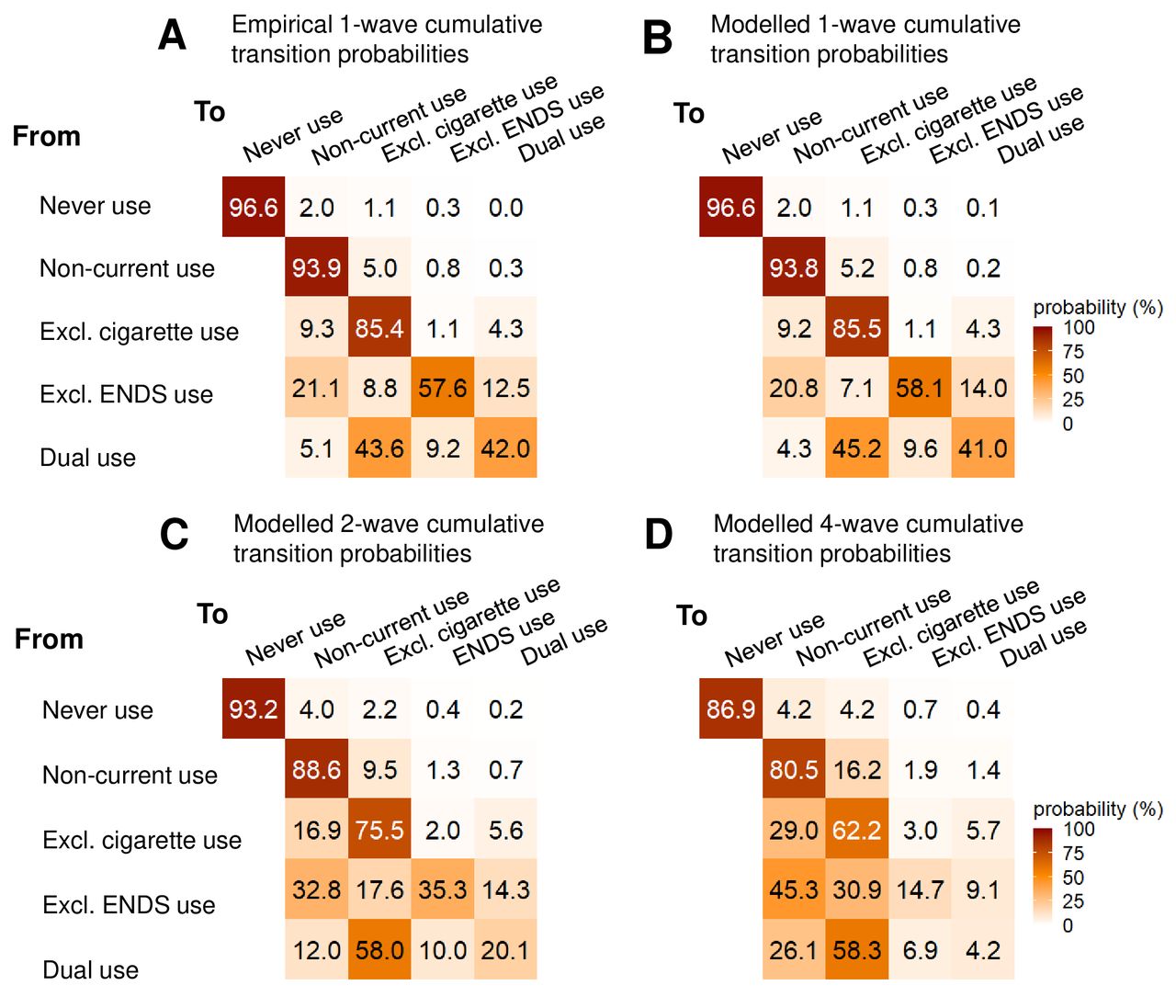
We compared the empirical one-wave (approximately 1 year) transition probabilities averaged over all four waves with the modelled one-wave transition probabilities (figure 3A,B). The model reproduces the empirical transitions well. Cigarette use was persistent, with 89.7% (95% CI 89.1% to 90.3%) of exclusive cigarette users and 86.1% (95% CI 84.4% to 87.9%) of dual users remaining cigarette users (either exclusive or dual) after one wave (figure 3B). In contrast, ENDS use was less persistent, with 72.1% (95% CI 69.6% to 74.6%) of exclusive ENDS users and 50.5% (95% CI 47.8% to 53.3%) of dual users remaining ENDS users (either exclusive or dual) after one wave. We found that 20.8% (95% CI 18.2% to 23.3%) of exclusive ENDS users transitioned to non-current use by the subsequent wave, and 45.2% (95% CI 42.4% to 47.9%) of dual users transitioned to exclusive cigarette use. The CIs for both the hazard rates and the transition probabilities are provided in the online supplemental table S3.

