Article Text

Abstract
Objective States and localities are formulating strategies to reduce the widespread retail availability of tobacco products. Evidence of associations between retailer density/proximity and tobacco use outcomes can help inform those strategies. We conducted a scoping review on tobacco retail availability and cigarette/e-cigarette use in adults and youth, and considered variations in spatial units, measures of retailer exposure and outcomes across studies.
Methods A systematic search for studies examining the association between retailer density/proximity and youth and adult cigarette/e-cigarette use was conducted across MEDLINE (PubMed), Web of Science and Google Scholar through 27 August 2020 with no restrictions.
Results Thirty-five studies were included in our qualitative synthesis. While there were differences in neighbourhood definitions (eg, egocentric vs administrative), there is evidence for a positive association between higher retailer density in egocentric neighbourhoods around homes and current smoking in adults and adolescents. Administrative unit measures in some studies showed associations with adult current smoking, and adolescent lifetime and current smoking. Studies on tobacco outlet proximity to homes obtained mixed results. Density/proximity of tobacco outlets around schools showed no or inverse association with adolescent smoking, but suggests higher susceptibility to smoking. Evidence of an association between e-cigarette retail availability and e-cigarette use is limited due to a small number of studies.
Conclusion The current literature provides limited empirical evidence of the association between tobacco retailer availability and smoking or e-cigarette use. More research with uniform measures of environmental exposure to tobacco retailers is needed to allow for greater comparability between studies.
- Public policy
- Environment
- Electronic nicotine delivery devices
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Smoking is the leading preventable cause of premature deaths in the USA.1 Nevertheless, tobacco products are still widely available, with the vast majority sold through retail outlets.2 Tobacco retailer density has been linked to smoking among youth and adults.3 4 There are several mechanisms through which retailer density may affect smoking. Higher density may reduce the search costs of finding and purchasing goods,5 6 increase opportunities to purchase tobacco products, and encourage retailers to reduce cigarette prices and increase illegal sales to minors due to increased competition.7 Higher density may further support the ubiquity of smoking8 and increase environmental cues to smoke, whether through point-of-sale displays and advertising,9 or the mere presence of an outlet.10 Widespread availability also increases exposure to retail tobacco marketing and promotions, known to be risk factors for smoking initiation11 and impulse purchases.12 13
The high concentration of tobacco retailers around schools3 14 or in areas with a large proportion of residents younger than 18 years4 raises further concerns, as it exposes youth to high-risk environments during the ages in which the risks of initiation of tobacco use and transitions to daily use are greatest. Given the limited mobility and price sensitivity of youth,15 16 reducing retail density may be a particularly effective strategy to reduce youth smoking.
While there is a growing body of research examining the relationship between tobacco retailer availability and smoking behaviour, there has been inconsistency in the measures used, making comparisons difficult. For example, some studies have focused on tobacco retailer density, others on proximity to retailers. Similarly, some studies have focused on daily smoking, while others have examined smoking within the past 30 days. To date, five reviews have attempted to summarise the evidence on this topic. Notably, four reviews17–20 focused solely on youth and young adults and one did not differentiate between youth and adult studies.21 A meta-analysis17 examined the relationship between retailer density near adolescents’ homes and schools and past 30-day smoking, and did not consider proximity to outlets. A narrative review18 included studies of retailer density and proximity with diverse smoking outcomes, but did not distinguish between exposure near schools versus homes. Systematic19 and methodological20 reviews examined studies on retailer density and proximity near schools and homes and diverse youth smoking outcomes. The conclusions emphasised fundamental challenges in study designs and measures of retailer exposure across studies. A recent methodological review21 examined studies on retailer density and proximity, focusing on the heterogeneity of exposure measures. However, it did not distinguish between youth and adult smoking outcomes, or consider results relative to spatial units or study location (eg, home, school, activity spaces) and did not report effect sizes. None of the prior reviews included studies on e-cigarette use, which has been increasing among US youth since 2011.22 23
The aim of this scoping review is to summarise empirical evidence regarding the association between tobacco retailer density and proximity and the use of cigarettes and e-cigarettes by adults as well as youth. We aim to distinguish findings by population (adult vs youth), various cigarette/e-cigarette use outcomes, spatial units (egocentric buffers vs administrative units) and study locations. In addition, we highlight variations in density/proximity measures, differences in definitions of smoking/e-cigarette use outcomes and control variables used, which may help account for inconsistent findings across studies.
Methods
Literature search strategy
A systematic literature search was conducted on 26 February 2020 across MEDLINE (PubMed), Web of Science and Google Scholar databases, with no restrictions on year of publication, language or article types. The search was updated on 27 August 2020. The first 100 hits on Google Scholar were screened as they were considered to be most relevant to the search topic. Search strings were created via the advanced search builder using text word combinations in the title or abstract relating to retail availability (ie, “retail”, “sale*”, “density”, “proximity”, “distance”, “availability”) and product use (ie, “smoking”, “tobacco use”, “cigarette*, “e-cigarette*”). A three-step selection process was applied. First, two authors (NT and DTL) independently screened titles and abstracts for eligibility. Second, full-text articles of selected abstracts were retrieved from databases and screened for exclusion criteria. Finally, references of full-text articles were examined for additional relevant literature. Disagreements were discussed and resolved by consensus. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist for scoping reviews is available in the online supplemental table S1.
