Article Text

Abstract
Background Understanding disparities in the burden of cancer attributable to smoking is crucial to inform and improve tobacco control measures. In this report, we estimate the population attributable fraction (PAF) of cancers deaths attributable to smoking at the national and provincial levels in China.
Methods Using cancer mortality data from 978 counties, smoking data from a nationwide survey and relative risks from a prospective study of 0.5 million adults in China, we calculated the absolute (non-standardised) and standardised numbers and proportions of cancer deaths among adults 30 years and older attributable to active and second-hand smoking in 2014 across all 31 provinces in Mainland China.
Results The estimated number of cancer deaths attributable to smoking in China in 2014 was 342 854 among men and 40 313 among women, of which second-hand smoking accounted for 1.8% and 50.0%, respectively. Among men, the absolute PAF in China was 23.8%, ranging from 14.6% in Xinjiang to 26.8% in Tianjin; the overall standardised PAF was 22.2%, ranging from 15.7% in Xinjiang to 26.0% in Guizhou. Among women, the overall absolute and standardised PAFs were 4.8% and 4.0%, ranging from 1.8% and 1.6% in Jiangxi to 14.9% and 9.6% in Heilongjiang, respectively. Overall, provinces with the highest standardised PAFs among men were located in Southwest China and among women in the Northeast.
Conclusions Comprehensive smoke-free policies in China should expand to all provinces, notably those with a higher burden of cancer attributable to smoking, instead of being mostly limited to Beijing and some other metropolitan areas.
- smoking caused disease
- disparities
- public policy
- carcinogens
- secondhand smoke
Statistics from Altmetric.com
Introduction
China has the highest number of tobacco users in the world, and accounts for over 40% of the world’s tobacco consumption.1 The prevalence of current smoking in China in 2010 was 54.0% among men and 2.6% among women, accounting for 318 million adults aged 18 years and older (304 million men and 14 million women).2 Tobacco use is estimated to cause one million premature deaths in China each year, which is projected to rise to two million in 2030 and three million in 2050, unless widespread tobacco control policies and programmes are immediately put into effect.3 Of these premature deaths, about 0.4 million were cancer deaths in 2013.4
Cancer is the leading cause of death in China,5 and smoking is the leading modifiable risk factor for cancer.4 Strong national and local tobacco control policies and programmes are critical to reduce this growing cancer burden in China. However, while China has made advances in tobacco control in recent years, progress has remained limited in scope and effect. In 2005, China ratified the WHO Framework Convention on Tobacco Control.6 Since then, at least 18 cities in China have adopted comprehensive smoke-free laws prohibiting smoking in public places and workplaces.7 In particular, the Beijing Smoking Control Ordinance, which came into effect in June 2015, has provided a model for successful tobacco control efforts.8 9 However, most of the other cities still lack comprehensive smoke-free laws, policies and programmes and continue to face challenges with both implementation and enforcement.7 Tobacco control policies also remain particularly weak in provinces with high smoking prevalence, such as the Yunnan province.10 Moreover, progress on substantive national and local tobacco control has been hampered by strong opposition from the state-controlled tobacco industry.6
Despite geographical variations in smoking prevalence,11 differences in the burden of cancer attributable to tobacco use across provinces in China remain unknown. Province-specific smoking-attributable mortality is particularly valuable for public health advocates and local policy makers to take effective action against tobacco use. Herein, we estimate the number and proportion of cancer deaths attributable to active smoking and second-hand smoking in adults older than 30 years in each of the 31 provinces/autonomous regions/municipalities (hereafter, provinces) in Mainland China.
Methods
Provincial cancer deaths
Provincial-level estimates of cancer deaths are based on data from 449 cancer registries and 605 disease surveillance points in 2014, respectively, covering 627 and 608 counties/cities/districts (counties, thereafter) in 31 provinces in Mainland China (online supplementary efigure 1). After the elimination of duplications, a total of 978 counties from 31 provinces were included in the analysis covering 340.7 million adults 30 years and older (accounting for 40.3% of the total population) in China in 2014, with the population coverage ranging from 24.5% in Tibet to 100% in Beijing. We first calculated cancer death rates stratified by sex, cancer site and age group (30–34 years, 35–40 years, …, 80–84 years, ≥85 years) in each province. Then we extrapolated the death rates with sex-specific, age-specific and province-specific populations in 2014 to estimate the number of cancer deaths in each province. Provincial total cancer deaths for men and women were calculated by summing across all age groups and cancer sites. Lastly, we summed across all 31 provinces to obtain the national sex-specific and age-specific cancer deaths and total cancer deaths.