One-wave (approximately 1 year) transition probability between tobacco use states estimated from (A) all-wave average weighted observed transitions and (B) the multistate transition model. The model matches the data well and provides estimates of underlying transition rates. We also include short-term projections of tobacco use states from the multistate transition model with (C) two-wave and (D) four-wave transition probabilities. ENDS, electronic nicotine delivery systems.
Projections of product use transitions
The less persistent nature of ENDS use by adults was further highlighted by the short-term projections of the model (figure 3C,D). We estimated that only 49.6% (95% CI 46.4% to 52.8%) of exclusive ENDS users would still be using ENDS after 2 years; this number drops to 23.8% (95% CI 21.1% to 26.5%) after 4 years. In contrast, 68.0% (95% CI 66.5% to 69.4%) of exclusive cigarette users would still be using cigarettes after 4 years (about 90% of whom will be using exclusively cigarettes). Most dual users would transition to exclusive cigarette use, and this transition occurs quickly: 58.0% (95% CI 55.3% to 60.6%) of dual users become exclusive cigarette users after 2 years. Fewer than 10% of dual users are predicted to remain dual users 4 years later. If these transition rates were to persist, then the long-term, steady-state prevalence of use in this cohort of ever users (ie, excluding initiation of never users) would be: 60.5% (95% CI 58.6% to 62.5%) non-current users, 33.3% (95% CI 31.5% to 35.2%) exclusive cigarette users, 2.8% (95% CI 2.4% to 3.1%) exclusive ENDS users and 3.3% (95% CI 3.0% to 3.6%) dual users. These projections should be treated as illustrations rather than predictions, since transition rates will likely change in the future in response to marketplace changes, regulations and other pressures.
The impact of ENDS on rates of starting and stopping cigarette use
We estimated the association of current ENDS use with rates of starting and stopping cigarettes. We found that exclusive ENDS users (who may or may not have ever used cigarettes) are more likely to be using cigarettes in the next wave than never users (HR 25.2; 95% CI 20.9 to 30.5) or non-current users (HR 5.0; 95% CI 4.3 to 5.8). Based on the transition rates, we would expect 1% of never users, 6% of non-current users and 25% of exclusive ENDS users to be using cigarettes after one wave. (Note that these numbers represent a person’s first transition within a wave; figure 3 accounts for the possibility of multiple transitions within one wave.) Dual users of ENDS and cigarettes were also more likely to stop using cigarettes than exclusive cigarette users (HR 1.9; 95% CI 1.6 to 2.3). Based on the transition rates, we would expect 10% of cigarette users and 18% of dual users to not be using cigarettes after one wave. However, the number of transitions depends on the prevalence of each tobacco use state. Over waves 1–4, the average prevalence estimates were 58.3% for never users, 22.5% for non-current users, 16.5% for exclusive cigarette users, 1.2% for exclusive ENDS users and 1.5% for dual users. Accordingly, of the people starting cigarette use in this period, we estimate 56% were previously non-current users, 30% were previously never users and only 14% were ENDS users. Similarly, of the people stopping cigarette use in this period, 86% were exclusive cigarette users, while only 14% were previously dual users.