Supplemental material
Inclusion criteria
Empirical studies were included if they examined tobacco retail availability as an exposure variable, and individual-level cigarette or e-cigarette use as an outcome variable (ie, current smoking, ever smoking, initiation, cessation, quit attempts, relapse, as well as intentions to quit and smoking susceptibility (as they are closely related to product initiation and cessation)), with full-text articles in English accessible online. Studies that investigated tobacco product categories that included e-cigarettes (eg, alternative tobacco products) were also included. Tobacco retail availability measures included, inter alia, those described in the PhenX Tobacco Regulatory Project Toolkit, such as density (number of retailers divided by land area or by total population) in person-centred buffers around study participants’ homes, schools or daily activity spaces (ie, egocentric neighbourhoods); density in administrative units (eg, county, city, census tract); and proximity to the nearest tobacco retailer from homes, schools, daily activity spaces, or census area centroids.24
Exclusion criteria
Studies were excluded if they investigated outcomes not related to cigarette or e-cigarette use (eg, normative perception of smoking), used aggregated data to measure use prevalence, or examined associations in subpopulations rather than in the general population (eg, treatment-seeking smokers) to allow for comparability and meaningful interpretation of results. Descriptive geospatial studies that did not aim to provide effect sizes were also excluded.
Data extraction
The following information was synthesised from each study: first author, country, study design, data collection period, sample size, population, tobacco product type, measures of exposure, definitions of spatial units, covariates, tobacco use outcomes and effect sizes.
Qualitative analysis
Given the heterogeneity and limited empirical comparability of studies, a scoping review was selected as the most suitable approach to provide a broad overview of research on the relationship between retailer density/proximity and cigarette/e-cigarette use in both youth and adult populations and map the differences in measures of exposure and outcomes. In contrast to a systematic review, we included all relevant studies, without a priori attempting to synthesise them based on methodological quality.
Results
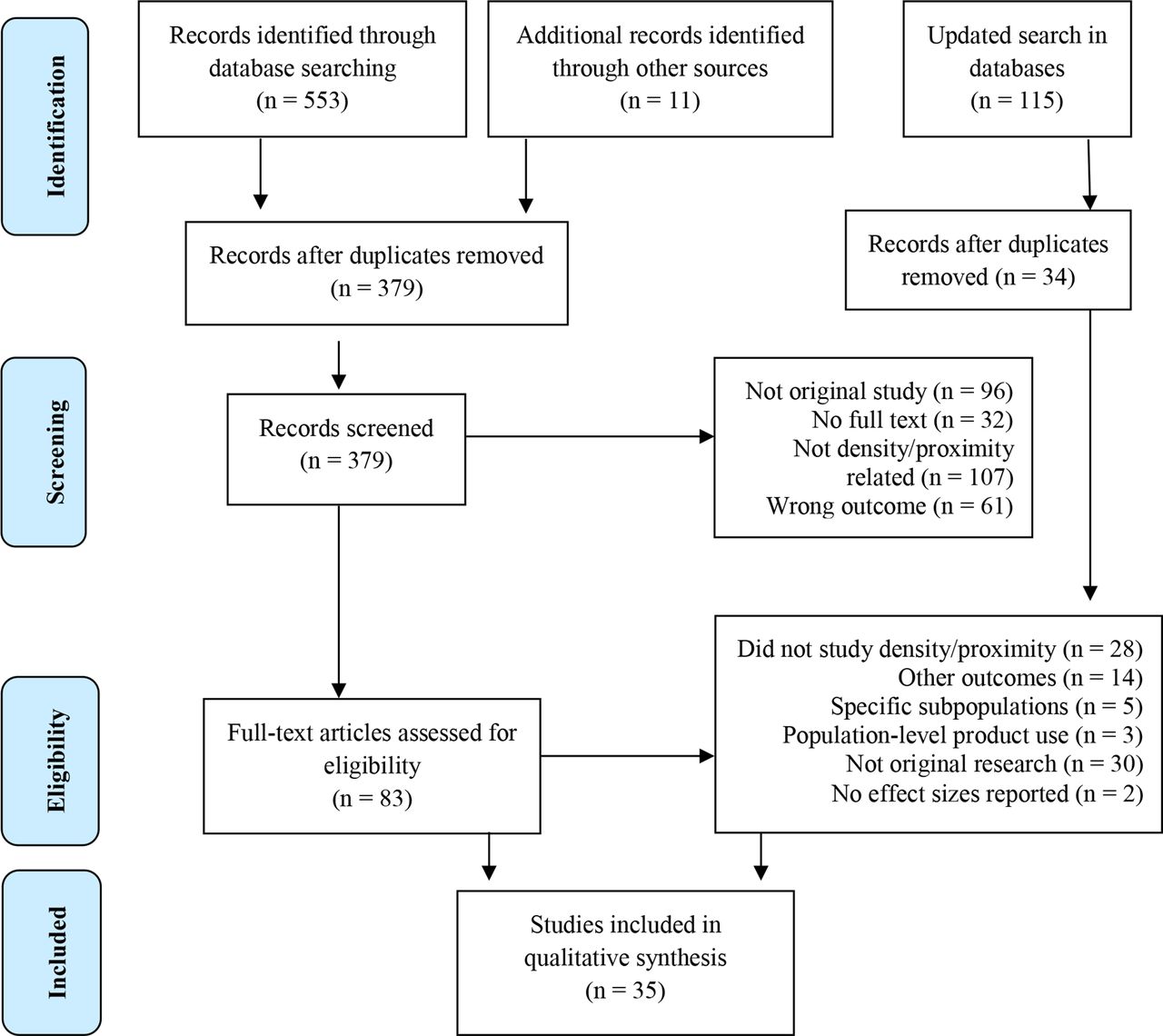
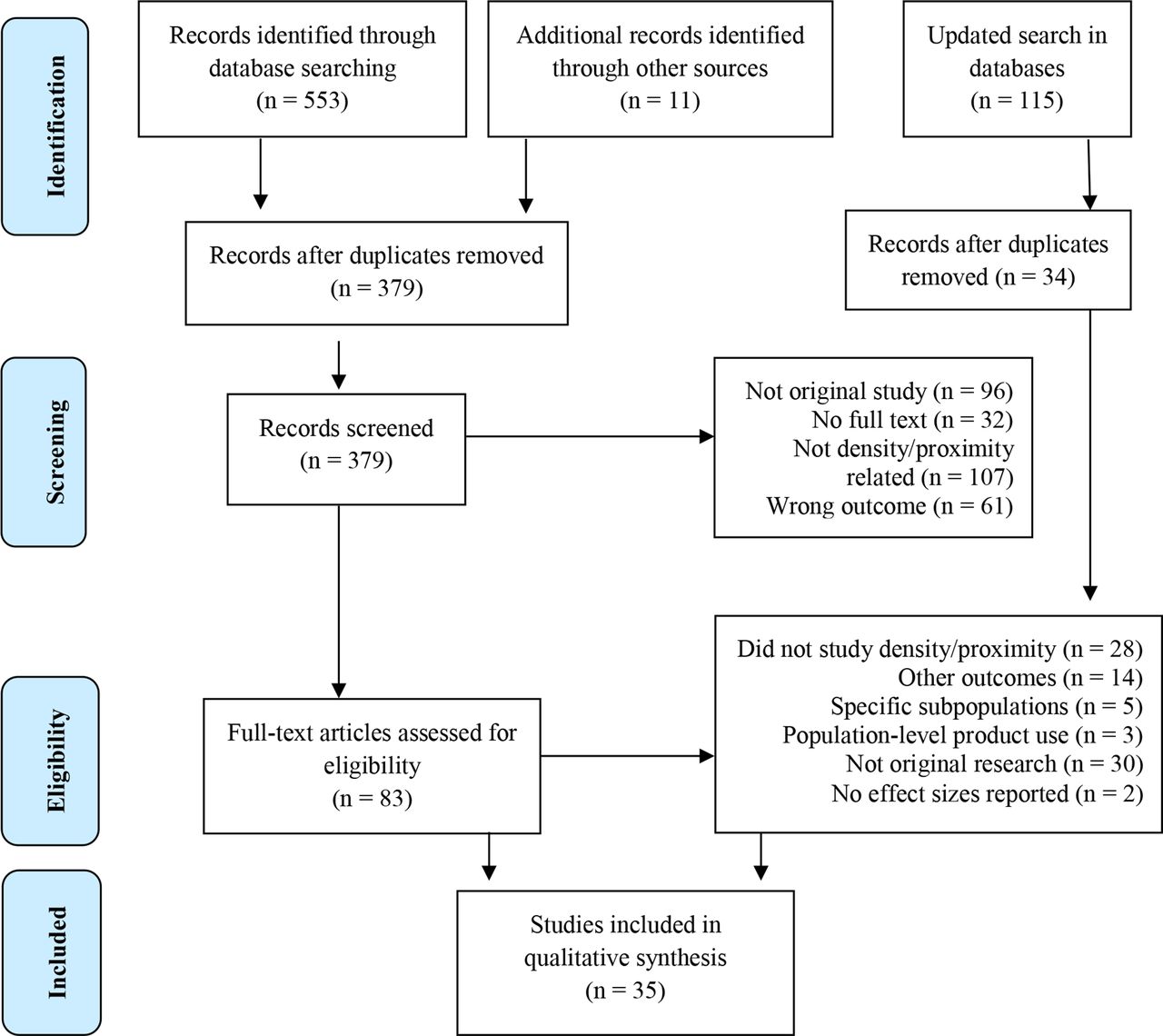
We identified 553 records through the database searches and additional 11 records through manual checks of bibliographies. After removing duplicates, 379 abstracts were screened for eligibility and 296 were excluded. Full-text articles for the remaining 83 records were retrieved and thoroughly assessed for exclusion criteria. An updated literature search following the same methods was performed through 27 August 2020, and identified 34 unique publications, of which 2 were included (figure 1).