Supplemental material
Smoking exposure data
Age-specific, sex-specific and province-specific smoking prevalence were obtained from the 2002 Chinese National Nutrition and Health Survey (NNHS), which was a stratified multistage cluster sampling design covering 132 sample sites from all 31 provinces (online supplementary efigure 1).12 Active smoking was defined as smoking at least one cigarette every day for 6 months or more during the lifetime (continuously or intermittently); a smoker who had smoked within 30 days before the survey was defined as current smoker, otherwise they were defined as a former smokers. Data were also obtained on the age at initiation of smoking and the intensity of smoking (cigarette equivalents per day) for smokers and on status of second-hand smoke for non-smokers. Second-hand smoking was defined as reporting exposure to environmental tobacco smoke for at least 15 min on 1 day per week.
Attributable burden estimation
We estimated the province-specific population attributable fractions (PAFs) for smoking-related cancer deaths using relative risks (RRs) among men from the China Kadoorie Biobank Study (online supplementary etable 1), which was a nationally representative prospective cohort with 512 891 Chinese participants from 10 geographically defined regions and 7 years follow-up.13 Consistent with the RR estimates, the cancer sites included in this analysis were cancers of the lung, liver, oesophagus, stomach, mouth, pharynx, larynx, pancreas, urinary bladder and all other cancers (including those without an established causal association with smoking). We combined the results for five cancer sites (mouth, pharynx, larynx, pancreas and urinary bladder; thereafter ‘minor sites’) and all other cancers due to small numbers in multiple provinces. Lung cancer is the only cancer associated with second-hand smoking in this analysis.14 15 We assumed 12 years lagged smoking prevalence in estimating the smoking-attributable burden for cancer death.16 In our analyses, we considered the difference in time period between cancer deaths and smoking exposure surveys. For example, for calculating PAFs for the age group 30–34 years in 2014, we used smoking prevalence for age 18–22 years from the 2002 NNHS.
The age and cancer site-specific PAFs were calculated based on estimates of exposure, RRs and the theoretical minimum risk exposure level for active smoking (zero for smoking) using the standard formula for multicategory exposure:17

where  ,
,  ,
,  ,
,  ,
,  represent the proportion of never, former and current light (<15 cigarettes per day), moderate (15–24 cigarettes per day), heavy (≥25 cigarettes per day) smokers; and
represent the proportion of never, former and current light (<15 cigarettes per day), moderate (15–24 cigarettes per day), heavy (≥25 cigarettes per day) smokers; and  ,
,  ,
,  ,
,  , the RR for the former and current light, moderate, heavy smokers, respectively, compared with never smokers. For calculating the burden of second-hand smoking, we first estimated the number of lung cancer deaths in non-smokers using:
, the RR for the former and current light, moderate, heavy smokers, respectively, compared with never smokers. For calculating the burden of second-hand smoking, we first estimated the number of lung cancer deaths in non-smokers using:

in which  and
and  referred to the total number of lung cancer deaths and prevalence of active smoking, respectively.4 Then, we used the following formula to estimate PAFs for second-hand smoking for each strata of sex and age group:
referred to the total number of lung cancer deaths and prevalence of active smoking, respectively.4 Then, we used the following formula to estimate PAFs for second-hand smoking for each strata of sex and age group:

where  is prevalence of second-hand smoking in the adult at the category i, and
is prevalence of second-hand smoking in the adult at the category i, and  is the RR for the association between second-hand smoking and cancer death.
is the RR for the association between second-hand smoking and cancer death.
