Article Text

Abstract
Objective This study aimed to quantify the long-term impact of implementing the WHO Framework Convention on Tobacco Control (FCTC) compliant tobacco control measures, MPOWER, on smoking prevalence and mortality in men and women aged ≥20 years in Japan.
Design A Stock-and-Flow simulation model was used to project smoking prevalence and mortality from 2018 to 2050 under eight different scenarios: (1) maintaining the 2018 status quo, (2) implementation of smoke-free policies, (3) tobacco use cessation programmes, (4–5) health warning about the dangers of tobacco (labels, mass media), (6) enforcement of tobacco advertising bans or (7) tobacco taxation at the highest recommended level and (8) all these interventions combined.
Results Under the status quo, the smoking prevalence in Japan will decrease from 29.6% to 15.5% in men and 8.3% to 4.7% in women by 2050. Full implementation of MPOWER will accelerate this trend, dropping the prevalence to 10.6% in men and 3.2% in women, and save nearly a quarter million deaths by 2050. This reduction implies that Japan will only attain the current national target of 12% overall smoking prevalence in 2033, 8 years earlier than it would with the status quo (in 2041), a significant delay from the national government’s 2022 deadline.
Conclusions To bring forward the elimination of tobacco smoking and substantially reduce smoking-related deaths, the government of Japan should fulfil its commitment to the FCTC and adopt stringent tobacco control measures delineated by MPOWER and beyond.
- Public policy
- Prevention
- Smoking Caused Disease
Data availability statement
Data are available in a public, open access repository.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Japan’s tobacco control has been insufficient despite its ratification of the WHO Framework Convention of Tobacco Control (FCTC), and the prevalence of smoking remains high particularly among men. While quantitative measures of the potential impact of implementing FCTC-compliant tobacco control policies are useful for guiding policy change, such information for Japan is currently scarce.
What this study adds
This study suggests that full implementation of tobacco control measures as recommended by MPOWER will accelerate the reduction of smoking prevalence and save nearly a quarter of a million deaths by 2050 in Japan; however, even with full implementation, delay is expected in attaining Japan’s current national target of 12% overall smoking prevalence.
How this study might affect research, practice or policy
The government should adopt stringent measures recommended by MPOWER and beyond to bring forward the elimination of tobacco smoking and substantially reduce smoking-related deaths.
Background
Tobacco use is the largest preventable cause of premature death and disability globally. A global public health treaty aimed to address the tobacco smoking epidemic, the WHO Framework Convention on Tobacco Control (FCTC) entered into force in 20051 and has been ratified by 182 countries.2 Since the treaty became effective, an increasing number of countries have implemented evidence-based tobacco control measures conforming to the WHO FCTC (MPOWER): Monitoring tobacco use and prevention policies (M); Protecting people from tobacco smoke (P); Offering help to quit tobacco use (O); Warning about the dangers of tobacco (health warning labels (W-L) and mass media (W-MM)); Enforcing bans on tobacco advertising, promotion and sponsorship (E) and Raising taxes on tobacco (R).3 Countries that successfully implemented some of these measures at the highest recommended level experienced substantial reduction of tobacco smoking and tobacco-attributable deaths.4 5
Japan ratified the WHO FCTC in June 2004. However, implementation has been fragmented and tobacco control remains suboptimal relative to the FCTC standard, with Japan receiving poor (no or minimal policy) ratings in the P, W and E domains in 2018.3 The 2020 Tokyo Olympic and Paralympic Games created social pressure and political will, and the tobacco control movement has been somewhat enhanced through the adoption of additional policies such as raising tobacco taxes and implementing stricter smoke-free regulations. However, despite these new measures connected to the Games and this renewed social and political focus on denormalisation of tobacco smoking, progress on tobacco control policy in Japan has been slow compared with other countries.3
Japan’s slow tobacco control progress is reflected in the high smoking prevalence among men at 27% in 2019,6 which was higher than other high-income countries. Tobacco smoking has been the top risk factor for non-communicable disease (NCD) mortality in Japanese adults,7 contributing to an estimated 19.1%–24.6% of total deaths in men and 3.6%–6% in women.8 9 The WHO Global Action Plan for the Prevention and Control of NCDs 2013–2020 established a global target of 30% relative reduction in smoking prevalence by 2025, using 2010 as baseline.10 Domestically, Japan has a target to achieve 12% smoking prevalence by 2022.11 However, it is doubtful if Japan can meet either of the targets with its presently suboptimal tobacco control measures.
