Article Text

Abstract
Background Menthol cigarettes are thought to encourage smoking initiation among youths and young adults and make it more difficult for smokers to quit, thus increasing cigarette harm. However, no study to date has quantified the damage that menthol cigarettes have caused the US population.
Objective To estimate the excess smoking prevalence, smoking initiation, and mortality in the US from 1980 through 2018 that can be attributed to menthol cigarettes.
Methods Using a well-established simulation model of smoking prevalence and health effects and data from the National Health Interview Survey (NHIS), we first reproduced the overall US adult smoking prevalence between 1980 and 2018 (pseudo-R2=0.98) and associated mortality. Then we re-ran the model, assuming that menthol cigarettes were not present in the market over the same period. Finally, we compared both scenarios to quantify the public health harm attributable to menthol over the 1980–2018 period.
Results From 1980 to 2018, we found that menthol cigarettes were responsible for slowing down the decline in smoking prevalence by 2.6 percentage points (13.7% vs 11.1% in 2018). Our results also show that menthol cigarettes were responsible for 10.1 million extra smokers, 3 million life years lost and 378 000 premature deaths during that period.
Conclusions With millions of excess smoking initiators and thousands of smoking-related deaths due to mentholated cigarettes from 1980 through 2018, our results indicate that these products have had a significant detrimental impact on the public’s health and could continue to pose a substantial health risk. Our findings can assist the Food and Drug Administration in evaluating potential regulatory actions for mentholated tobacco products.
- harm reduction
- public policy
- prevention
Data availability statement
Data are available in a public, open access repository. This study was carried out based on publicly available data sources.
Statistics from Altmetric.com
Introduction
Menthol cigarettes were first created in 1925 by Lloyd Spud Hughesand1 and became widespread in the period between 1957 and 1962.2 Menthol causes a cooling sensation in the throat and airways, reducing the irritation and harshness of cigarette smoke. This characteristic of menthol cigarettes is thought to encourage youth and young adults to initiate smoking and delay smoking cessation.3–5 The 2009 Family Smoking Prevention and Tobacco Control Act gave the Food and Drug Administration (FDA) the authority to regulate the manufacture, distribution and marketing of tobacco products. In particular, it gave the FDA the power to ban menthol in cigarettes. In 2011, the FDA Tobacco Products Scientific Advisory Committee (TPSAC) menthol report6 was submitted to the FDA commissioner and indicated that the availability of menthol cigarettes in the market harmed public health by increasing the number of smokers, with resulting premature death and morbidity.7 In 2013 and again in 2018, the FDA sought public comment, research results and other information on the impact of menthol cigarettes on smoking initiation, prevalence and other factors to inform regulatory actions that the FDA might take for mentholated cigarettes. However, no specific actions for menthol cigarettes have yet been made.
The conclusions of the 2011 TPSAC menthol report were supported by a simulation analysis that compared a projected status quo scenario over the period from 2010 to 2050 with a scenario in which menthol cigarettes were not available over the same time period. To complement that study, we use the same model as in the TPSAC report to estimate the public health harm (measured as excess mortality, smoking initiation and prevalence) that menthol cigarettes have already caused over 1980–2018, a period similar in length to that in the TPSAC report. Our analysis puts in perspective the magnitude of the harm that menthol cigarettes have already caused in the USA and provides the FDA with additional information about the potential danger of those products.
Methods
In this study, we use a well-stablished simulation model of smoking prevalence and health effects (the Mendez-Warner model) to quantify the health impact of menthol cigarettes on the US population during the period from 1980 through 2018. This dynamic model was first introduced by Mendez et al 8 and used extensively in other studies6 9–11 to project the US adult smoking prevalence and smoking-related mortality under different scenarios depicting the impact of potential smoking control policies. A complete description of the model (as modified for the menthol report) is provided in the appendix to the TPSAC menthol report,6 and available also as an online supplemental file to this study. Most of the model parameters were recalibrated and updated to capture accurately the prevalence of menthol and non-menthol smoking in the US adult population over 1980–2018.