The 95% CIs for the PAFs were estimated using a bootstrap simulation method with 5000 replications. Following PAF calculations, the number of cancer deaths attributable to smoking and the corresponding 95% CIs in each age group and sex group for each evaluated cancer site in 31 provinces were calculated by multiplying the age-specific, sex-specific, site-specific and province-specific PAFs by the corresponding estimated cancer deaths in 2014. The total number of attributable deaths and 95% CIs for each cancer site and province were then calculated by summing across all age groups. Finally, the overall PAFs and the corresponding 95% CIs for each cancer site and province were calculated by dividing the number of attributable deaths by the total number of cancer deaths among adults 30 years and older in each province.
Standardisation and sensitivity analysis
It is well known that there exist considerable geographical disparities in cancer mortality in China; for example, lung cancer is more common in North-East China than South-West China (online supplementary efigure 2). However, it should be noted that the calculation of PAFs without considering the age structure of provincial populations could potentially introduce bias when we compare age-aggregated PAFs across provinces. For example, all site-specific PAFs in Tianjin were lower than Guizhou in this analysis, whereas the overall PAF (for all cancers combined) was higher in Tianjin (online supplementary etable 2). Thus, we conducted a standardisation process to obtain age-standardised and cancer site-standardised PAFs. The age-specific and site-specific proportions for standardisation were based on total national cancer deaths (online supplementary etable 3).
Smoking in this analysis was defined by both status (never, former or current) and intensity of smoking for current smokers combined. To assess the effect of using other definitions for smoking, we repeated analyses by defining smoking using smoking status only (never, former or current), current smoking intensity and age at initiation of smoking.
Results
In 2014, an estimated 383 167 cancer deaths in adults 30 years or older in China were attributable to smoking (both active and second-hand smoking), with 342 854 of these deaths occurring in men (23.8% of all cancer deaths, 95% CI 23.3% to 24.3%) and 40 313 in women (4.8%, 95% CI 4.5% to 5.2%) (table 1). Of these deaths, about 6180 lung cancer deaths among men (5.9% of lung cancer deaths among non-smokers; 1.4% of all lung cancer deaths) and 20 170 among women (11.5% of lung cancer deaths among non-smokers; 10.2% of all lung cancer deaths) were attributable to second-hand smoking (online supplementary etable 4).
Provincial-level smoking prevalence and cancer deaths attributable to smoking in adults 30 years and older, 2014
Among men, the absolute (non-standardised) proportion of cancer deaths attributable to smoking ranged from 14.6% in Xinjiang to 26.8% in Tianjin and Shandong; and was over 26.0% in five provinces (Tianjin, Shandong, Chongqing, Heilongjiang and Hunan) and less than 20.0% in five other provinces (Xinjiang, Tibet, Guangxi, Ningxia and Shanghai). Among women, the absolute proportion ranged from 1.8% in Jiangxi to 14.9% in Heilongjiang. In five provinces (Heilongjiang, Tianjin, Jilin, Inner Mongolia and Liaoning) the PAF was >10.3%, but is 6.1% or less in all other provinces (table 1).
The age-standardised and cancer site-standardised PAF among men is 19.0% or higher in all provinces except Xinjiang (15.7%), being highest in Guizhou (26.0%) (figure 1 and online supplementary etable 4). Among women, the standardised PAF ranged from 1.6% in Jiangxi to 9.6% in Heilongjiang. Overall, provinces with the highest PAFs differed by sex. Among men, they are mostly located in the South-West, whereas among women, they are in the North-East (figure 1). Tibet, Ningxia and Xinjiang are among 6 provinces with the lowest standardised PAFs for men but among the 10 highest for women.

Rank of age-standardised and cancer site-standardised proportion of cancer deaths attributable to smoking in each province of Mainland China, 2014. The proportion was standardised for each cancer site and age group, with active and second-hand smoking both included.
