Article Text

Abstract
Introduction The US Food and Drug Administration most recently announced its intention to ban menthol cigarettes and cigars nationwide in April 2021. Implementation of the ban will require evidence that it would improve public health. This paper simulates the potential public health impact of a ban on menthol in cigarettes and cigars through its impacts on smoking initiation, smoking cessation and switching to nicotine vaping products (NVPs).
Methods After calibrating an established US simulation model to reflect recent use trends in cigarette and NVP use, we extended the model to incorporate menthol and non-menthol cigarette use under a status quo scenario. Applying estimates from a recent expert elicitation on the behavioural impacts of a menthol ban, we developed a menthol ban scenario with the ban starting in 2021. We estimated the public health impact as the difference between smoking and vaping-attributable deaths and life-years lost in the status quo scenario and the menthol ban scenario from 2021 to 2060.
Results As a result of the ban, overall smoking was estimated to decline by 15% as early as 2026 due to menthol smokers quitting both NVP and combustible use or switching to NVPs. These transitions are projected to reduce cumulative smoking and vaping-attributable deaths from 2021 to 2060 by 5% (650 000 in total) and reduce life-years lost by 8.8% (11.3 million). Sensitivity analyses showed appreciable public health benefits across different parameter specifications.
Conclusions and relevance Our findings strongly support the implementation of a ban on menthol in cigarettes and cigars.
- advocacy
- electronic nicotine delivery devices
- public policy
- smoking caused disease
Data availability statement
Data are available upon reasonable request. The model and data will be provided upon request. The model and data will be provide upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
While US cigarette smoking prevalence has declined substantially in the past decade, the prevalence of menthol smoking has remained constant.1–5 Menthol cigarettes now represent 35% of cigarette sales6 and are disproportionately used by youth, young adults, women and African-Americans.3 7 Menthol cigarette use has been associated with increased smoking initiation and reduced smoking cessation.8–11 In response, the European Union, Canada, Brazil, Ethiopia and Turkey have banned menthol in cigarettes.12 In the USA, more than 20 localities and the state of Massachusetts have banned menthol cigarettes.13 Recently, the Food and Drug Administration announced its intention to implement a nationwide ban on menthol in cigarettes and cigars.14 A stronger evidence base is urgently needed about whether such a ban would improve public health.15 16
A small body of research has examined the potential impact of banning menthol in cigarettes. A simulation model17 projected that a menthol ban would have major impacts on smoking prevalence and smoking-attributable deaths. However, that model simulated a ban starting in 2010 and did not consider the impact of switching to nicotine vaping products (NVPs, also known as e-cigarettes). Additionally, recent evidence finds that a menthol ban would likely increase smoking cessation, with more limited evidence of reducing smoking initiation and switching from smoking to other products.18 To better gauge the potential impact of a menthol cigarette and cigar ban in the vaping era, we conducted an expert elicitation to explicitly consider the impact of the ban on smoking initiation and cessation and on NVP use.19
This paper applies the results of our expert elicitation to evaluate a US menthol ban on all combustibles, including cigarettes and cigars. We use the previously developed smoking and vaping model (SAVM)20 to simulate the impact of the ban on cigarette and NVP use. We extend that model to distinguish menthol and non-menthol cigarette use and to estimate the public health impact of a menthol ban on combustible tobacco products.
Methods
The SAVM is a compartmental model that simulates the public health impact of cigarette and NVP use over time for a specific set of birth cohorts in a given population.20 The model is publicly available as a Microsoft Excel file with a user manual.21 We extend SAVM to project menthol and non-menthol cigarette use in the absence of a ban (status quo scenario) and in the presence of a ban (menthol ban scenario). We estimate the public health impact as the difference in smoking and vaping-attributable deaths (SVADs) and life-years lost (LYLs) between scenarios. Further description of the model and model equations are found in online supplemental file 1.