To catalyse a dialogue about the need for more comprehensive tobacco control measures in Japan, this study aims to estimate:
smoking prevalence over the next three decades under the status quo scenario and seven enhanced MPOWER implementation scenarios;
when the international and national targets of smoking prevalence will be met in each scenario and
the number of lives saved by enhanced MPOWER implementation.
Methods
Data sources and preparation
Age-specific and sex-specific populations in Japan were projected from 2010 to 2050 using published values for all-cause total mortality rate estimates, birth rates and infant sex ratios from the Japanese Vital statistics12 and National Institute of Population and Social Security Research.13 Age-specific and sex-specific smoking prevalence was obtained from the National Health and Nutrition Survey (2010–2018).6 Mortality rates by smoking status were apportioned and projected forward using estimates of the relative risks of all-cause death derived from a pooled analysis of nine nationally representative Japanese cohort studies; the relative risks for current and former smokers used in this study were 1.60 and 1.24 for men, and 1.48 and 1.24 for women, respectively.14 Further details of data sources (online supplemental table 1) and preparation methods are described in online supplemental file sections 1 and 2.
Supplemental material
Simulation scenarios
Stock-and-Flow System Dynamics models15 were used to project the number of smokers, smoking prevalence and mortality from current, former and never smokers from 2018 (baseline) to 2050 for men and women aged 20 years or older under the status quo and seven intervention scenarios. The status-quo scenario was based on the status of tobacco control in Japan in 2018 (table 1).3 A total of six intervention scenarios were hypothesised on implementing each intervention at the highest recommended level. The P, O, W-L, W-MM, E and R measures were selected for the present analysis because they have yet to be implemented at the highest level in Japan.3 The last intervention scenario is hypothesised on implementing all MPOWER measures at the highest level simultaneously.
Intervention scenarios and the respective effect sizes
Simulation models
The simulation was run in each age- (20–29, 30–39, …, 70+ years) and sex-specific group. The model started with the number of current and former smokers at the baseline year 2018. The number of smokers was obtained by multiplying the 2018 population by the 2018 smoking prevalence. Then, cessation rates and former and current smokers’ all-cause mortality rates were applied to determine the number of smokers who became former smokers and the number of deaths by smoking status. The present study defines the cessation rate as the net value after considering smoking cessation and initiation. To obtain the cessation rate for the status quo model, current smoker prevalence data was used to fit a linear regression model on the log of prevalence (online supplemental figure S1). The estimated annual trend in each age group was used as the age-specific cessation rate (online supplemental table S2) and applied throughout all years in the status quo model (2018–2050) and for 2 years in the intervention model (2018–2019).

Diagram of the Stock-and-Flow simulation model. A diagram illustrating the simulation model used to assess the impact of MPOWER tobacco control measures on smoking prevalence and mortality.
The cessation rates for all intervention scenarios were converted from intervention-specific effect sizes adapted from Levy et al,16 defined as the long-run (40-year horizon) relative reduction in smoking prevalence of full implementation relative to zero/minimal implementation. The effect sizes used in our study reflect the magnitude of the effect expected from implementation of the highest recommended policy level relative to Japan’s MPOWER policy level in 2018, converted to annual cessation rates (table 1) (see online supplemental file 2.5 - 2.7). The effect size was assumed to be equal across all age groups and sexes, except for the R measure, which was larger among younger age groups who are more cigarette price-sensitive than their older counterparts.17 18 The derived cessation rates (online supplemental table S2) were applied as constant from 2020 onwards in each intervention scenario.
Having calculated changes in the distribution of current, former and never smokers due to cessation and mortality, the population matured by 1 year, and 10% of the remaining population in each 10-year age group was shifted to the next age group. We considered smoking prevalence for those aged 20 years and above and assumed that the new cohort of 20 year-olds entered the population with a smoking prevalence that matches the current profile of 20–29 year-olds. At the end of each full year-cycle, the numbers of current, former and never smokers were converted to prevalence, and the respective number of deaths was totalled (figure 1). Equations for all simulation steps are provided in online supplemental file section 2.