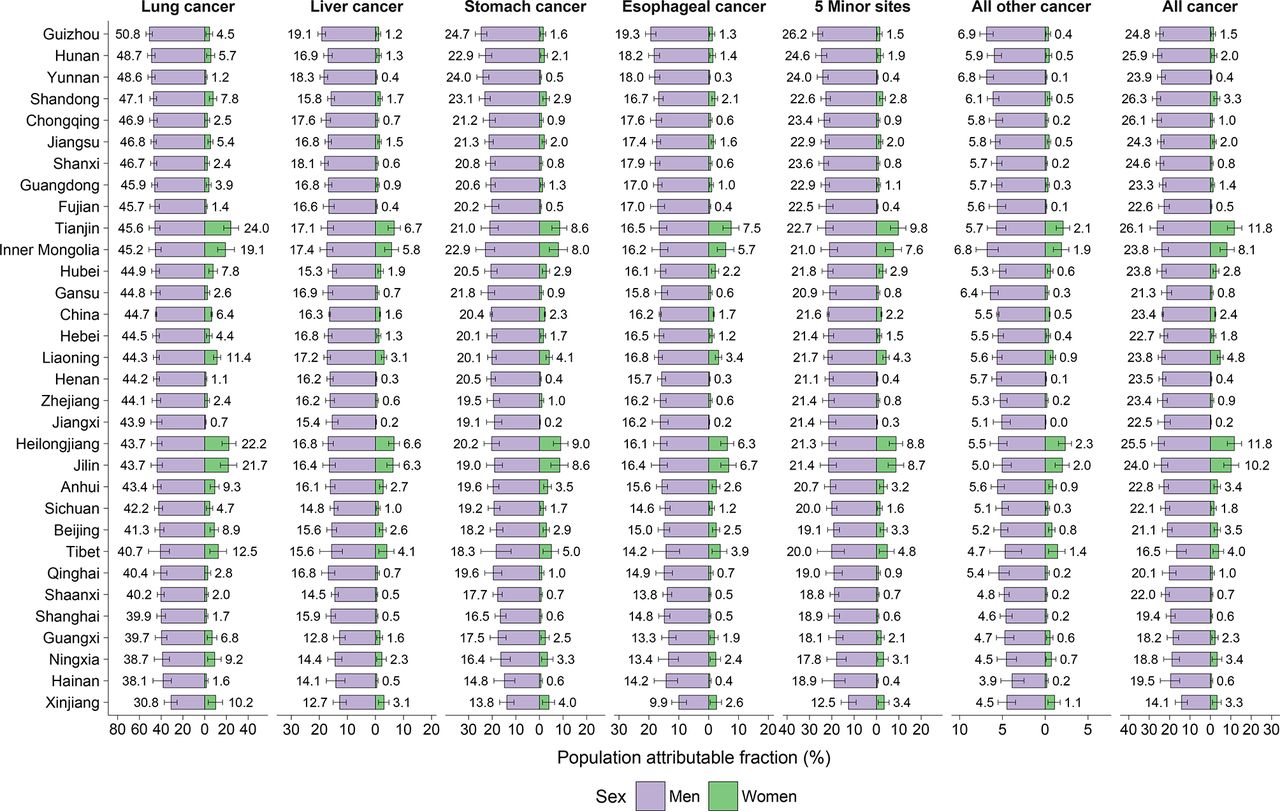
The pattern of absolute PAFs (figure 2) and age-standardised PAFs (online supplementary etable 4) by cancer site for active smoking is generally comparable across provinces. Guizhou is the province with highest absolute and standardised PAFs for all evaluated cancer sites among men. Tianjin, Heilongjiang, Jilin, Inner Mongolia and Tibet rank as the top five among women.

Provincial-level absolute proportion of deaths attributable to active smoking for site-specific cancer in Mainland China, 2014. Five minor sites include: mouth, pharynx, bladder, larynx and pancreas.
