Article Text

Abstract
Objective To investigate the tobacco-attributable burden on disease, medical costs, productivity losses and informal caregiving; and to estimate the health and economic gains that can be achieved if the main tobacco control measures (raising taxes on tobacco, plain packaging, advertising bans and smoke-free environments) are fully implemented in eight countries that encompass 80% of the Latin American population.
Design Markov probabilistic microsimulation economic model of the natural history, costs and quality of life associated with the main tobacco-related diseases. Model inputs and data on labour productivity, informal caregivers’ burden and interventions’ effectiveness were obtained through literature review, surveys, civil registrations, vital statistics and hospital databases. Epidemiological and economic data from January to October 2020 were used to populate the model.
Findings In these eight countries, smoking is responsible each year for 351 000 deaths, 2.25 million disease events, 12.2 million healthy years of life lost, US$22.8 billion in direct medical costs, US$16.2 billion in lost productivity and US$10.8 billion in caregiver costs. These economic losses represent 1.4% of countries’ aggregated gross domestic products. The full implementation and enforcement of the four strategies: taxes, plain packaging, advertising bans and smoke-free environments would avert 271 000, 78 000, 71 000 and 39 000 deaths, respectively, in the next 10 years, and result in US$63.8, US$12.3, US$11.4 and US$5.7 billions in economic gains, respectively, on top of the benefits being achieved today by the current level of implementation of these measures.
Conclusions Smoking represents a substantial burden in Latin America. The full implementation of tobacco control measures could successfully avert deaths and disability, reduce healthcare spending and caregiver and productivity losses, likely resulting in large net economic benefits.
- Public policy
- Low/Middle income country
- Advertising and Promotion
- Taxation
- Packaging and Labelling
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Smoking continues to be a leading cause of disease and death, impacts the economy of individuals and their families, and is responsible for costs and productivity losses, representing a burden for countries and contributing to poverty.
In 2007, WHO introduced the MPOWER package of cost-effective best practices measures, including tobacco tax increases; smoke-free environments; health warnings on tobacco product packaging; and enforcement of bans on tobacco advertising, promotion and sponsorship.
Despite the proven effectiveness of these measures, their implementation and enforcement are suboptimal in Latin America.
WHAT THIS STUDY ADDS
Our study shows that smoking is responsible for a substantial burden in terms of disease, direct medical cost, productivity losses and time devoted to providing unpaid care to family members.
The economic losses attributable to tobacco represent 1.4% of the combined gross domestic product of Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Mexico and Peru (countries accounting for 80% of the Latin American population); current tobacco taxes cover only 15.1% of these economic losses.
Countries are missing out on major health and economic benefits by not properly implementing key tobacco control measures.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We provide clear evidence about the benefits of full implementation of tobacco control strategies that could guide government decisions to invest in tobacco control best practices.
Latin America needs to strengthen its existing measures of tobacco control aiming at their full implementation: (1) substantial increases in tobacco taxes to reach international standards; (2) complete implementation and enforcement of smoke-free environments; (3) plain packaging; and (4) complete bans on tobacco advertising, promotion and sponsorship.
Introduction
In 2019, tobacco use was responsible for the loss of 200 million disability-adjusted life-years (DALYs) globally.1 The negative impact of tobacco use goes beyond health, causing more than $1 trillion in healthcare expenditures and lost productivity each year as a result of tobacco-related diseases.2 In health and economic terms, most of the burden falls on small and medium-developing countries, where 80% of the world’s 1.1 billion people who actively smoke live.3 In addition to direct medical costs, tobacco also affects the economy through the productivity losses caused by tobacco-attributable diseases, and the informal unpaid care of these diseases, a burden that disproportionately affects women. In Latin America, smoking is among the five leading risk factors for death and disability, contributes to poverty due to decreased productivity and out-of-pocket expenses and accounts also for $34 billion in direct medical costs annually.2 4 5
Although the evidence on the harmful effects of tobacco is indisputable, over the past two decades, the progress made on tobacco control has been insufficient; smoking remains a leading risk factor for early death and disability.6 Although most countries in the region have signed the Framework Convention for Tobacco Control (FCTC), the enforcement of key control interventions is delayed because of misinformation, prejudice, lack of quality data and pressure from the industry.4 7 8 To promote the implementation of tobacco control policies in the region, it is necessary to monitor the health and economic consequences of smoking at the country level and to make this information available to decision-makers. High-quality data may raise awareness of the health, social and economic harms of tobacco use, the harmful effects of delayed implementation of control measures, and the benefits of proper implementation and enforcement. If effective actions are not taken, the tobacco epidemic will certainly grow in Latin America, a region suffering from the double burden of communicable and chronic diseases, and where the COVID-19 epidemic has exacerbated the shortage of health resources.