National and international smoking prevalence targets
The Ministry of Health, Labour and Welfare established a national target of 12% overall prevalence of smoking by 2022.11 19 The WHO Global Action Plan for the Prevention and Control of NCDs 2013–2020 established a global target of 30% relative reduction in smoking prevalence by 2025 using 2010 as baseline,10 which means reduction of smoking prevalence from 32.2% to 22.6% in men and 8.4% to 5.9% in women in Japan.
Averted deaths
The number of averted deaths was calculated as the difference between the number of deaths in the status quo and intervention scenarios, including deaths from current, former and never smokers. A positive value for averted deaths indicates fewer deaths in the intervention scenario than the status quo scenario.
Sensitivity analyses
We performed two sensitivity analyses. Sensitivity analysis 1 assumed that intervention policies’ effects start to wane after 10 years. The cessation rates from 2018 to 2030 were applied as constant, and from 2030 onwards, the cessation rates were set to reduce by 3% annually. In sensitivity analysis 2, long-term effects were realised in 10 or 20 years instead of 40 years.
Results
Smoking prevalence under the status quo scenario and MPOWER policy scenarios
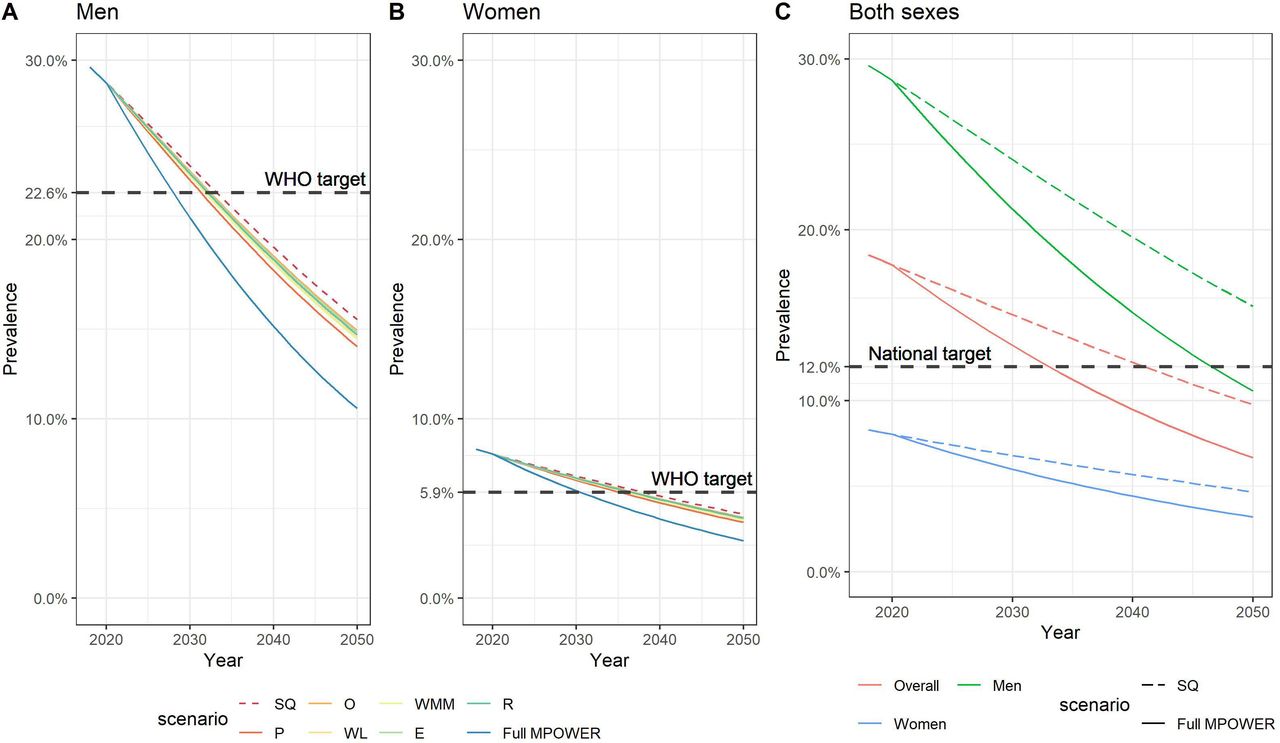
Under the status quo scenario, the smoking prevalence is projected to steadily fall from 29.6% to 15.5% for men and from 8.3% to 4.7% for women between 2018 and 2050 (figure 2, online supplemental figure S2). In both sexes, a greater downward trend in prevalence of current smokers was observed in younger age groups than in older age groups. A slight increase in smoking prevalence before a steady downward trend was observed in older age groups, most prominently in the 70+ age group and in women. In the individual policy scenarios, smoking prevalence reduced to 14.0%–14.9% in men and 4.2%–4.5% in women by 2050 (figure 3); smoke-free policies enforced at the highest level (P) achieved the biggest prevalence drop, followed by W-MM, W-L, E, R and O. The reduction in smoking prevalence is greater and faster when all MPOWER measures were implemented simultaneously at the highest level, reducing the smoking prevalence to 10.6% in men and 3.2% in women by 2050 (figure 3).