Transition hazards by sociodemographic group
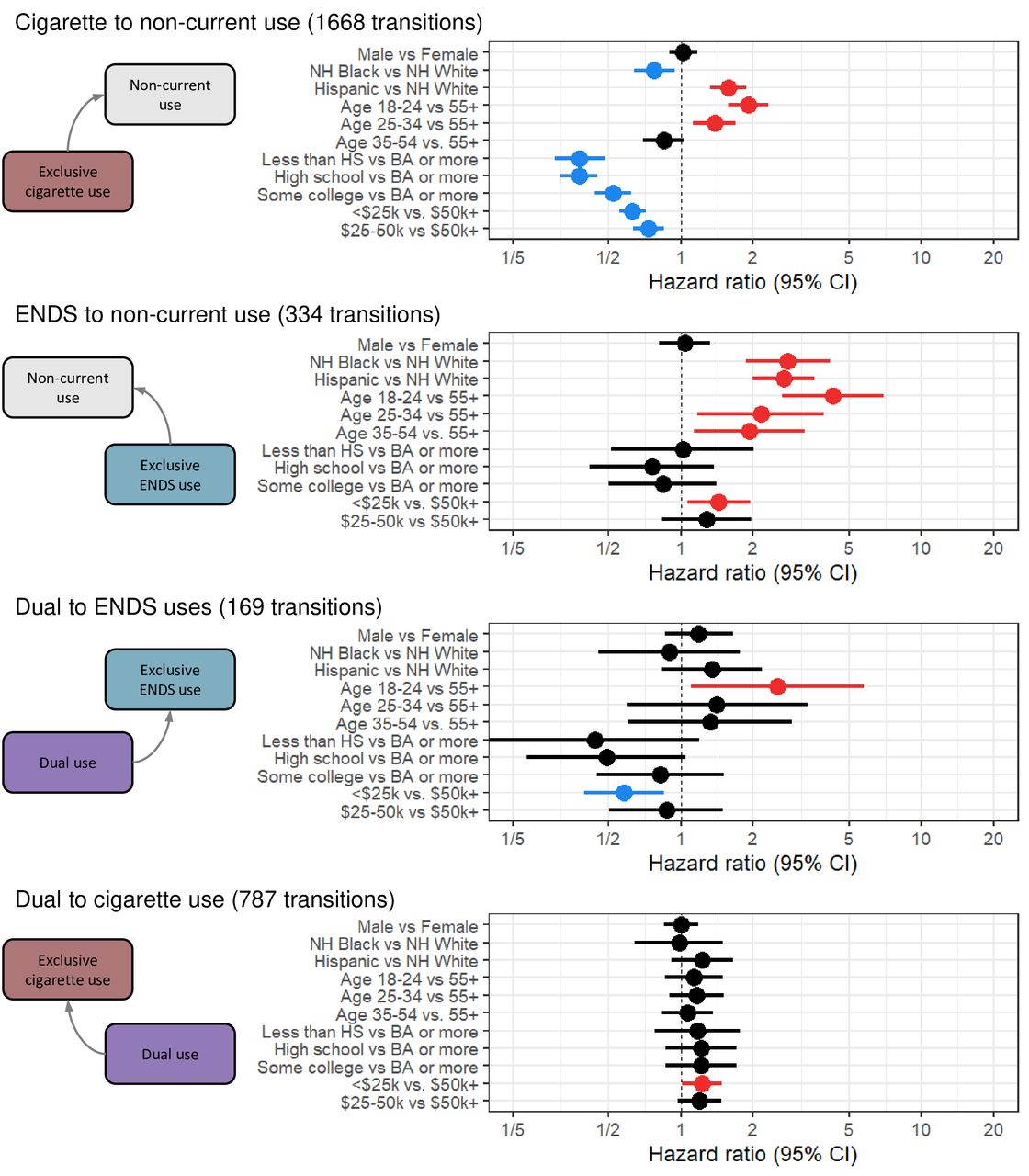
Transition rates vary by sociodemographic group. We present HRs for the eight transitions related to starting or stopping cigarette or ENDS use (figures 4 and 5). HRs by sociodemographic group for these transitions are provided in the online supplemental tables S4–S8, as are one-wave transition probabilities (online supplemental figures S3–S7). There is a substantial age gradient in each transition, with younger users more likely to transition than older users, for both starting and stopping use of either cigarettes or ENDS. We see that never users aged 18–24 years are substantially more likely to initiate ENDS use than never users aged 34–54 years (HR 27.6; 95% CI 8.1 to 93.9). The effect is smaller but still significant among current cigarette users (HR 4.5; 95% CI 3.2 to 6.3). Men are more likely than women to initiate either cigarettes (HR 1.7; 95% CI 1.4 to 2.0) or ENDS use (HR 3.6; 95% CI 2.5 to 5.3) from never use. NH Black and Hispanic never users are more likely to initiate exclusive cigarette use than NH White never users (NH Black HR 2.7; 95% CI 2.1 to 3.3; Hispanic HR 2.1; 95% CI 1.6 to 2.7); however, both NH Black and Hispanic exclusive cigarette users are less likely to start ENDS to become dual users than NH White exclusive cigarette users (NH Black HR 0.4; 95% CI 0.3 to 0.6; Hispanic HR 0.7; 95% CI 0.5 to 0.9). NH Black exclusive cigarette users are less likely to transition from cigarette to non-current use than NH White users (HR 0.8; 95% CI 0.6 to 0.9) while Hispanics are more likely to make this transition (HR 1.6; 95% CI 1.3 to 1.9). Both NH Black and Hispanic exclusive ENDS users are more likely than NH White ENDS users to transition to non-current use (NH Black HR 2.8; 95% CI 1.9 to 4.2; Hispanic HR 2.7; 95% CI 2.0 to 3.6). Higher income and education levels are generally associated with lower rates of starting single product use and higher rates of discontinuing use. Among dual users, individuals in the lowest income bracket were more likely to transition to exclusive cigarette use than those in the highest income bracket (HR 1.3; 95% CI 1.0 to 1.5) and less likely to transition to exclusive ENDS use (HR 0.6; 95% CI 0.4 to 0.9).