Supplemental material
Status quo scenario
The SAVM20 first projects never, current and former smoking prevalence using age and sex-specific initiation and cessation rates for each cohort of males and females by individual age (0–85) beginning in 2013. The model parameters were estimated by applying an age-period-cohort statistical smoking model to National Health Interview Survey (NHIS) data through 2013,22–25 thereby incorporating trends before NVP use became more prevalent in 2013.26 Current smoking is defined as having smoked ≥100 cigarettes during one’s lifetime and currently smoking at least some days. Current smokers become former smokers after having quit for 2 years to reflect cessation net of relapse. Future smoking prevalence is based on the estimated initiation and cessation rates.
Overlaying the smoking model, SAVM incorporates switching from smoking to regular NVP use, NVP initiation and cessation, and smoking initiation and cessation.20 To simplify the analysis and because dual use is often unstable,27–31 dual users of cigarettes and NVPs are included in SAVM as current smokers.30 Those who vape de novo or who switch from smoking to vaping before age 35 are treated as exclusive vapers, reflecting the minimal smoking-related mortality risks of smokers who quit by age 35.32 33 Those who switch from smoking to vaping after age 35 become former smokers who vape.
An earlier version of the SAVM generally validated well,20 but underestimated the decline in smoking. Given the importance of smoking initiation to future smoking rates, we recalibrated model parameters using 2013–2018 NHIS data, as described in online supplemental file 1.
To incorporate menthol use, we differentiate menthol and non-menthol smokers in the model by age and gender. Using data from the 2013/2014 to 2016/2017 Population Assessment of Tobacco and Health (PATH) study, menthol smokers are defined as those whose regular brand is flavoured to taste like menthol.34 Transitions in the status quo scenario are illustrated in figure 1.

Transitions between smoking and nicotine vaping product (NVP) use states in the status quo scenario.
Smoking initiation rates for menthol and non-menthol smokers are determined assuming a constant proportion of menthol smokers among all smokers at age 30 (MP30), an age when most initiation and smoking patterns have become established.35 36 Based on our analysis of PATH data (see online supplemental file 2), less than 3% of smokers switch between menthol and non-menthol cigarettes or initiate smoking after age 30. Using PATH data for ages 25–35, MP30 is estimated as the average proportion of menthol smokers and is applied to smoker initiation rates at each age a in year t as:
Supplemental material


While this method does not explicitly model differences in the trajectories of menthol and non-menthol use prior to age 30, it implicitly allows for initiation as well as switching between menthol and non-menthol use through age 30.
Age and year-specific cessation rates of menthol and non-menthol smokers are based on transforming overall cessation using the menthol proportion at each age (MPa) and the ratio of the menthol to non-menthol cessation rates (RMNCr), yielding:


Based on recent studies11 37–41 and PATH data, we set RMNCr=0.8 for all ages and both genders.
To allow for different switching rates from menthol and non-menthol smoking to NVP use, we apply a similar method using the ratio of menthol to non-menthol switching (RMNSw). We assume that switching rate declines annually by 10% beginning in 2018 (to reflect that those most amenable to vaping have already switched).


Based on recent PATH data, we set RMNSw at 0.9 for all ages and both genders.
Given limited evidence of differential mortality,42 43 we assume no difference in the mortality rates of menthol and non-menthol smokers.
Online supplemental file 1 shows projected trends. The proportion of menthol smokers among all smokers shows an upward trend, consistent with trends reported in recent studies.1–6
Menthol ban scenario
We model a federal menthol ban beginning in 2021. While the model focuses on cigarette use, the ban is assumed to apply to both cigarettes and cigars. We focused on the effect of a ban on both, since little cigars have been found to be a close substitute for cigarettes.44–46 Were cigars (especially little cigars) exempted, many preban menthol cigarette smokers would likely switch to menthol cigars.