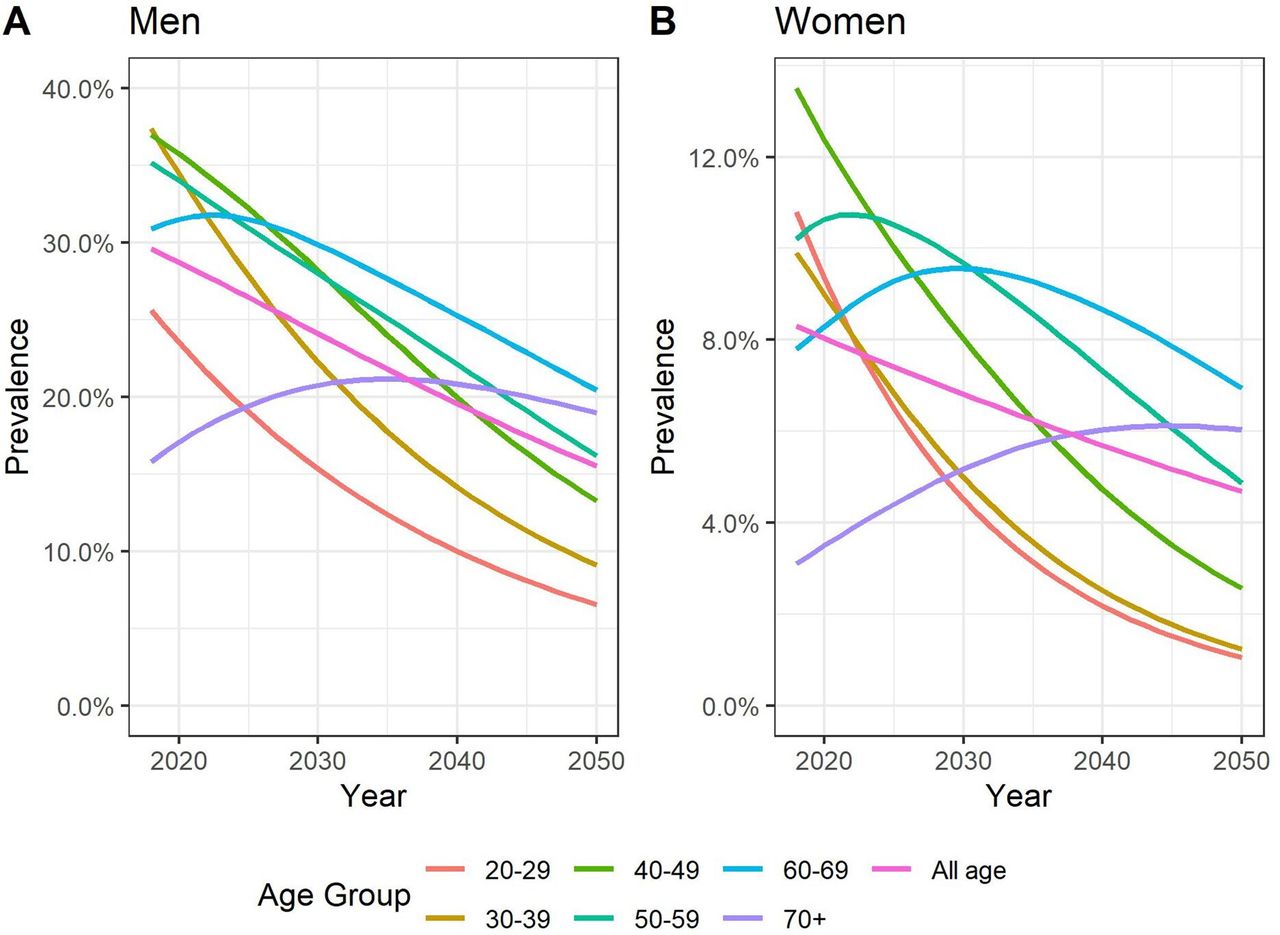
Projected sex-specific and age-specific prevalence of current smokers from 2018 to 2050 under the status quo scenario. Each plotted line indicates the projected age-specific prevalence (%) of current smokers in (A) men and (B) women from 2018 to 2050.