HRs by sociodemographic group for selected transitions corresponding to starting cigarette or ENDS use (univariable models). Red HRs are significantly greater than 1, blue HRs are significantly less than 1 and black HRs are not significant at significance level α=0.05. BA, Bachelor of Arts; ENDS, electronic nicotine delivery systems; HS, high school; NH, non-Hispanic.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
HRs by sociodemographic group for selected transitions corresponding to stopping cigarette or ENDS use (univariable models). Red HRs are significantly greater than 1, blue HRs are significantly less than 1 and black HRs are not significant at significance level α=0.05. BA, Bachelor of Arts; ENDS, electronic nicotine delivery systems; HS, high school; NH, non-Hispanic.
Discussion
We developed and applied a multistate transition model to a longitudinal, complex survey of adults in order to estimate underlying rates of transition between different kinds of tobacco use. In the pre-JUUL era (before 2018) in the USA, we find that adult use of ENDS was less persistent than cigarette use. This result was true for both exclusive ENDS users and dual users of ENDS and cigarettes. This pattern was previously reported from empirical analysis of the first three waves of PATH,14–16 23 and our analysis demonstrates that it has continued. Results from at least one other study have also suggested ENDS use in adults has not been durable.24 Although the landscape of tobacco products is expected to continue to change—including with the recent advent of IQOS (a type of Heated Tobacco Product) and pod/cartridge ENDS products—,these results provide valuable insight into how ENDS products have been used in the recent past, and this analysis can be updated with future surveys to track how transition rates evolve with new products.