We rely on the aforementioned expert elicitation.19 Finalised in September 2020, the elicitation was specifically developed to assess the impact of a menthol ban on smoking initiation and cessation and on NVP use.19 The panel of experts was selected using a three-pronged approach: (1) selection of lead and senior authors of studies identified in a scoping review on the impact of menthol and flavour bans18; (2) a search in Scopus to identify individuals who are the most published authors on the topic of menthol tobacco and with an H-Index of ≥20; and (3) the advice of an external advisory panel. After selecting 12 of the 82 experts with the highest rated criteria 1 and 2 above and with no reported conflicts of interest, our final sample comprised 11 experts after one invitation was declined.
Experts were asked to estimate transitions regarding current tobacco and NVP use patterns under a menthol cigarette and cigar ban, including continued (illicit) menthol cigarette or cigar smoker47; switching to non-menthol cigarettes or cigars, smokeless tobacco or novel nicotine delivery products (NNDPs, including NVPs and heated tobacco products); or ceasing all nicotine product use. Because mortality risks for cigars are similar to or less than those for cigarettes,48 49 estimated panel transitions into cigar use are modelled as non-menthol cigarette use. For convenience, the small percentage of estimated transitions to smokeless tobacco use (2% for ages 18–24 and <1% for ages 35–54) is also transferred to non-menthol cigarette use. Although the elicitation included heated tobacco products in NNDPs, we treat all such transitions as NVP use based on relatively similar risks.50–52 The elicitation methodology and results are described further in online supplemental file 2.
The experts first estimated the impact of a menthol ban on smoking initiation for those aged 12–24 who, absent a ban, would have initiated menthol smoking by age 24. Based on experts’ mean estimates, 38.3% of otherwise menthol smokers would instead become non-menthol smokers, 2.4% illicit menthol smokers, 17.3% NVP users and 42.0% would not use cigarettes or NVPs. These adjustments are applied to the initiation rates of otherwise menthol smokers in 2021 and as ongoing transitions in future years.
For those already menthol smokers, experts considered transitions over a 2-year period under the status quo and under a menthol ban. We model the experts’ estimates of mean net transitions (the difference in 2-year transitions under the status quo and a menthol ban). Among current menthol smokers aged 18–24, 10.1% switch to illicit menthol combustibles, 48.0% switch to non-menthol combustibles, 24.2% switch to NVPs and 17.7% quit all product use. These transitions are applied to menthol smokers through age 30. Among current menthol smokers aged 35–54, 8.8% switch to illicit menthol cigarettes and cigars, 59.1% switch to non-menthol tobacco use, 17.3% switch to NVPs and 14.7% quit all product use. These transitions are applied to menthol smokers above age 30. Current non-menthol smokers were assumed to be unaffected by the ban.
Public health outcomes
Smoking-attributable deaths are estimated as the excess mortality risk at each age for current and former smokers multiplied by their respective populations. Vaping-attributable deaths are measured in the same way, except vaping excess mortality risk is initially set at 15% of excess smoking risk, higher than previously published estimates.53 54 Total LYLs are estimated at each age by the number of SVADs multiplied by the expected years of life remaining of a never smoker.
We estimate the public health impact of a menthol ban as the differences in SVADs and LYLs in the status quo and menthol ban scenarios over a 40-year period, 2021–2060. To address uncertainties about the values of variables applied to both scenarios, we conduct sensitivity analyses of the public health impacts with excess mortality risks of NVPs at 5% and 25% that of excess smoking risks, with smoking and NVP initiation and cessation transitions and rates of switching from cigarettes to NVPs varied by −10% and +10% of their baseline levels and with the ratio of menthol to non-menthol cessation and menthol to non-menthol switching equal to 1.
Results
Public health impact under the base case status quo and menthol ban scenarios
Table 1 presents the 2021–2060 menthol and non-menthol smoking and NVP prevalence, SVADs and LYLs from the model for US adults (aged >18), males and females combined (weighted by population). Results from 2026 and 2060 are presented to display illustrative short-term and long-term status. Online supplemental file 3 provides breakdowns by gender and with the time period extended from 2060 to 2080.