Supplemental material
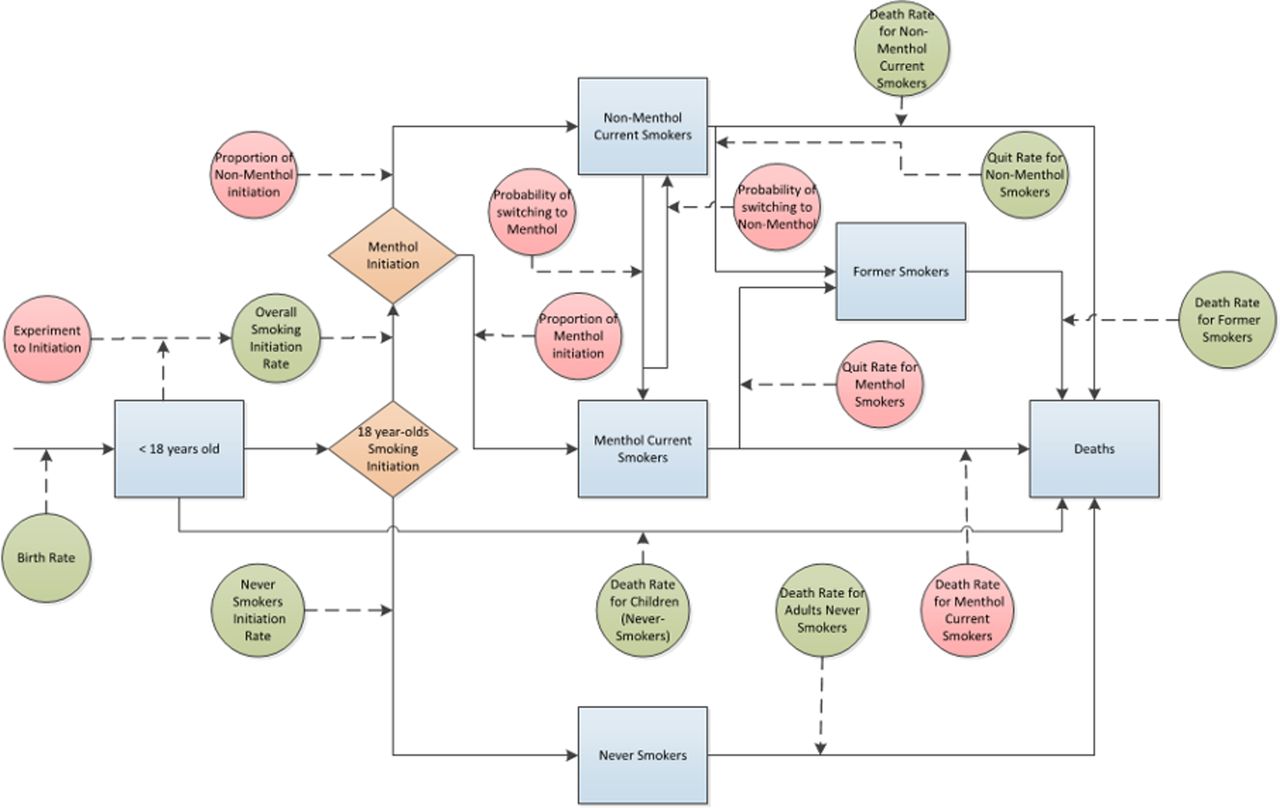
Figure 1 shows the modified Mendez-Warner model used in the TPSAC menthol report and this study. The blue boxes represent the major compartments of the model, tracking the number of adult never smokers, current menthol smokers, current non-menthol smokers and former smokers over time. The circles correspond to the model’s parameters (red for menthol-specific parameters, and green for the rest); the orange diamonds indicate the events of individuals becoming adult menthol, and adult non-menthol, regular smokers.

The dynamics of the menthol cigarettes model.
The dynamics of the model are as follows. A birth cohort corresponding to each calendar year over the period of 1980 to 2018 is introduced into the model using corresponding data from the national vital statistics reports.12 13 Teens are assumed to experiment with cigarette smoking (menthol and non-menthol). Those who never experimented with cigarette smoking, or quit permanently before age 18, are considered never smokers when they reach the age of 18. On the other hand, those who continue smoking into adulthood are given the opportunity to become menthol or non-menthol regular smokers at age 18, regardless of whether they experimented or not with menthol cigarettes as teens. However, those who experimented with menthol as teens have a higher chance of becoming regular smokers (of either menthol or non-menthol cigarettes) at age 18.14
We chose 18 as the age at which to concentrate adult smoking initiation, and used the year-specific National Health Interview Survey (NHIS) reported smoking prevalence for the 18-24 year-olds group (inflated by 20%) as the smoking initiation rate for that year. While most regular smoking had started by age 18, by slightly inflating the 18–24 year old smoking prevalence we capture the small proportion of those who initiated regular smoking after age 18. Those who started to smoke regularly before age 18 are subsumed in the smoking prevalence at age 18.