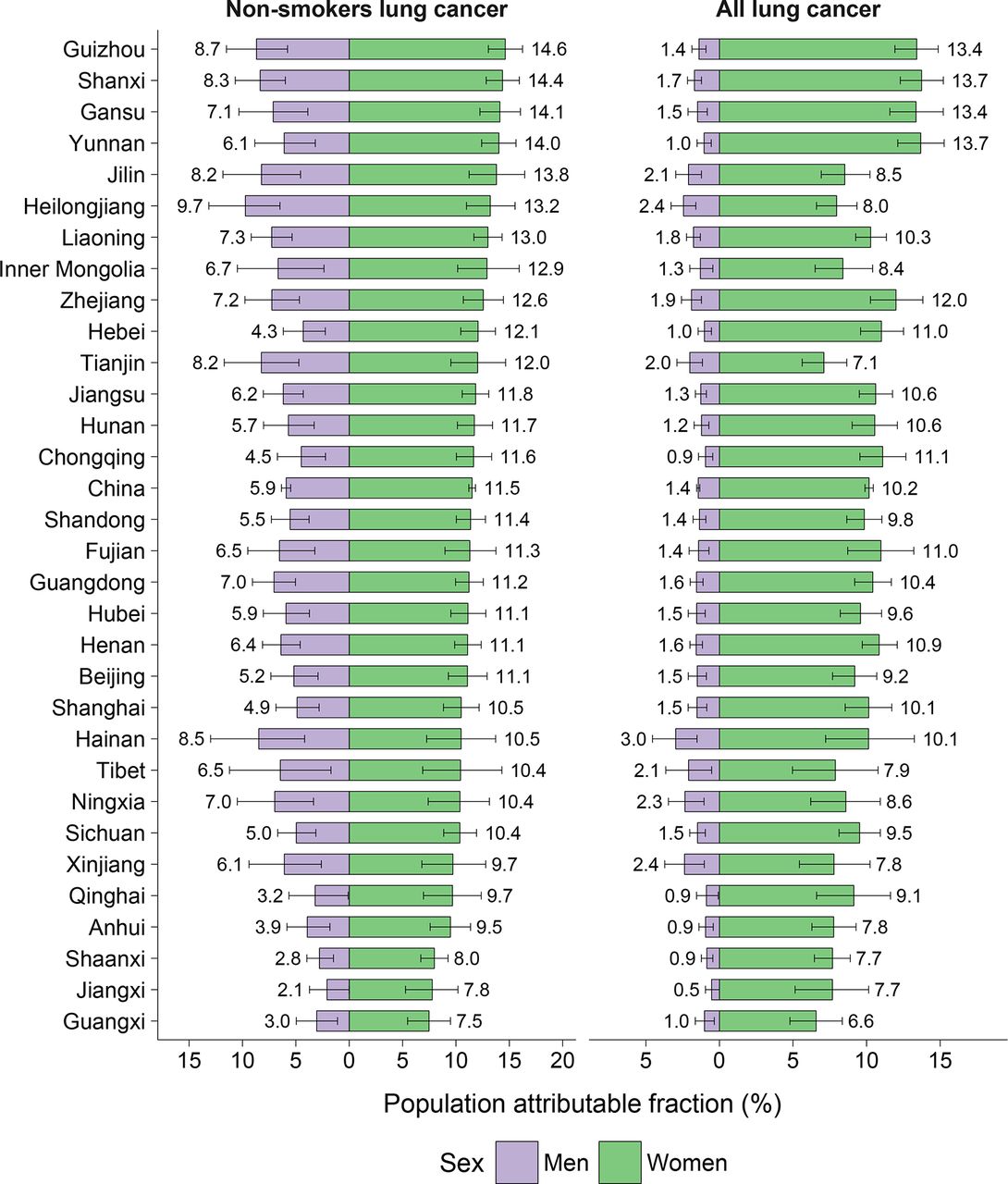
The proportion of lung cancer attributable to second-hand smoking is higher in women than in men across all 31 provinces (figure 3). Among men, the PAF is the highest in Heilongjiang, Guizhou, Hainan, Shanxi, Tianjin and Jilin and lowest in Jiangxi. Among women, Guizhou, Shanxi, Gansu, Yunnan and Jilin have a higher PAF, and Guangxi has the smallest. The rankings of provinces in terms of absolute and standardised PAFs for lung cancer attributable to second-hand smoking are very similar (online supplementary etable 4).
{kind=link}
{kind=link}
{kind=link}
Provincial-level absolute proportion of lung cancer deaths attributable to second-hand smoking in Mainland China, 2014. The proportion were reported using the non-smokers lung cancer deaths and all lung cancer deaths as references, respectively.