Supplemental material
Smoking and NVP prevalence, smoking and vaping-attributable deaths, life-years lost and public health impact for both genders combined, age 18 and above, 2021–2060
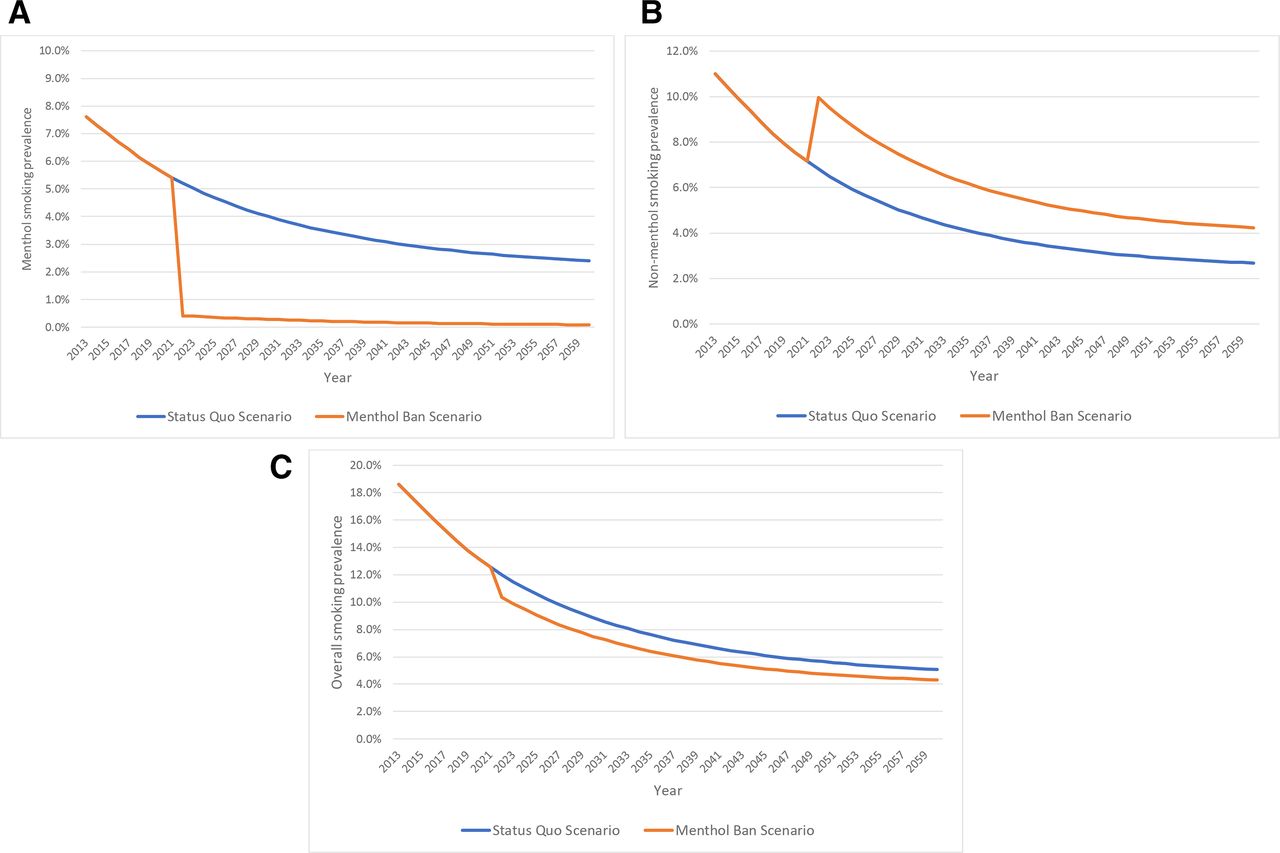
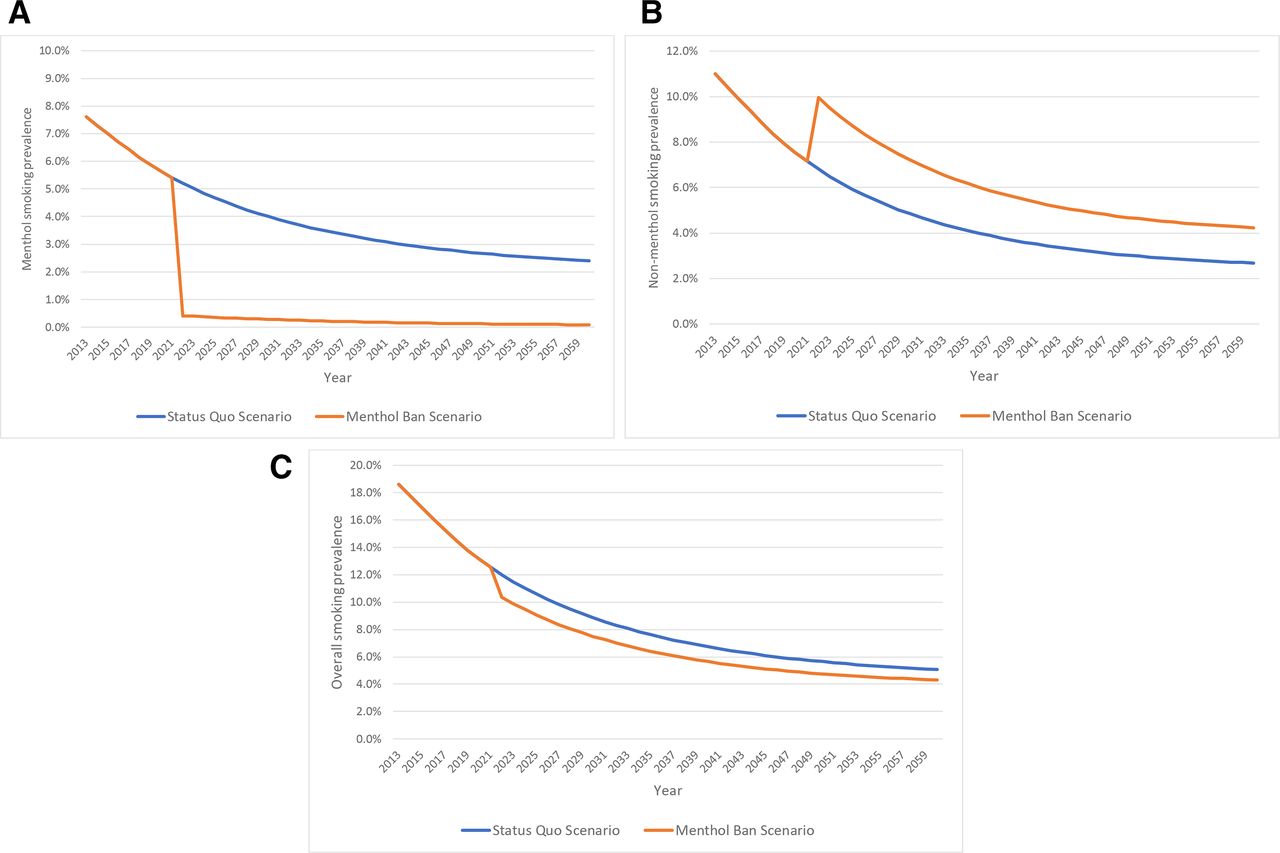
Under the status quo scenario, adult (age >18) menthol smoking prevalence declines from 5.4% in 2021 to 4.5% in 2026 and 2.4% in 2060, while non-menthol smoking prevalence declines from 7.1% in 2021 to 5.7% in 2026 and 2.7% in 2060. Cumulative SVADs from 2021 to 2060 of 14.2 million translate to 143.2 million LYLs.
Under the menthol ban scenario, adult menthol smoking prevalence declines to 0.3% in 2026 and 0.1% in 2060, while non-menthol smoking prevalence increases to 8.4% in 2026 but declines to 4.2% in 2060. Cumulative SVADs of 13.6 million translate to 131.9 million LYLs.