The aims of this study are twofold: (1) to estimate the tobacco-related burden on disease, mortality, direct medical costs, productivity losses and caregiver burden; and (2) to estimate the health and financial effects of the four main tobacco control interventions recommended by the FCTC in Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Mexico and Peru, constituting 80% of the population of Latin America.
Methods
Study design
This study is based on an economic model developed as part of a collaborative project between academic institutions, researchers and decision-makers from 12 Latin American countries (of which eight were selected for this project based on their population size and/or availability of required data).4 9 The model is a state transition or Markov probabilistic microsimulation of individuals (first-order Monte Carlo technique) that considers the natural history, direct medical costs, indirect costs such as productivity loss, and quality-of-life losses associated with the main tobacco-attributable diseases (coronary and non-coronary heart disease, cerebrovascular disease, chronic obstructive pulmonary disease (COPD), pneumonia, influenza, lung cancer, mouth and pharynx cancer, oesophageal cancer, stomach cancer, pancreatic cancer, kidney cancer, larynx cancer, acute myeloid leukaemia, bladder cancer and cervical cancer). Its characteristics, components, validation and applications are described in previous publications.4 7 8 10 11 In this model, individuals are followed up in hypothetical cohorts, from 35 years of age to death, and annual individual risks of disease incidence, disease progression and death are estimated based on individuals’ demographic attributes, smoking status, previous clinical conditions and underlying risk equations.
Information sources
Data to populate the model were obtained from a literature review that used MEDLINE, LILACS, Embase, EconLit, Google (for grey literature) and Google Scholar. Public statistics and country representative surveys were the main sources of information on demographics, mortality rates and smoking prevalence. Research teams from participating countries provided additional information from local sources on civil registrations, vital statistics and hospital databases, and validated the epidemiological parameters used. A detailed description of information sources of information is available in the online supplemental material.
Supplemental material
The direct medical costs associated with tobacco-related diseases were updated by the cumulative inflation rate estimates made by our group or, when not available, following a microcosting approach in which resources needed for diagnosis, treatment and follow-up were weighted by usage rates. For cancer events other than lung cancer, indirect estimates were made through the relative cost gap compared with lung cancer, validated by an expert consensus process. We report direct medical costs from the healthcare system perspective. We used a weighted average of the costs of the different health sectors in each country.
The costs of labour productivity loss attributable to tobacco consumption were estimated considering the premature death of working-age individuals, and the decrease in individuals’ labour productivity due to a health condition (absenteeism). To estimate the cost component associated with premature death, we applied the Value of a Statistical Life formula.12 For the absenteeism cost component, we adopted an indirect estimation criterion, assuming that individuals’ work productivity decreased proportionally to the reduction of quality of life attributed to that condition.13 To estimate both cost components, we calculated individuals’ labour income (by age and sex) through a Mincer equation14 using representative household surveys in each country, and the legal retirement age by sex in each country.15 For further details, see Pinto et al.11
We used the proxy good method to estimate the monetary value of the use of time in informal care (informal carers are defined as those who provide care to family members without receiving remuneration or economic compensation for it).16 First, a comprehensive literature review was performed to collect data on time of informal care (in hours per day) for the selected diseases. Currently, regional statistics on this topic are not available. We validated the collected data with a survey among professional caregivers and experts. Then, we used an indirect estimate using information of health state preference values (or utilities) through the interpolation of the validated data for those cases with no reliable information.17 Finally, national household survey databases were processed to obtain the average wage per hour of a proxy of informal caregiver. We introduced the economic burden of informal care in the main outcomes, multiplying the annual cost of hours of the informal caregiver for each of the diseases and the number of cases attributable to tobacco consumption.
All costs were estimated in local currency and converted to US dollars using 2020 average exchange rates, published by central banks. Macroeconomic parameters, such as gross domestic product (GDP) and health expenditure, were extracted from data banks of multilateral organisations.
The epidemiological and economic data to populate the model were obtained from 1 January 2020 to 1 October 2020. The main parameters and their sources are shown in the online supplemental file 1.
Model calibration and validation process
In each country, calibration was done by comparing the specific mortality rates predicted by the model in each sex and age group with the vital statistics (for the base year 2020). Variations of less than 10% were considered acceptable. In the case of larger variations, the risk equations were modified until estimates fell within the desired range (modifying up to a maximum of ±20% of the estimated incidence and/or lethality rates of each condition). The model was externally validated against other epidemiological and clinical studies not used for equation estimation and development.