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of the selection process for literature review.
Overall, 35 studies, published between 2003 and 2019, were included in the qualitative synthesis (table 1). Most studies (19) were conducted in the USA, while others came from Canada,25–31 New Zealand,32 33 Finland,34 35 Australia3 36 37 and Scotland.38 39 The majority (29) examined cigarette use; few focused on e-cigarettes31 40–42 or on alternative/non-combustible tobacco products that included e-cigarettes.43 44 Nearly half of the studies considered outcomes in adults (15), commonly aged 18+ years, except in three international studies,3 32 38 where adults were defined as 15+ or 16+ years.
Main characteristics of studies on the associations between tobacco retailer density/proximity and adult smoking outcomes
Studies of youth (20) included school-age participants in school-based studies and youth and young adults (ranging from 7 to 23 years old) in home-based and administrative unit-based studies (table 2).
Main characteristics of studies on the associations between tobacco retailer density/proximity and youth smoking outcomes
Overall, person-centred density measures were employed in 8 adult25 26 28 29 35 36 45 46 and 10 youth studies.8 30 31 33 37 41 47–50 Administrative density measures per land area appeared in five adult27 38 43 46 51 and four youth studies,4 39 42 44 and density per population count appeared in one adult3 and five youth studies.9 52–55 Proximity was measured as the shortest distance from home,25 26 28 29 34 35 44–46 49 52 school8 42 49 50 or activity space28 29 to the nearest tobacco retailer in 15 studies, as a presence of at least one retailer per land area in four studies8 25 31 40 and as travel time by car to the nearest retailer in one study.32
Since most studies employed multiple outcomes and measures of exposure (table 3), we grouped results for youth and adult populations by tobacco use outcomes based on the type of retailer exposure (density/proximity) and spatial units (person-centred buffers vs administrative units). Additionally, we specified the types of buffers (circular vs street network) and distances (straight-line vs roadway) used in the analyses.
Measures of tobacco retailer density/proximity across included studies
Retailer density and smoking outcomes in adults
Current smoking
Five cross-sectional studies investigated the relationship between tobacco retailer density and adult current smoking, defined as daily or occasional,3 29 36 ‘smoking at all nowadays’38 and past 30-day smoking27; one cross-sectional study focused on the number of cigarettes smoked per day.46 Using person-centred measures to capture density within 0.5 km street network buffers around participants’ home address or in their daily activity spaces, higher retailer density in residential neighbourhoods was associated with current smoking in two studies from Australia36 and Canada29 with ORs ranging from 1.01 (95% CI: 1.00 to 1.01)36 to 1.53 (95% CI: 1.23 to 1.91; p<0.05),29 and with a prevalence ratio (PR)=1.46 (95% CI: 1.26 to 1.70; p<0.05) for density in daily activity spaces.29 Higher density derived from administrative units, such as a count per 1000 people within census tracts in Australia3 or per square kilometre within residential ZIP codes in Scotland38 was associated with current smoking, with effect sizes ranging from dy/dx (predicted probability)=0.07 (95% CI: 0.05 to 0.10; p<0.01)38 to OR=1.11 (95% CI: 1.02 to 1.21; p=0.018).3 Density per square kilometre within census tracts in a Canadian study was not associated with current smoking.27 In a US study, density within 1-mile circular buffers around homes or per square mile in corresponding census tracts was not related to the number of cigarettes smoked per day.46
Smoking initiation
In a cross-sectional US study, higher retailer density per 10 km of roadway within census tracts was associated with smoking initiation in young adults aged 25–34 years (vs aged 18–24 years) (OR=3.75, 95% CI: 1.18 to 11.90, p<0.05).43
Smoking cessation, quit attempts and relapse
Five studies applied person-centred density measures using circular buffers25 or street network buffers26 28 35 45 around participants’ homes and investigated associations with their cessation outcomes. In two longitudinal studies, density within 500 m buffers was associated with reduced 30-day smoking abstinence, but only in high-poverty neighbourhoods in the USA (OR=0.94; 95% CI: 0.90 to 0.98; p<0.01)45 and with lower quit attempts in high-income (vs lower income) neighbourhoods (OR=0.54; 95% CI: 0.35 to 0.85; p<0.05) and increased relapse (OR=1.11; 95% CI: 1.00 to 1.23; p>0.05) in Canada.25 Smoking cessation was associated with low and intermediate levels of density within 500 m from homes (PR=1.28; 95% CI: 1.10 to 1.50; p<0.05) and daily activity spaces (PR=1.28; 95% CI: 1.08 to 1.51; p<0.05) in a Canadian cross-sectional study,28 and inversely related to higher availability within 500 m only for moderate/heavy male smokers (PR=0.63; 95% CI:0.49 to 0.81; p<0.05) in a longitudinal Finnish study.35 Density within 1 km from home showed no associations with either 30-day abstinence or relapse in a longitudinal Canadian study.26