Figure 2A–C shows menthol, non-menthol and overall smoking prevalence from 2013 to 2060 under the status quo scenario and menthol ban scenario. By 2060, combined menthol and non-menthol smoking prevalence falls from 5.1% under the status quo to 4.3% with a menthol ban, a 15.1% relative reduction. Exclusive NVP prevalence increases by 25% under the menthol ban compared with status quo scenario (7.4% vs 5.8%). Cumulative SVADs by 2060 are reduced by 650 000 (4.6% relative reduction), and LYLs are reduced by 11.3 million (7.9% relative reduction).
{kind=link}
{kind=link}
(A) Current menthol smoking prevalence (age 18 and above), menthol SAVM, status quo and menthol ban scenarios, 2013–2060. (B) Current non-menthol smoking prevalence (age 18 and above), menthol SAVM, status quo and menthol ban scenarios, 2013–2060. (C) Current overall smoking prevalence (age 18 and above), menthol SAVM, status quo and menthol ban scenarios, 2013–2060. SAVM, smoking and vaping model.
Sensitivity to NVP relative risks and NVP transition parameters
Table 2 provides sensitivity analyses to variations in model parameters relative to the baseline levels (case 1). With NVP risk at 5% of excess smoking mortality risks and baseline levels of other parameters (case 2), both total averted SVADs and LYLs increase by 5%. With NVP risks at 25% (case 3), averted SVADs and LYLs both decline by 5%.
Sensitivity analysis of averted smoking and vaping-attributable deaths and life-years lost to NVP relative risks and individual transition parameters, both genders combined, all ages, 2021–2060
With a 10% change in the smoking initiation rate (case 4, case 5), averted LYLs vary by 2% in the opposite direction and vary by 6% in the same direction with a 10% change in the overall smoking cessation rate (case 6, case 7). Equating the menthol to non-menthol cessation rate (case 8) reduces the averted LYLs by 24%. With a 10% change in the overall switching rate to NVP use (case 9, case 10), averted LYLs vary by about 3% in the opposite direction. Assuming the same switching rate from menthol smokers as non-menthol smokers (case 11) reduces averted LYLs by 24%. Maintaining the switching rate at the 2018 level rather than assuming a 10% annual decline (case 12) reduces averted LYLs by 22%.
The results were relatively insensitive to NVP initiation (0.1% change) and cessation rates (0.6% change) (cases 13–16).
Discussion
In the absence of a ban on menthol in cigarettes and cigars, the proportion of smokers who smoke menthol cigarettes is likely to continue to increase over time even as overall smoking prevalence declines. With a ban implemented in 2021, we estimated that combined menthol and non-menthol cigarette smoking would decline by 14.7% by 2026 and by 15.1% by 2060 relative to combined smoking in the absence of a ban. With these reductions, SVADs were estimated to fall by about 5% and LYLs by 8.8%, translating to 650 000 deaths averted (16 250 per year) and 11.3 million life-years gained (almost 300 000 per year) over a 40-year period. These impacts are large relative to other tobacco control policies,55 and the public health gains are observed over a wide range of parameter values in the model. Further, while we focus on health gains over a 40-year period, much of the impact is on initiation and related health effects that occur after 40 years. When the analysis is extended to consider a 60-year period, life-years gained increase from 11.3 to 14.7 million (see online supplemental file 3).
Our analysis expands on previous research by incorporating NVP use. A relatively large percentage of menthol smokers, particularly young menthol smokers, switch to NVP use. While increased NVP use presents its own risks, sensitivity analyses indicated that assuming NVP excess mortality risks are 25% those of smokers still yields 620 000 deaths averted and 10.7 million life-years gained under a ban. Increasing the NVP initiation rate and reducing the NVP cessation rate also had minimal effects, despite our assumption that cessation from NVPs is no more likely than from cigarettes. Nevertheless, these risks and the potential for NVPs to be a gateway to smoking, while uncertain, could influence the public health impact of a menthol ban in combustibles. If these prove to be a significant problem, stronger policies may be needed to reduce NVP use among youth. However, while the public health implications were relatively insensitive to changes in the rate of NVP initiation and cessation, they were sensitive to rates of switching from cigarette to NVP use, suggesting that policies to reduce NVP use among youth could also reduce their use by adults, thereby reducing adult smoking cessation.