After age 18, the model keeps track of the number of individuals in each compartment every year, further distinguishing them by age (up to 100) and, in the case of former smoker, by years since they quit (up to 30). Every year, all individuals in the model age by 1 year or die. Additionally, smokers are allowed to switch between menthol and non-menthol cigarettes or quit smoking. The model uses permanent quit rates (net of relapses).
Mortality rates are specific for age and smoking status, further adjusted for years since quitting in the case of former smokers. We did so by combining the age-specific death rates for the general population with relative risks of death due to smoking that are specific for age and smoking status (and specific for years since quitting, in the case of former smokers), derived from Cancer Prevention Study II data.15 The overall death rates by age for the general population were taken from the United States Life Tables and updated every 2 or 3 years over the entire 1980–2018 period. Consistent with Centers for Disease Control and Prevention practice, we assumed no smoking-related mortality before age 35.16
For our analysis, we employed the smoking cessation rates by age estimated by Mendez et al 8 for the 1980 to 1989 period, and the overall smoking cessation rates estimated in Mendez et al 17 for 1990–2018. Since the latter study did not estimate cessation rates by age, we scaled the age-specific cessation rates in Mendez et al,8 to match the average values estimated in Mendez et al.17 Then, we further differentiated the cessation rates for menthol and non-menthol cigarettes, as discussed later.
Menthol-specific parameters (red circles in figure 1) were obtained from published sources. The rates of menthol and non-menthol initiation were computed by applying the proportion of menthol smokers among initiators aged between 18 and 24 years to the overall adult initiation rate using the 1980–2018 NHIS data. The proportion of menthol experimentation was estimated among youths aged 15 to 17 from the National Survey on Drug Use and Health data over 2004–2018. The remaining menthol parameters were kept constant throughout 1980–2018 and are shown in table 1 together with their 95% confidence intervals (CIs) or ±25% of the parameters’ baseline values (for cases without reported CIs).
Menthol specific parameters with 95% CIs
In table 1, the ‘ratio of yields from experimenter to smoker’ (the ratio of the proportion of menthol experimenters who become established smokers to the proportion of non-menthol experimenters who become established smokers) indicates how much more likely a menthol experimenter is to become a regular smoker at age 18 than a non-menthol experimenter. The second parameter in the table is the ‘menthol cessation multiplier’ (the ratio of menthol-smoking cessation rates to non-menthol-smoking cessation rates), which measures how likely a menthol smoker is to quit compared to a non-menthol smoker. The ‘menthol mortality multiplier’, in row 3 of the table, measures the increased risk of death for a menthol cigarette smoker compared with a non-menthol one (taken directly from the TPSAC menthol report.) Finally, the last two rows show the annual switching rates between menthol and non-menthol brands for a particular smoker. These switching rates were taken from the TPSAC menthol report. Menthol and non-menthol smoking cessation rates are age-specific and were calculated using the overall cessation rate, the proportion of menthol smokers among all smokers, and the menthol cessation multiplier (0.76, 95% CI 0.63 to 0.91).18
For this study, we updated all the parameter values used in the TPSAC menthol report, except for the switching rates between menthol and non-menthol cigarettes and the menthol mortality multiplier, for which we could not find more appropriate values.
We used the model to estimate the number of smoking-attributable deaths, life years lost and new smokers for which menthol was responsible between 1980 and 2018. To do so, we first developed a simulation scenario using retrospective NHIS data to reproduce the US smoking trends from 1980 to 2018 (the status quo ante scenario). Then, over the same period, we constructed an alternative (counterfactual) scenario in which menthol cigarettes were assumed to be non-existent over 1980–2018. The smoking initiation rate in the counterfactual case was derived by assuming the same number of experimenters as in the status quo ante scenario but, since now everyone is experimenting with non-menthol cigarettes, a smaller proportion of experimenters become regular smokers at age 18, according to the ratio of yields from experimenters to smokers. In this study, the ratio of yields from experimenters to smokers was taken from the study by Nonnemaker et al (1.80, 95% CI 1.02 to 3.16)14 .