{kind=link}
{kind=link}
{kind=link}
Projected smoking prevalence by MPOWER tobacco control policy scenario and (A, B) international and (C) national targets of smoking prevalence. WHO target is as stipulated in the WHO Global Action Plan for the Prevention and Control of Non-Communicable Disease 2013–2020, that is, to work towards 30% reduction in smoking prevalence by 2025, relative to the prevalence in 2010. In Japan, the smoking prevalence in 2010 was 32.2% in men and 8.4% in women. Therefore, the WHO target is defined here as 22.6% in men and 5.9% in women by 2025. National target is to achieve an overall smoking prevalence (combined both sexes) by 12% by 2022, as stipulated in National Health Promotional Movement in the 21st Century (Healthy Japan 21, the second term). E, Enforce bans on tobacco advertising, promotion and sponsorship; Full MPOWER, Simultaneous implementation of all MPOWER tobacco control measures at the highest recommended level; O, Offer help to quit tobacco use; P, Protect people from tobacco smoke; R, Raise taxes on tobacco; SQ, Status quo; WL, Warn about the dangers of tobacco (Labelling); WMM, Warn about the dangers of tobacco (Mass Media).
Expected time to attain the targets of smoking prevalence
Under the status quo, Japan will achieve the international target of 30% relative reduction in smoking prevalence in men by 2034 and in women by 2038, and the 12% national target of overall smoking prevalence by 2041 (figure 3, online supplemental table S3). With full MPOWER implementation, Japan will achieve the male and female international smoking prevalence targets by 2028 and 2031 respectively, and the national overall smoking prevalence target by 2033. Although MPOWER interventions will shorten the time to meet targets, Japan still falls short of the stipulated timeframe (international: 2025, national: 2022). In the analysis where cessation rates were set to reduce by 3% annually from 2030 (Sensitivity analysis 1), expected time to attain the targets remained the same. In Sensitivity analysis 2, where the long-term effects are assumed to be realised in 10 or 20 years, the international target would be achieved in time only in the 10-year horizon model, and the national target would be achieved 7 or 3 years earlier than the main model, respectively (online supplemental figure S3, online supplemental table S3).
Number of deaths averted from each MPOWER policy scenario
Table 2 shows the cumulative number of deaths averted from each intervention scenario at years 2030 and 2050. By 2050, scaling up P can prevent 71 332 deaths (59 001 men and 12 331 women), and scaling up O can prevent 27 982 deaths (23 143 men and 4840 women). If all MPOWER measures were to be implemented at the highest level simultaneously, a total of 237 299 deaths (196 455 men and 40 844 women) would be averted by 2050, which is three to eight times more deaths averted than any individual MPOWER policy. In the sensitivity analyses, the corresponding numbers were 223 265 deaths (Sensitivity analysis 1), 694 585 deaths (Sensitivity analysis 2: 10 year horizon) and 425 087 deaths (Sensitivity analysis 2: 20 year horizon) (online supplemental table S4).