Our results are conservative in some respects. First, we considered impacts through 2060. Beyond 2060, deaths averted would increase both in absolute and relative terms as the effects on younger generations of reduced smoking are fully realised. We also limited the direct effects of a menthol ban on current menthol smokers to 2 years. Further increases might be expected over time (eg, via additional cessation from illicit menthol or from non-menthol smoking by previous menthol smokers). Our analysis does not consider the effects of a menthol ban on non-menthol smokers. Peer effects of reduced menthol smoking by family, friends, parents or coworkers may motivate more non-menthol smokers to quit.18 While the expert elicitation expected relatively small impacts on non-menthol smokers,19 a 5% reduction in non-menthol use (as suggested by one expert) spread equally between NVPs and no tobacco use would further avert 69 000 deaths (a 9% increase compared with our baseline findings) and 1.1 million LYLs (10% increase) by 2060. Finally, we do not explicitly include current cigar use in this application of the model. Public health benefits are also likely to accrue for current cigar smokers, who may quit all use or switch to NVPs in reaction to a ban.
We did not perform analyses of subpopulations within the USA. Our expert elicitation19 suggested larger impacts on African-Americans. Under a menthol ban, experts estimated 48% of African-Americans who would otherwise initiate menthol smoking would not initiate smoking or vaping compared with 39% for the overall population, and African-American menthol smokers aged 35–54 would be more likely to quit all tobacco use (27% vs 22%). With African-Americans having disproportionately high rates of menthol smoking,3 7 56 a menthol ban would reduce downstream health disparities in smoking-related morbidity and mortality.57 58
Limitations
The results depend on parameters and assumptions underlying the model. While the model was calibrated to incorporate the increase in NVP use through 2018, youth NVP rates increased further in 201959 60 and then fell substantially in 2020,59 indicating that NVP use is difficult to predict. Although some evidence suggests that NVP use may increase smoking initiation,61 62 recent increases in youth vaping coincide with rapid declines in smoking by youth and young adults.63 64 If these reductions in youth and young adult smoking are not maintained, the increased smoking rates among youth and young adults would lead to a larger impact from a menthol ban.
Another limitation is that SAVM does not distinguish dual use of NVPs and cigarettes from exclusive cigarette use. While some studies indicate stable levels of dual use,65 66 other studies indicate dual use is an unstable use state, with high rates of transition to exclusive NVP use or cigarette smoking.27–31 Moreover, some studies suggest similar health risks for dual users as for exclusive smokers,67–69 although others have suggested higher levels.70–72 Further study is warranted on health impacts and patterns of dual use. The model also does not distinguish the health impact experienced by exclusive menthol cigarette smokers who switch to cigar use as a result of a menthol ban. While a recent study found similar levels of biomarker-based risk exposure of exclusive cigar and exclusive cigarette users48 73 and smoking patterns of little cigar users have been found to be similar to those of cigarette users,74 further exploration is warranted on the health impacts of cigar use, especially different types of cigars, for example, little cigars, cigarillos or large cigars. Those switching to smokeless tobacco were also not distinguished. While our expert panel indicated minimal switching to smokeless tobacco, current marketing of oral products, such as ON!,75 may increase the likelihood of switching to these products.