By age group, the PAFs are higher in men aged 55–59 years and women aged 80–84 years for all active smoking-related cancers, while the peak age of PAFs is about 25 years younger for second-hand smoking, that is, 30–34 years for men and 55–59 years for women (online supplementary efigure 3). Using alternative definitions for smoking did not substantially change the results (online supplementary etable 5).
Discussion
In 2014, about 0.4 million cancer deaths (16.8% of all cancer deaths) in adults 30 years and older in China were attributable to active and second-hand smoking. More than 98% of these deaths in men were attributable to active smoking, compared with 50% in women. PAFs were higher in South-West China for men and North-East China for women, consistent with patterns in smoking prevalence. Interestingly, while the PAF for smoking was lowest for men in Xinjiang, Ningxia and Tibet, these three minority autonomous regions were among the provinces with highest PAF for women.
Disparities in PAFs by sex and province appear to be primarily driven by differences in smoking prevalence in corresponding provinces, age groups and sex. Smoking prevalence among Chinese men started to substantially increase in the second half of the 20th century and peaked in the 1990s (61.4%).18 Despite some declines, however, male smoking prevalence is still high (52.9% in 2010).6 However, smoking is much less accepted for women in China and smoking prevalence among women remains relatively low, especially in more traditional, rural areas in South China.19 Smoking among women is higher in North-East China and in urban areas like Beijing and Tianjin, where female smoking is more socially acceptable.20 21 By birth cohort, in the China Kadoorie Biobank Study, smoking prevalence peaked in men born in the 1950s–1960s, while among women, smoking prevalence gradually decreased from the oldest age group (born in the early 1930s) to the youngest age group in that study (born in the late 1960s).3 13 There was a similar pattern in the NNHS data used in this study. Correspondingly, PAFs for active smoking in this study were higher in men aged 55–59 years (born during 1955–1959) and women aged 80–84 years (born during 1930–1934). Cigarettes are still regarded as a common gift and a form of social currency in China, especially in rural areas where awareness of the health effects of tobacco use is lower than in urban areas.22 As in most other countries, smoking prevalence in China is associated with lower socioeconomic and educational levels.23 24 In some metropolitan areas, such as Beijing and Shanghai, smoking ban in public areas was implemented and public support for tobacco control has grown substantially.25 However, in other provinces, notably those where tobacco is grown, such as Yunnan, Hunan and Guizhou, tobacco use is considerably higher.26 27 Thus, attitudes and cultural acceptability of smoking, socioeconomic status and education level, and public sector support for tobacco control policies and programmes, appear to be key determinants of patterns of smoking prevalence, and the resulting cancer burden, among the 31 provinces in Mainland China.
Despite high smoking prevalence, the current proportion of cancer deaths attributable to smoking is lower in China compared with some other countries. For example, while the PAF for lung cancer mortality associated with active smoking in men was around 45% in this study, it is around 90% in USA, the UK, France, Japan and Korea.28 Methodological differences, such as using the smoking impact ratio to calculate the burden of cancer associated with smoking, may have contributed to this variation. However, differences in stages of the cigarette epidemic and competing risks in China versus other countries may be greater contributors to this variation in PAFs.29 In comparison with Western populations where the epidemic is more advanced, the observed RR for lung cancer and several other cancers are quite modest in China (eg, 2.5 in China and about 25 in USA for lung cancer).13 30 However, probably due to an earlier age of initiation, the RRs associated with smoking along with the associated PAFs have increased over the past two decades.3 It is likely that the magnitude of this association will substantially increase in China over time as the full impact of tobacco smoking emerges, a pattern also observed in several Western countries.30 Lung cancer incidence is relatively high among non-smokers in China as compared with other countries, likely as a result of exposure of competing risks factors such as second-hand smoking, ambient air pollution and other sources of indoor air pollution.31 32 Generally, estimates from our study were consistent with previous estimates from China for smoking-related PAFs for all cancers4 13 and site-specific cancers.33 34 However, slightly higher overall PAF estimates for active smoking in 2005 reported by an earlier study (32.7% in men and 5.0% in women)35 could, in part, be explained by higher RRs used in that study. For example, the RR for ever-smoking and lung cancer in that study was 5.7 for men and 5.0 for women, based on a case-control study in Shanghai,35 whereas it was about 2.5 for current smoking in our study, based on a large-scale prospective study.13