Estimated number of sex-specific cumulative averted deaths from each intervention scenarios
Discussions
This study projected tobacco smoking prevalence and mortality in the Japanese population up to 2050 under status quo and hypothetical tobacco control scenarios. It showed that strengthening tobacco control in all MPOWER domains to the highest level can accelerate the decline in smoking prevalence in Japan, reducing prevalence to 10.6% in men and 3.2% in women by 2050, and avert a total of nearly a quarter million deaths over the next three decades. Japan will not be able to achieve international and national targets in time, but with MPOWER interventions at the highest recommended level, Japan will meet these targets 6–8 years sooner than with current tobacco control measures.
Of the six individual interventions, comprehensive smoke-free legislation (P) would have the greatest impact on smoking prevalence. As of 2018, P was rated as minimal.3 In anticipation of the Tokyo 2020 Olympic and Paralympic Games, the 2020 revision of the Health Promotion Act introduced smoking bans for all eateries with penalties for facilities that violate the rule. However, this policy exempts nearly half of all eateries with seating areas not more than 100 m2,20 21 far from the FCTC Article 8 requirement of a complete smoking ban in all public places,22 leaving some risk of secondhand smoke exposure for customers and workers. Therefore, any exemption should be removed.23
Improving W-L and W-MM from the minimal level to the complete level can reduce smoking prevalence. Japanese cigarette packaging warnings are inconspicuous,24 in contrast with countries like Australia. Although labelling surface area has improved from 30% to 50% in 2020, the impact is likely small compared with graphic warnings.19 The WHO Report on the Global Tobacco Epidemic 202125 upgraded Japan’s W-MM rating from minimal to highest level despite limited changes in practice. A nationwide antitobacco campaign is needed to denormalise smoking habits, curb smoking initiation and promote cessation.19
Our study found only a small effect of tobacco taxation on reducing smoking prevalence, compared with other MPOWER measures. Japan has already achieved a moderate level of implementation with 63.1% tobacco taxation in 2018,3 but the price of the most commonly sold brand of cigarettes in international dollars as of 2018 was low at $4.45/pack in Japan, in contrast to countries like Sri Lanka ($22.17), Singapore ($16.87), New Zealand ($16.08) and Ireland ($14.95).26 Although the sales price for a pack of 20 cigarettes increased by approximately 50 JPY in 2020, this price remains highly affordable,27 especially for older age groups, and a 75% tax component is unlikely to deter smokers from tobacco use. Tobacco taxation beyond 75% and other tax and price-based measures should be considered.
Enforcement of bans on tobacco advertising, promotion and sponsorship (E) is also effective in reducing smoking prevalence, but Japan currently lacks such bans, and more than 40% of smokers and 66% of non-smokers continue to be exposed to cigarette advertising.28 Furthermore, coverage of smoking cessation services (O) is suboptimal, with comprehensive cost-coverage only available for heavy smokers29 and no national quitline. Many smokers resort to unassisted smoking cessation methods30 which are unreliable.31 Given that 26% of smokers (25% of men and 31% of women) in Japan expressed quit intentions,6 cost-covered cessation services should be expanded to all smokers.
We found that implementation of comprehensive MPOWER measures is far more effective than a fragmented approach in reducing smoking prevalence, but still insufficient to attain national or international smoking prevalence reduction targets in time. Our model showed a relatively small number of averted deaths (1% of male deaths and 0.2% of female deaths), largely due to greater prevalence of former smokers (online supplemental figure S2) for whom the risk of mortality stays elevated for years, though to a lesser degree than for current smokers. Another reason could be the assumption of constant cessation under the status quo, which could have overestimated the reduction of smoking prevalence in this scenario. The conservative assumptions in our analysis likely yielded conservative estimates of the policy effects, yet even in the most optimistic scenario where intervention effects were realised in 10 years, the national target will not be achieved. These results point to the urgent need to shift all smokers to former smokers and deter non-smokers from initiating smoking by implementing full MPOWER measures and enhanced measures beyond MPOWER.