Estimation of the smoking-attributable disease burden
The main outcomes of the model were disease events, hospitalisation, disease incidence, life-years, quality-adjusted life-years, disease costs, indirect costs and healthy years of life lost (both years lost by premature mortality and quality-of-life losses). The disease burden was estimated as the difference in outcomes between the results predicted by the model for each country under current smoking prevalence and a hypothetical cohort of individuals who never smoked, for each country. Passive smoking and perinatal effects were estimated to impose an additional burden of 13.6% (men) and 12% (women).18
Estimation of the effect of control measures
To estimate the impact of control measures, we followed the approach reported in our previous studies.4 7 10 11 The effect of price increases through taxes on the smoking prevalence was calculated as follows:

where PrevB is the baseline prevalence of smoking before price increase; ∆P is the percent price variation; Ip is the proportion of variation in cigarette consumption expected to impact on smoking prevalence; and Ed is price elasticity of demand for cigarettes. For impact of tax increase on revenues, see online supplemental material. The retail price increase (∆P) modelled for each country was defined based on the affordability of cigarettes according to WHO19: 60% increase for countries in which the cost of 100 packs <3% of GDP per capita (Argentina, Brazil and Colombia), 40% when it was 3%–6% (Chile, Costa Rica, Mexico and Peru) and 20% when it was >6% of the GDP per capita (Ecuador).
Although the association between tax increase and illicit trade is controversial,20 the model considers the potential substitution between legal and illegal markets, based on the cross-price elasticity between them. Parameters needed to estimate cigarette price elasticity for each country were obtained from the literature. In the absence of country-specific estimates, we used information of cigarette consumption in the illicit market before and after a tobacco tax reform in Colombia21 to estimate a proxy of cross-price elasticity of the demand between the licit and illicit tobacco products.
To estimate the impact of implementing plain tobacco packaging, advertising bans or smoke-free air, the smoking prevalence post-intervention was calculated as follows:
Prevalencepost=Prevalancepre−[(Em−Ec)/(1−Ec)×Ip×Prevalencepre]
where Prevalencepre is prevalence of people who smoke before the intervention, Ip is variation proportion in consumption affecting this prevalence, Em is the expected effectiveness of fully implementing the intervention, and Ec is the effectiveness being achieved (if any) with current measures (expressed as relative reduction in tobacco consumption). The effectiveness achieved by these measures for smoke-free air and advertising bans was adjusted according to compliance level in each country.19 The estimated effectiveness of the smoke-free interventions included risk reduction in persons who do not smoke due to reduced exposure to secondhand smoke.8 The impact on health and economic outcomes was estimated as the difference in outcomes between the results predicted by the model for each country under current smoking consumption and under the new scenario of reduced consumption after the implementation of the intervention. The interventions’ impact is reported as the 10-year cumulative effect.
For sensitivity analysis, we used the 95% CI of the elasticity estimate in each country for increasing taxes, and the effectiveness estimate range for the other interventions. Base case results and uncertainty intervals are presented for all results. See online supplemental material for details of the interventions’ expected effectiveness (base case values and ranges), current situation in each country and methods used to estimate the cumulative effect.
Role of the funding source
Sponsors had no role in the study design, data collection, analysis, and interpretation, or writing of the report. The corresponding author had full access to all data and was responsible for the decision to submit for publication. We also confirm that all researchers are independent from funders. All authors had full access to all data in the study and take responsibility for the data and the accuracy of the data analysis.
Transparency statement
The lead author of this study, Professor Dr Andrés Pichón-Riviere, affirms this manuscript is an honest, accurate and transparent account of the study being reported; no important aspects of the study have been omitted and any discrepancies from the study as originally planned have been explained.
Data sharing statement
Data collected for the study are available upon request to corresponding author, after approval of a proposal, with a signed data access agreement.
Patient and public involvement
Decision-makers from 12 countries in Latin America were involved in the design, data collection and dissemination of this study.
Results
Health, economic and social burden of tobacco
In 2020, 351 000 deaths were attributable to smoking in the eight countries included in this study, representing 12.4% of all deaths in adults aged ≥35 years. Smoking is estimated to cause 2.2 million disease events annually, including 143 000 strokes, 130 000 cancers and 756 000 cardiovascular events (table 1). In total, 12.2 million healthy years of life are lost every year because of both tobacco-attributable premature mortality (73.3%) and disability (26.7%), with COPD, cardiovascular disease and cancer as the leading causes (figure 1A). Argentina, Brazil and Chile are the three countries in which smoking is responsible for the most significant burden of disease, exceeding 2500 years of life lost per 100 000 population (3200, 2800 and 3300 years, respectively).