In two further cross-sectional studies, higher density per square kilometre or square mile within residential ZIP codes was associated with being a former (vs current) smoker in a Scottish study (dy/dx=−0.05; 95% CI: −0.09 to –0.02; p<0.01)38 and with lower intentions to quit in the next 6 months in a US study, but only among price-sensitive, non-daily smokers (likelihood ratio G2=66.1).51
Proximity to tobacco retailers and smoking outcomes in adults
Current smoking
Three cross-sectional studies investigated adult current smoking, variously defined as daily smoking,32 smoking daily or occasionally,29 and the average number of cigarettes smoked per day.46 Proximity from participants’ homes to the nearest retailer, defined as the shortest walking distance (metres) in a Canadian study29 or shortest straight-line distance (miles) in a US study,46 was not associated with current smoking or the number of cigarettes smoked per day. However, shortest walking distance to a tobacco retailer (metres) in daily activity spaces was related to current smoking in a Canadian study (PR=1.42; 95% CI: 1.09 to 1.86; p<0.05).29 In New Zealand, travel time by car from census area centroids to the nearest tobacco retailer was not associated with current smoking, when adjusted for neighbourhood deprivation and rurality.32
Smoking cessation, quit attempts and relapse
Of six studies that assessed proximity from home to the nearest tobacco outlet, three measured walking distance (metres),25 28 45 two measured straight-line distance (metres, kilometres)26 34 and one compared both.35 All studies but one were longitudinal. A greater walking distance was associated with higher odds of 30-day smoking abstinence in a US study, but only in high-poverty areas (OR=2.80; 95% CI: 1.51 to 5.19; p<0.001)45; and was otherwise unrelated to quit attempts and relapse in one Canadian study,25 and to smoking cessation in another cross-sectional Canadian study.28 However, the same measure in daily activity spaces was associated with smoking cessation (PR=1.21; 95% CI: 1.02 to 1.43; p<0.05).28 In studies from Finland34 and Canada,26 greater straight-line distance from home to the nearest tobacco retailer was positively associated with smoking cessation (OR=1.16; 95% CI: 1.05 to 1.28; p=0.004),34 but not with 30-day smoking abstinence26 or relapse.26 34 In another Finnish study, smoking cessation was inversely associated with closer proximity using both measures, but only in moderate/heavy male smokers (PR=0.73, 95% CI: 0.60 to 0.88; p<0.05).35
Retailer density and adolescents’ smoking outcomes
Current smoking
Adolescent current smoking was defined in seven cross-sectional studies as past 30-day smoking,4 9 49 53 55 smoking ‘at all nowadays’39 or ‘any cigarette use on a given day’.48 All but one study39 were conducted in the USA. Greater density within 0.75-mile circular buffers around homes was associated with higher smoking frequency (β=0.293; SE=0.069; p≤0.05).49 Density within 100 m of daily activity space polylines was not associated with youth smoking in a study that used real-time geographical ecological momentary assessment.48 While density per square kilometre within residential ZIP codes39 and within census tracts4 was positively associated with increased smoking, with ORs ranging from 1.20 (95% CI: 1.01 to 1.44) to 1.47 (95% CI: 1.13 to 1.91; p<0.01), larger administrative measures, such as county-level density per 1000 people (aged 17 years and younger)9 55 and city-level density per 10 000 people,53 showed no associations.
Lifetime smoking
Adolescent lifetime smoking was defined in five studies as ever smoking a cigarette,39 52 ever trying a cigarette (even one puff)8 and ever smoking a whole cigarette (more than just a few puffs).53 54 Most studies were cross-sectional and conducted in the USA, except for one longitudinal study54 and one conducted in Scotland.39 Higher retailer density within 0.5 mile of egocentric road network buffers around homes was associated with higher odds of lifetime smoking (OR=1.01; 95% CI: 1.00 to 1.02; p<0.05).8 Administrative measures, such as density per square kilometre in residential ZIP codes (OR=1.53; 95% CI: 1.27 to 1.85; p<0.001)39 and density per 10 000 population in cities (OR=1.12; 95% CI:1.04 to 1.22; p<0.01 and OR=1.312; 95% CI: 1.041 to 1.655; p≤0.05)53 54 also correlated with lifetime smoking, while nationwide density per 1000 persons showed no associations.52
School-level retailer density and adolescents’ smoking outcomes
Current smoking
Eight cross-sectional studies considered adolescent current smoking, defined as past 30-day smoking,37 42 47 49 past 30-day smoking and more than 100 cigarettes in a lifetime,33 50 occasional or daily smoking,30 or smoking ‘at all nowadays’.39 Smoking was not associated with higher retailer density in egocentric buffers around schools in three US, one Canadian (Ontario) and one Australian (Victoria) studies,30 37 47 49 50 and inversely associated with higher density within 500 m road network buffers in one New Zealand study (OR=0.75; 95% CI: 0.65 to 0.87; p<0.05).33 An administrative measure of density per square mile around schools in the USA showed no association,42 while density per square kilometre within school ZIP codes in a Scottish study (OR=0.75; 95% CI: 0.59 to 0.95; p<0.05)39 showed an inverse relationship.