Although public health gains from an enhancement of tobacco control measures are evident, Japan faces many challenges to tobacco control implementation due to industry interference in policymaking; the pre-eminent political challenge is the Japanese government’s 33% financial stake in Japan Tobacco.32 Japan was rated the poorest in the Global Tobacco Industry Interference Index which measures efforts by governments to address tobacco industry interference.33 Countries that shield against industry interference have succeeded in implementing strong tobacco control.34 35 Enhanced action to bring forward the elimination of tobacco smoking in Japan will be easier to achieve if the government enacts strict regulations on tobacco industry’s interference on health policies and conforms to WHO FCTC Article 5.3.1
To our knowledge, this is the first study to assess the potential impact of MPOWER tobacco control measures on smoking prevalence and mortality in Japan. Our results can facilitate public and political dialogue on strengthening the nation’s tobacco control policies by illustrating the public health gains achievable from more comprehensive interventions. The strengths of our study include assessing, separately and in combination, the effects of various tobacco control policies as benchmarked against MPOWER strategies and calibrated to Japan’s status quo policies. This analysis enables a comparison of benefits between policies and managed expectation on time needed to attain tobacco control targets. Another strength is that the datasets used in this study were sourced from government-funded, nationally representative cross-sectional surveys and large-scale cohort studies conducted among the Japanese population.14
Nevertheless, our results have some limitations. First, it did not take into account the potential impact of the growing popularity of heated tobacco products (HTPs).36–38 HTP use in Japan increased especially among male smokers of younger ages, and smokers use HTPs with or without intention to quit smoking.37 While use of HTPs can influence individual patterns of smoking,39 40 the effect of HTP use on smoking cessation or prevalence remains inconclusive.41 Continued efforts to better understand the impact of HTP use on smoking patterns and subsequent mortality risk should be encouraged and resulting evidence should be incorporated into future simulation studies. Second, our projection model did not incorporate variations in mortality risk according to time since smoking cessation, which may have underestimated the number of averted deaths in former smokers. Third, we did not simulate the impacts of MPOWER on never smokers. With about 15 000 deaths per year in Japan attributable to secondhand smoke exposure,42 some averted deaths from never smokers can be expected with stricter smoke-free policies. Last, our projection did not include people aged under 20 years because the rapidly declining smoking rate among minors43 could underestimate the smoking initiation rate of early adulthood.
Conclusion
Full implementation of MPOWER tobacco control measures can accelerate the reduction of tobacco smoking prevalence and is expected to save nearly a quarter of a million deaths by 2050. However, even with full implementation, Japan is unable to attain the national and international targets in time. To end the tobacco epidemic and its associated preventable mortality, an acceleration of progress with tobacco control is needed, for which the government should realise their commitment to greater public health and begin the final steps to eliminate tobacco use, the largest preventable risk factor for global premature death and disability, from Japanese society.
Data availability statement
Data are available in a public, open access repository.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
SLY and KT are joint first authors.
SLY and KT contributed equally.
Contributors SLY and KT are co-first authors and contributed equally to the article. SG and SLY had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Conception and design: SG, KK, KT, SLY. Development of methodology: SG, KK, SLY. Acquisition of data and analysis: SLY. Interpretation: SG, KK, MEL, IS, KT, SLY. Initial writing of the manuscript: KT, SLY. Review and revision of the manuscript: SG, KK, MEL, IS, KT, SLY. Supervision: SG, KK. Guarantor: KK.
Funding The study was supported by the Japan Society for the Promotion of Science (JSPS) KAKENHI (Grants-in-Aid for Scientific Research) (B), Grant number: 17H03589, and the Ministry of Health, Labour and Welfare, Health and Labour Sciences Research Grants, Comprehensive Research on Life-Style Related Disease including Cardiovascular Diseases and Diabetes Mellitus and Cancer Control Policy, Grant number: 19-FA1-005 and 20EA1017. KT reported having been supported by European Commission FP7 Marie Curie Actions—People—Co funding of regional, national and international programmes (COFUND) during the initial phase of this work.
Disclaimer Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/World Health Organization.
Competing interests KK reported having received a JMWH Bayer Grant (1 million JPY) from 1 September 2017 to 31 August 2019 via the Japan Society for Menopause and Women’s Health. No other disclosures were reported.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.