Multistate transition modelling is a powerful tool for exploring the patterns that underlie longitudinal transition data. Unlike previous empirical analyses that have described observed transitions in PATH, this approach allows us to estimate transition incidence and the underlying transition rates. Our method considers the potential for multiple transitions between observations, can incorporate information from participants with missing observations, expands the kinds of inferences we can make (eg, sociodemographic HRs) and allows for short-term predictions for the whole cohort. The field of tobacco regulatory science has just recently begun to apply these models to longitudinal surveys.17–20 However, the importance of incorporating complex survey design into these transition models has been underappreciated: to our knowledge, this study is the first tobacco research analysis to incorporate study weights and variance estimation directly. Without weights, transition estimates will be biased, and without appropriate treatment of variance, confidence bounds may be artificially narrow. The lack of easily available methods to incorporate complex survey design into transition models has thus far hampered the field, but future transition modelling work on complex survey data should incorporate the approach we outlined here, or another valid approach, such as synthetic populations.25
There is a continued debate about whether ENDS should be considered a cigarette cessation tool or a catalyst of cigarette use and, accordingly, which tobacco control policies should be adopted.3–5 8 26 Although this analysis cannot directly address the question of whether ENDS use causally increases or decreases cigarette initiation or cessation rates, we find that ENDS, as generally used by adults in approximately 2013–2017, were associated with increased rates of both initiation/relapse and 30-day abstinence from cigarette use. However, the magnitudes of the effects were substantially different. Exclusive ENDS users (including never cigarette users or non-current cigarette users) were more than 20 times more likely to be using cigarettes in the subsequent wave than never users (25% vs 1% transition in one wave) and about five times more likely than non-current users (25% vs 6% transition in one wave). In contrast, dual users were only about two times more likely to not be using cigarettes in the subsequent wave than exclusive cigarette users (18% vs 10% transition in one wave). These results suggest that ENDS may have been used to replace cigarettes by some users. However, in the market as currently regulated—as opposed to, for example, use only by prescription in a tobacco cessation programme—ENDS use may be facilitating cigarette initiation and relapse among adults. Nevertheless, ENDS use was relatively low during this period so its impact in either direction was somewhat limited. Only 14% of people who started cigarette use were previously exclusive ENDS users, and only 14% of people stopping cigarette use were previously dual users. Regulatory strategies are needed to minimise the potential harms of ENDS use from catalyst effects and maximise their potential benefits as an aid to smoking cessation. It is also important to emphasise that, while our analysis sheds light on the impact of possible catalyst effects of ENDS use on cigarette use, our analysis is limited to those aged 18 and older and thus excludes those ages when initiation most often takes place. Relatedly, we found that direct switching between exclusive cigarette use and exclusive ENDS was rare. Instead, our analysis suggests that people transition through periods of non-use or dual use. Additionally, transitions directly between dual use and non-current use were negligible. These results suggest that cigarette and ENDS transitions occur separately (if not independently), with one product being started or stopped at a time. If these patterns are borne out in other studies, they could have implications for tobacco control strategies.