Lifetime and experimental smoking
Five cross-sectional studies considered adolescent lifetime smoking, defined as ever smoking a cigarette39 47 or ever trying a cigarette (even one puff),8 or experimental smoking, defined as past 30-day smoking and having smoked less than 100 cigarettes in a lifetime.33 50 In two US studies, higher densities within 0.5-mile and 1-mile circular buffers around schools were associated with adolescent lifetime smoking (OR=1.10; 95% CI: 0.99 to 1.20; p=0.51),47 and with experimental smoking (OR=1.11; 95% CI: 1.02 to 1.21) only for high school students in urban areas.50 Density within 0.5-mile, 500-metre and 1-kilometre road network buffers around schools showed no association with lifetime smoking in the USA8 or experimental smoking in New Zealand.33 In one Scottish study, higher density per square kilometre within schools’ ZIP codes was inversely associated with lifetime smoking (OR=0.66; 95% CI: 0.50 to 0.86; p<0.01).39
Susceptibility to smoking
Susceptibility to smoking (intention to try a cigarette soon or in the next year or if offered to try by a best friend) was associated with higher density within 1 km circular buffers in a cross-sectional Ontario study (OR=1.03; 95% CI: 1.01 to 1.05; p<0.05)30 and within 1 km road network buffers around schools in a cross-sectional New Zealand study (OR=1.07; 95% CI: 1.01 to 1.16; p<0.05).33
Retailer proximity to homes and adolescents’ smoking outcomes
Retailer proximity to schools and adolescents’ smoking outcomes
Current smoking
Three cross-sectional US studies examined current adolescent smoking, defined as past 30-day smoking42 49 or past 30-day smoking and more than 100 lifetime cigarettes50 and retailer proximity to schools, measured as a straight-line distance in feet50 or in miles49 and street network distance.42 None found significant associations.
Lifetime and experimental smoking
Two cross-sectional US studies explored the relationship between retailer proximity to adolescents’ schools, defined both as a distance in roadway miles, and the presence of at least one outlet within 1000 ft,8 or as a straight-line distance,50 and lifetime smoking or experimental smoking. Neither found an association.
E-cigarette retailer density/proximity and e-cigarette use
Four cross-sectional studies investigated the density of e-cigarette retailers near schools and adolescent lifetime and/or current (past 30-day) use. In a US study, a count of tobacco retailers that sold e-cigarettes within a 0.5-mile circular buffers around schools was associated with current use (adjusted PR (aPR)=1.04; 95% CI: 1.01 to 1.08; p<0.05) and lifetime use (aPR=1.03; 95% CI: 1.00 to 1.05; p<0.05).41 However, the number of vape shops within 0.5, 1.0 and 1.5 km circular buffers was not associated with current or lifetime use in a Canadian study.31 In a US study, the number of e-cigarette retailers per square mile within schools’ ZIP codes was not related to current use among students.42 Proximity, defined as a presence of at least one e-cigarette specialty store within a 0.25-mile buffers from schools, was only associated with lifetime use in middle school students (vs high school students) (OR=1.70; 95% CI: 1.02 to 2.83) and not associated with current use.40 In a Canadian study, the presence of at least one e-cigarette retailer within 0.5, 1.0 and 1.5 km circular buffers around schools was not associated with lifetime or current use.31 In a US study, walking distance from school to the closest e-cigarette retailer was not associated with students’ current e-cigarette use.42
While no studies examined the initiation of e-cigarettes (exclusively), two considered initiation of alternative/non-combustible tobacco products (including e-cigarettes) among youth and young adults. A longitudinal study in the USA showed that living in census tracts with higher tobacco retailer density per square mile was positively associated with adolescents’ initiation of alternative tobacco products (OR=1.22, 95% CI: 1.07 to 2.12), but no association was found for retailer proximity from home measured in roadway miles.44 In a cross-sectional US study, living in tracts with higher tobacco retailer density (count per 10 km of roadway) was not associated with non-combustible product initiation in young adults.43
Discussion
Our scoping review summarises evidence on the association between tobacco retailer availability and the use of cigarettes and e-cigarettes in adults and adolescents, while considering variations in tobacco use outcomes and measures of density/proximity.