Besides the status quo ante and counterfactual scenarios, in which menthol parameters were set at their baseline values, we performed a sensitivity analysis for each parameter shown in table 1, by setting them at their lower and upper limits indicated in the table. These limits are set by taking the 95% CI for the estimated parameter value, or ±25% of the parameter’s baseline value (for cases without reported CIs). We also performed a Monte Carlo analysis with all parameters being sampled simultaneously from independent normal distributions to produce a 95% confidence band around the estimated smoking prevalence in the counterfactual scenario.
In addition, we examined the individual contributions of changes in initiation and cessation due to menthol to the excess smoking-related deaths and life years lost. To do so, we performed two additional simulation runs, in which we set first the initiation, and then the cessation rate, in the counterfactual scenario to their respective values in the status quo ante scenario.
For each scenario, we computed the number of smoking-attributable deaths as the excess number of deaths for current and former smokers as compared with never smokers.19 The cumulative difference in smoking-attributable deaths between the status quo ante and counterfactual scenarios is an estimate of premature deaths due to mentholated cigarettes. The harm of menthol in cigarettes is also quantified by the cumulative number of life years lost, which is obtained from the cumulative difference in the total population between the two scenarios.

{kind=link}
{kind=link}
Simulated smoking prevalence under status quo ante and counterfactual scenarios and reported NHIS smoking prevalence over 1980–2018. The shaded region shows the 95% confidence band of the estimated prevalence in the counterfactual scenario.
Results
The estimated US smoking prevalence under the status quo ante and counterfactual scenarios, together with the reported NHIS smoking prevalence over 1980–2018, are presented in figure 2. The estimated status quo ante scenario aligns very closely with the observed NHIS data (pseudo-R2=0.98).
The figure shows that, in the absence of menthol cigarettes, the overall US smoking prevalence would have declined from 33.2% to 11.1%, compared with the observed 13.7% in 201820 (a difference of 2.6 percentage points).
Table 2 presents the results of our analysis. The entries in column 1 describe the different scenarios we considered in our simulation runs. Columns 2, 3 and 4 show, for each scenario, the number of excess smoking initiators, cumulative excess premature deaths, and cumulative life years lost, from 1980 to 2018, due to menthol smoking. Row 1 shows the results corresponding to our baseline scenario (i.e., all the model parameters set at their baseline values). Rows 2–11 present the results of the sensitivity analysis for the model’s menthol input parameters (the ratio of yields from experimenter to established smoker, the menthol cessation multiplier, the menthol mortality multiplier, and the switching rates from menthol to non-menthol cigarettes and vice versa). Finally, rows 12 and 13 present the independent contributions of changes in initiation and cessation due to menthol to the results. Scenario 12 displays the impact of the menthol-caused reduction in smoking cessation (by setting the initiation rate of the counterfactual identical to that of the status quo ante), while scenario 13 shows the contribution of increased initiation due to menthol (by setting the cessation rate in the counterfactual identical to that of the status quo ante).
Estimates of cumulative excess smoking initiation, smoking-related deaths and life years lost due to menthol cigarettes over the period 1980–2018
The figures within parentheses below the numbers in all the cells, show the ratio of such numbers to their corresponding baseline values in row 1. Our results show that menthol cigarettes were responsible for 10.1 million extra smokers over 1980–2018 (row 1)—that is, approximately 266 000 additional smokers every year, for the past 38 years. Moreover, nearly 3 million life years and 378 000 smoking-related deaths (i.e., about 9900 premature deaths per year) were caused by menthol cigarettes over the period 1980–2018.
Row 2 shows that the ratio of yields has a considerable impact on the magnitude of the number of new smokers, as well as on the number of premature deaths and life years lost. For instance, a 1.8-fold increase in the ratio of yields (from 1.80 to 3.16) could lead to an approximately 90% increase in the cumulative number of new smokers and a 40% increase in the cumulative number of smoking-related deaths. Furthermore, the analysis shows that the number of smoking-related deaths as well as the number of life years lost are sensitive to the menthol cessation multiplier and the menthol mortality multiplier but not the switching rates. Other things being equal, the decrease in smoking cessation due to menthol cigarettes makes up about 56% of the total number of smoking-related deaths and 65% of the cumulative life years lost due to menthol, while the increase in smoking initiation attributed to menthol cigarettes is responsible for 44% and 36% of the excess deaths and life years-lost due to menthol, respectively.