The results are also subject to uncertainties regarding the impact of a menthol ban. The menthol ban transitions were based on results of an expert elicitation.19 While we adopted a well-defined selection process that screened for menthol-related research expertise, the results are dependent on the selected reviewers.19 In addition, because expert elicitations rely on opinions, they are subject to heuristics and biases that are difficult to correct.76–79 The opinions of individual experts differed considerably, especially regarding the extent of switching to exclusive NVP and no use. However, the use of median rather than mean estimates of net transitions (not shown) had little effect on the results. The elicitation results are also consistent with our recent review of menthol ban studies,18 while the magnitude of our findings is broadly consistent with those of a previous menthol ban model17 and a recent study of menthol bans.80
We modelled a ban on menthol applied to both cigarettes and cigars to restrict substitution from cigarettes to little cigars.81–84 We did, however, ask the experts about the impact of a menthol ban on just cigarettes, which the experts indicated would have substantially less impact. We also asked experts about the impact of a menthol ban that is extended to all nicotine delivery products, including NVPs, and they indicated that menthol smokers were less likely to switch out of menthol cigarette use (ie, into NVPs or no regular use) in that scenario compared with a ban limited to cigarettes and cigars. This outcome is consistent with expectations that menthol smokers would be especially likely to switch to menthol NVPs.85 The effects of a menthol ban will also depend on other tobacco control policies. In particular, higher cigarette taxes would reduce smoking initiation and increase cessation,86–90 and increased enforcement of age 21 purchase laws would likely reduce smoking initiation.91 92 While these policies would reinforce the effects of a ban, they may reduce its relative impact, as suggested by our sensitivity analyses regarding reduced smoking initiation and increased smoking cessation.
Finally, the results depend on the modelling approach. Further research might consider expanded categories of nicotine delivery product types (eg, inclusion of smokeless tobacco, distinguishing NVP device type) and multiproduct use, feedback loops via system dynamics models (eg, due to reactions by government or industry to policy changes) and heterogeneity of the population via microsimulation (eg, differential effects by race or socioeconomic status).24 25
Conclusion
Our findings strongly support the implementation of a ban on menthol in cigarettes and cigars on public health grounds. These gains reflect reduced smoking initiation and increased smoking cessation. Support for a menthol ban is strengthened by sensitivity analyses showing that large public health benefits accrue under a broad range of model parameters. Additional public health benefits may be expected through reductions in menthol cigar use.
What this paper adds
The US Food and Drug Administration (FDA) recently announced its intention to ban menthol in combustible products. Previous research has focused on the relationship between menthol cigarette use and initiation and cessation and on the impact of menthol use on overall smoking, but has not considered the potential impact on future cigarette and nicotine vaping product use if a ban of menthol in cigarettes and cigars were to be implemented. Additional evidence is needed by the FDA on its public health impact.
Our model estimates that such a menthol ban on cigarettes and cigars could prevent 650 000 premature tobacco-related deaths and reduce life-years lost by 11 million over a 40-year period. These gains accrue under a broad range of assumptions.
Our findings strongly support implementation of a ban on menthol in cigarettes and cigars on public health grounds.
Data availability statement
Data are available upon reasonable request. The model and data will be provided upon request. The model and data will be provide upon request.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Stephanie Land for her helpful comments.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AlexCLiber, @cdoug
Contributors DTL and RM supervised the project and were the principal writers of the original manuscript and the revised manuscript. ZY conducted the original data analysis and wrote the original methods and results sections. YL conducted the original data analysis and helped write the original methods and results sections. CC led the original expert elicitation and helped write the methods section and revisions. LMS-R and NT helped lead the original expert elicitation and helped write the methods section and revisions. MK conducted the data analysis on the expert elicitation and helped write the methods section and revisions. RMi, JLH, NFL, SS, AFB, ACL and CD helped write the original paper and revisions. JJ helped conduct the analysis, and write the original paper and revisions. KEW was a major contributor to the original paper and revisions.
Funding This project was funded through the National Cancer Institute (NCI) and the Food and Drug Administration (FDA) grant U54CA229974.
Disclaimer The opinions expressed in this article are the authors’ own and do not reflect the views of the National Institutes of Health, the Department of Health and Human Services, or the US government.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.