For adults, evidence from cross-sectional research showed a positive association between current smoking and both person-centred measures around homes (two of two studies)29 36 or in daily activity spaces (one of one)29 and administrative units (two of three)3 38 of retailer density. Evidence on the relationship between current smoking and retailer proximity to homes, daily activity spaces or administrative unit centroids was more limited (one of three).29 There was also evidence, mainly from longitudinal studies, of associations between higher person-centred density near homes and lower smoking cessation (two of two),28 35 quit attempts (one of one),25 30-day abstinence (one of two)45 and higher relapse (one of two).25 However, these associations were usually limited to specific populations, such as price-sensitive non-daily smokers,51 moderate/heavy male smokers,35 or residents of high-poverty45 or high-income neighbourhoods.25 Farther retailer proximity from homes showed associations with higher cessation (two of three),34 35 but was not related to smoking relapse (none of three).
For adolescents, evidence gathered from predominantly cross-sectional research indicated a positive association of person-centred measures of retailer density near homes and daily activity spaces with current smoking and the number of cigarettes smoked (two of two),48 49 as well as lifetime smoking (one of one).8 For administrative units, there was some evidence of a positive association with density and current smoking (two of five),4 39 but evidence for lifetime smoking was more consistent (three of four).39 53 54 Higher density near schools showed no or inverse association with adolescent current smoking, but was related to greater susceptibility to smoke (two of two).30 33 There was no evidence that retailer proximity to homes or schools was related to adolescent smoking.
Given e-cigarettes’ popularity among youth, research on association of use with retail density/proximity of e-cigarettes is surprisingly scarce. Existing studies focused on e-cigarette retailer availability near schools and suggest that adolescent current e-cigarette may be related to retailer density (one of three),41 but not proximity (none of three). Inadequate data about which tobacco retailers sell e-cigarettes are an obstacle to research on this topic. Studies of vape shops (that sell e-cigarettes exclusively) may underestimate retail availability of e-cigarettes, while studies of all tobacco retailers surely overestimate it.
Our findings are consistent with a meta-analysis that found a small but significant positive relationship between tobacco retailer density around adolescents’ homes (but not schools) and past month smoking.17 While results of a narrative review18 were inconclusive due to heterogeneity and small number of included studies, systematic19 and methodological20 reviews also found some support for a positive association of youth smoking with higher retailer density around homes, but not with proximity to homes or schools. A recent methodological review21 concluded that there was an overall positive relationship between tobacco retailer density and smoking prevalence and initiation, with retailer proximity inversely related to smoking cessation. However, these findings did not distinguish between adult and youth smoking outcomes or the location of retailer exposure, thus limiting comparability of included studies and a meaningful interpretation of results. In contrast, our review provides a more comprehensive analysis, highlighting that while tobacco retailer density/proximity around homes and in activity spaces is related to both adolescent and adult smoking, retailer availability around schools is not (or inversely) related to adolescent smoking prevalence, but rather to susceptibility to smoking and cigarette experimentation.
Variation in measurements of retailer density/proximity across studies may partially explain the inconsistent evidence, since inaccurate definition of neighbourhoods contributes to spatial misclassification of exposure. Administrative definitions of neighbourhoods are more common and convenient, but assuming the same exposure for all individuals may mask true associations. Egocentric definitions of neighbourhoods or activity spaces are optimal to estimate individual-level retailer exposures, but the data are more difficult to obtain. Although circular buffers are more commonly used to define egocentric neighbourhoods, street network buffers better reflect real-life settings since they account for physical barriers.56 Similarly, roadway distance or travel time is a more appropriate measure of proximity as opposed to straight-line distance,35 but they require data about participant locations (home, work, school) that can be difficult to obtain.
In this review, most studies with adult participants focused on retailer density in egocentric neighbourhoods, using street network buffers around home or constructed activity spaces, while several opted for administrative measures per land area, particularly in census tract and residential ZIP codes. In adolescent studies, density measures within egocentric circular buffers near schools and in administrative units relative to population count were more commonly employed. These measures were generally consistent with recommendations of the PhenX Toolkit for tobacco regulatory research,24 and similar to the findings of the recent methodological review,21 none provided a clear advantage in revealing associations. Retailer proximity for both populations was commonly measured as the shortest road network distance or straight-line distance to the nearest retailer. Less common measures that were not included in the PhenX Toolkit, such as travel time by car, or presence of at least one retailer within a certain distance, were used, but did not show a significant advantage in revealing associations.