Our study is the first analysis that systematically assesses sex-specific, age-specific and site-specific cancer burden attributable to smoking in 31 provinces across Mainland China. However, our study has some limitations. First, we used RRs for specific cancer sites based on reported associations among men due to high uncertainty in reported RRs among women in the China Kadoorie Biobank Study.13 However, the reported RRs for the association between smoking and all cancers were similar in men (1.44) and women (1.42). Further, we took into account smoking intensity to reduce potential bias due to lower smoking intensity among women in China. Second, the RRs for lung cancer death reported by the China Kadoorie Biobank Study were slightly higher than that for incident lung cancer,3 13 but we used RRs for cancer incidence in our study as they were based on higher numbers of cancers. Third, we aggregated all other cancers into one group due to small numbers, and this group included some cancer sites with less than sufficient evidence for a causal association with smoking, which may overestimate the total number of attributable deaths in this study. However, the latter aggregated group constituted only 5.1% of all attributable cancers among men and 4.6% among women, thereby limiting possible overall impact on our findings.
We found that a considerable proportion of cancer deaths in all provinces in China, notably among men, are attributable to tobacco use. However, there are also substantial differences in this proportion across provinces. As the tobacco epidemic remains at an earlier stage in China than that compared with North America and Europe, the full impact of tobacco smoking patterns in recent decades on cancer mortality may have not have been realised yet. Thus, if no tobacco control action is taken to immediately reduce tobacco use with quality implementation of targeted policies and programmes, the burden for cancer and other smoking-related diseases will continue to grow dramatically. As illustrated by the experience of Beijing’s strictest smoking ban, policies and programmes in Beijing appear to be having an impact on reducing smoking behaviour,9 36 this experience could serve as a model for other regions in China, including rural areas and tobacco-growing provinces. Further, the MPOWER tobacco control initiatives recommended by the WHO Framework Convention on Tobacco Control include monitoring tobacco use, protecting people from tobacco smoke, offering help to quit tobacco use, warning about the dangers of tobacco, enforcing bans on tobacco advertising and promotion, and raising taxes on tobacco products. These efforts need high-level support and should be required and promoted at the national and provincial levels, including joint efforts from the local governments, multiple levels of the Chinese Centre for Disease Control and Health Inspection Bureaus, as well as greater support for non-government organisations, private enterprises and civil society organisations to promote strong tobacco control policies and programmes, and help China stem the quickly rising tide of preventable cancer deaths attributable to tobacco use.
What this paper adds
While previous studies estimated the smoking-attributable cancer burden in China nationally, no similar estimates exist at the provincial level. This study provides the first estimated smoking-attributable cancer burden across all 31 provinces in Mainland China.
Previous studies are built on limited data and relative risk (RR) estimates, resulting in less precise estimates due to the small sample sizes. However, this study takes advantage of population-based data and RR estimates from China, allowing us to estimate cancer deaths attributable to both active and second-hand smoking simultaneously.
This study identifies substantial variations on smoking-attributable cancer burden across Chinese provinces among both men (ranging from 15% to 27%) and women (2% to 15%). Local government and non-government organisations should tailor their tobacco control policies and programmes to meet these higher-risk groups accordingly.
References
Footnotes
Contributors WC conceived and designed the study. CX led the data analysis, wrote the first draft and drafted the final manuscript. RZ, MZ and LW did the cancer data abstraction, collecting, cleaning, checking and coding. MZ and SZ oversaw data collection and quality control. HZ, XZ and KS contributed to manuscript amendments and abstraction of smoking data. FI and MP contributed to the development of analysis plans, reviewed the results and contributed to the preparation of the final manuscript. ZY and HL checked the analysis process and reviewed results. All authors contributed to the interpretation of data and approved the final manuscript.
Funding This study was supported by the Ministry of Science and Technology of China (grant number 2014FY121100).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.