We emphasise that a limitation of this analysis is that we are estimating association not causation: because we cannot know what people’s behaviour would have been in the absence of ENDS products, we cannot know the extent to which our results reflect a selection bias.27 28 Those ENDS users starting cigarette use might have also started cigarettes in the absence of ENDS. The high rate of cigarette initiation/relapse among ENDS users in this analysis, then, may only be reflecting a general propensity toward tobacco use of some kind, and the true causal effect of ENDS use on cigarette initiation may be substantially less than the observed association or even be non-existent. Similarly, the high rate of stopping smoking among dual users may reflect a greater interest in ENDS among smokers looking to quit; it may also reflect our limited definition of stopping use (30-day abstinence) as opposed to longer term, sustained quitting. (That being said, the non-current use compartment was relatively stable, with over 80% of non-current users projected to remain so after 4 years.) Moreover, these results do not account for participant’s longer term product use histories, such as previous cessation attempts, which may impact future transitions. While randomised studies of the effect of ENDS on cigarette initiation are unlikely to occur, some randomised trials and observational studies have indicated that ENDS may indeed be effective in helping cigarette users quit,29–32 although some, including US Surgeon General Reports, argue that the evidence to date remains inconclusive.5 33 Other recent analyses of PATH have found strong associations between ENDS use and relapse of cigarette use6 7 and that ENDS use was not associated with long-term abstinence.34 Ultimately, the impact of ENDS use is likely to depend on market regulations. Another related limitation of the current analysis is that we do not account for frequency and intensity of use, the levels of nicotine or the specific ENDS products used, all of which likely influence transition behaviours.
A limitation of the Markov modelling framework itself is the assumption that the rate of transition to future states depends on one’s current state but not on one’s past states. As such, we capture transitions between consecutive waves but not necessarily longer term patterns across multiple waves. For example, a history of failed quit attempts may impact a smoker’s likelihood of trying an ENDS product in the future. Future work may be able to incorporate past use more explicitly into estimates of future transitions or to apply other assumptions about the amount of time spent in each use state (ie, semi-Markov model); more precise transition time data would help future analyses. One final limitation is that this analysis considers only a specific period, approximately 2013–2017, and thus reflects transitions during that period. Both empirical and modelling analysis supported the assumption that transition rates did not change over this period. However, since then, the ENDS product JUUL became widely used and appears to have had a large impact,35 and we expect transition rates to change in future waves.
This work suggests that ENDS use in adults has been less persistent than cigarette use and was associated with both higher cigarette initiation and relapse and at least short-term smoking abstinence. The population impact of ENDS will likely depend on the efficacy of tobacco control policies and interventions to prevent use in non-smokers and facilitate use among current smokers who might not quit otherwise. Although the tobacco product landscape will continue to change, this work is an important step toward developing a nuanced systems approach to estimating how multiple, interdependent factors give rise to future patterns of use and health effects. Ultimately, this work may be used to inform how proposed regulations will shape downstream health effects in the coming decades.
What this paper adds
Previous empirical analysis of Population Assessment of Tobacco and Health study indicated that past 30-day cigarette use is persistent while past 30-day electronic nicotine delivery systems (ENDS) use is less persistent.
The lack of methods for applying multistate transition models to complex surveys has held back more sophisticated analyses of longitudinal tobacco use data.
This study estimated underlying transition rates between tobacco use states. Consistent with previous analysis, we estimate that 90% of cigarette users and 86% of dual users continued to use cigarettes after one wave, while only 72% of ENDS users and 51% of dual users continued to use ENDS after one wave.
We found that ENDS use was associated with both a greater rate of starting cigarette use (more than 20 times that of never users) and a greater rate of stopping cigarette use (about two times that of exclusive cigarette users) among dual users.
Data availability statement
Data are available in a public, open access repository. Data from the PATH study are available for download as Public Use Files in a public, open access repository (https://doi.org/10.3886/ICPSR36498.v10). Conditions of use are available on the website above.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation: RMeza. Data curation: JJ, JLH, EJM. Methodology: AFB, JMGT, RMeza. Analysis: AFB. Original draft preparation: AFB. Review and editing: AFB, JJ, JLH, RMistry, IVB, SRL, TRH, DTL, JMGT, NLF, RMeza. Funding acquisition: RMeza, DTL.
Funding This project was funded through National Cancer Institute (NCI) and Food and Drug Administration (FDA) grant U54CA229974 and the University of Michigan Rogel Cancer Center core grant P30CA046592.
Disclaimer The opinions expressed in this article are the authors’ own and do not reflect the views of the National Institutes of Health, the Department of Health and Human Services or the US government.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.