Differences between local or national tobacco policies across study settings may further limit comparability and partially explain null findings. Compliance with youth access laws, for example, may mitigate/moderate the relationship between retail density and adolescent smoking.33 39 Smoke-free air policies have also been shown to moderate this association.53 However, with the exception of a few studies,43 47 53 the effects of such policies have not been accounted for. Another moderating influence may be point-of-sale advertising and display bans, which are effective in reducing smoking in adolescents57 58 and adults59 and therefore are likely to be another moderating influence. Notably, studies from Quebec, Canada and Finland, where point-of-sale advertising restrictions have long been in place, still found retailer density/proximity associated with lower adult cessation rates,28 34 35 suggesting that retail availability affects smoking behaviour independent of advertising exposure. Finally, given that racially diverse and socioeconomically disadvantaged neighbourhoods have significantly higher density of tobacco retailers,3 4 34 60 61 the relationship between retailer density and individual smoking behaviour is likely modified by neighbourhood socioeconomic status (SES),46 which many studies did not address. Inconsistent findings may also be attributed to the different operational definitions of this concept across studies. Future research should also include spatial measures that better capture racial residential disparities, such as historical redlining.62
Increasingly, jurisdictions are implementing policies to reduce the spatial availability of tobacco products.63 64 Evidence is beginning to emerge regarding their impact on tobacco use,65 66 although it may take years before changes may be seen at the population level.67 Simulation models examining the impact of various retail restrictions estimate reduced smoking prevalence and health benefits.5 68–70 However, evidence suggests that there is no standard approach to retailer reduction policies, and their effects may vary across different settings.6
Overall, this review supports the view that reducing tobacco retailer density may help reduce adult and youth smoking prevalence. To our knowledge, this is the first review to consider the relationship between tobacco retailer availability/accessibility in different geographical settings and cigarette and e-cigarette use by adolescents and adults. An important strength of this review is that it considered multiple tobacco use outcomes and compared various measures of density and proximity. However, the review has several limitations. Since the emphasis of this scoping review was to provide a comprehensive overview of the current literature regardless of the standard of evidence, the critical assessment of the quality of included studies was not performed. This limits our ability to provide concrete guidance to inform policymaking. Further, most studies were cross-sectional, making it difficult to distinguish whether increased retail density/proximity increases the odds of smoking, or whether tobacco retailers are locating their businesses in response to high market demand. Nevertheless, evidence from longitudinal studies suggests a causal effect of living in areas with densely distributed tobacco retailers or in their close proximity and decreased adult cessation.34 35 Finally, while some studies had a fixed neighbourhood buffer zone to measure retailer density, others chose increasing intervals of buffers. In such studies, we reported a buffer size closest to the one across the included studies for the purpose of comparability, which may have biased the results. Future research should consider sensitivity analysis regarding buffer sizes used across studies, perhaps separately for urban and rural areas. A uniform grid unit method for geospatial distribution of tobacco retailers, with larger grid units in rural versus urban areas, is recommended.71 Tobacco retail accessibility may play an important role in individual smoking behaviour, particularly in rural areas,72 but remains largely unexplored. Specific measures of retail accessibility, such as travel time by car, should be considered in the PhenX Toolkit of recommended measures for tobacco regulatory research.
Conclusion
This scoping review finds some evidence of an association between tobacco retailer availability and smoking outcomes in youth and adults. More research is needed, particularly of longitudinal design, with representative samples, uniform measures of exposure and outcome variables, and consistent inclusion of major individual and area-level characteristics, such as racial diversity and neighbourhood SES. Quasi-experimental before–after studies are also needed to fill the gap in evidence regarding causality between retailer density/proximity and outcomes in youth and adults. Studies on the risk of cigarette initiation and tobacco retailer availability are particularly scarce and should be the focus of future research. Finally, studies examining associations between retailer availability and e-cigarette use are scarce and further research is warranted.
What this paper adds
Limiting tobacco retail availability may be an effective tobacco control strategy to reduce smoking and improve public health. Evidence on the associations between tobacco retailer density/proximity and cigarette/e-cigarette use is mixed and inconsistencies in measures of retailer exposure across studies have been reported. There was a need for a comprehensive literature review to summarise the existing evidence for both youth and adults and highlight the methodological gaps.
This review suggests that tobacco retailer density, but not proximity, may be a contributing factor in promoting smoking among youth and adults. In particular, future tobacco control policies limiting retailer exposure in residential areas may be successful in reducing smoking, while reducing tobacco retailer availability around schools may not be as effective. Research on e-cigarette use and density/proximity of e-cigarette retailers is surprisingly scarce, given their popularity among youth. There is a need for more research with representative samples, uniform measures of exposure and outcome variables, and consistent control for major area-level characteristics, such as racial diversity and neighbourhood disparity.
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors DTL and NT came up with the idea for the article. NT performed the literature search, wrote the article, has access to all data and is the guarantor for the finished article. PAM, DTL and LH made substantial contributions to the conception of the work and the interpretation of findings. All authors participated in the review and final approval of the manuscript.
Funding This research was funded by a grant from the National Cancer Institute (1R01-CA229238, PI: Ruth E Malone).
Disclaimer The opinions expressed in this article are the authors’ own and do not reflect the views of the National Institutes of Health, the Department of Health and Human Services, or the US government.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.