Discussion
The purpose of this study is to show the magnitude of harm caused by menthol cigarettes in the past as a cautionary tale of the potential future adverse impact of menthol flavour in tobacco products.
Our results show that menthol cigarettes have caused significant population harm over 1980–2018. During that period, we estimate that menthol cigarettes were responsible for approximately 378 000 smoking-related premature deaths, 3 million life years lost and 10.1 million new smokers. Additionally, our sensitivity analysis indicates that the two most important drivers of our results are the relative impact of menthol versus non-menthol experimentation on the transition to regular smoking (the ratio of yields) and the menthol cessation multiplier. While intrinsic differential mortality rates between menthol and non-menthol cigarettes could cause a significant impact on the results, a review of the literature did not reveal direct harm caused by the menthol compound to an individual at the levels found in menthol cigarettes (and other tobacco products). On the other hand, results from empirical research show that individuals who experiment with menthol cigarettes are more likely to become regular smokers, and those who smoke menthol cigarettes are less likely to quit smoking. Thus, our findings imply that the negative impact of menthol on the population’s health is the result of an increase in the initiation rate and a decrease in smoking cessation rate due to menthol (that is, not an individual, but a population health impact). Both changes in initiation and cessation rates contribute significantly to the total harm of menthol cigarettes: smoking related deaths (56% cessation, 44% initiation) and life years lost, (65% cessation, 35% initiation) as shown in table 2. This finding shows that menthol is harmful to both adults (for whom menthol makes quitting more difficult) and youths (who can transition more easily from experimenters to regular smokers and thus nicotine addiction).
Our results indicate that menthol cigarettes have caused significant public health harm across the entire population age spectrum, acting through different pathways. It is true that cigarette smoking has been declining for decades now and is at historically low levels, but menthol in other nicotine delivery products could exert the same effect as in cigarettes, stimulating their diffusion and permanence. As the FDA has expressed interest in the evaluation of a potential menthol flavour ban on some or all tobacco products, our findings can serve to illustrate to the agency the magnitude of the public health problem directly attributable to retaining menthol.
Several factors lend confidence to our results. We used a well-established model in our analysis and provided the model’s detailed formulation to the reviewers and readers of the article; our model calibration produced an almost perfect fit to the NHIS prevalence data over 1980–2018 (pseudo-R2=0.98); and the specific parameters related to menthol came from empirical studies and were obtained after a careful literature search.
However, while we believe that our results reflect accurately the magnitude of the menthol-associated harm to the population, we acknowledge some limitations to our study.
First, we recognise that our results depend on the effect of menthol on the initiation and cessation of tobacco product use. While our sensitivity analysis shows that our results are robust, the uncertainty limits on some of the parameters produce a significant variation in the results. For example, the variability reported for the ‘ratio of yields from experimenter to regular smoker’14 implies a range of uncertainty in the number of deaths averted, ranging from 58% to 140% of its baseline value. This range of uncertainty is not uncommon in simulation studies, but our results should be taken qualitatively as indicators of the magnitude of the overall menthol harm as opposed to precise values. As empirical research provides updated information about the sensitive parameters in the model, we will incorporate them in the analysis to reduce the uncertainty in the results.
Second, we assumed that switching rates between menthol to non-menthol cigarettes remain constant with age, which is not likely to be the case, since older smokers are likely to be more settled in their smoking preferences. However, our analysis shows that our results are not very sensitive to plausible levels of uncertainty on the switching rates.
Finally, we modelled the US general population, and thus our results are applicable to such a group. It is well known that the prevalence of menthol cigarettes is disproportionally high among African Americans. Therefore, menthol harm is certain also to be disproportionally higher among that group. We plan to examine this issue in future research.
What this paper adds
No study to date has quantified the harm that menthol cigarettes have already caused to the US population.
We estimate that menthol cigarettes were responsible for 10.1 million extra smokers, 3 million life years lost and 378 000 premature deaths over the period 1980–2018.
Our results show that menthol in cigarettes is harmful across all age groups.
Data availability statement
Data are available in a public, open access repository. This study was carried out based on publicly available data sources.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TTTL and DM conceptualised the project. TTTL calibrated the model, performed the simulations. DM developed the original model and supervised the work. Both authors contributed to writing of the manuscript.
Funding Research reported in this publication was supported by the National Cancer Institute of the National Institutes of Health and Food and Drug Administration Centre for Tobacco Products (award number U54CA229974).
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or the Food and Drug Administration.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.