Annual burden of mortality, disease incidence and years of life lost (YLL) attributable to tobacco, by cause and country for 2020
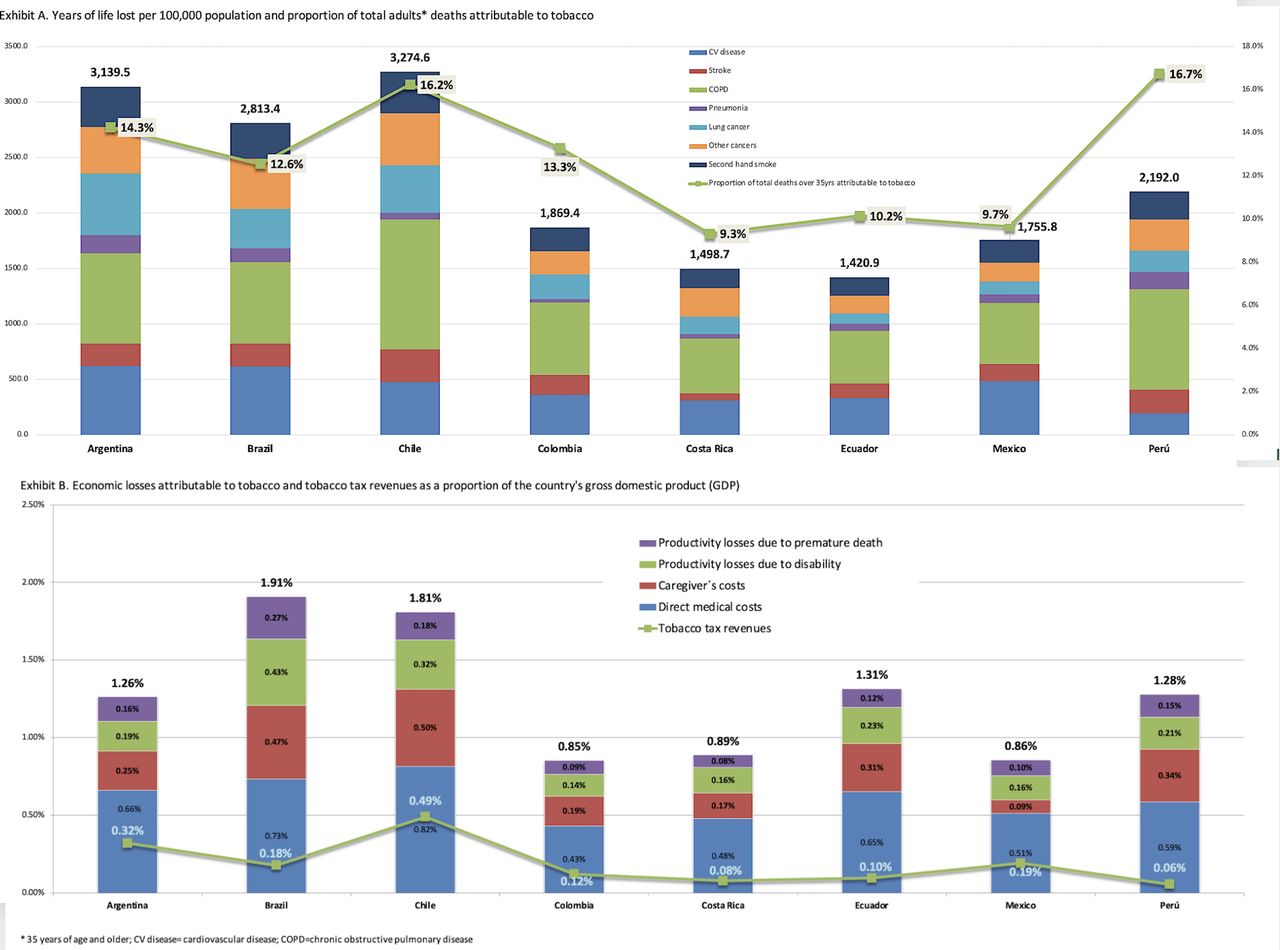
Annual health and economic burden attributable to tobacco (US$2020). (A) Years of life lost per 100 000 population and proportion of total adults’* deaths attributable to tobacco. (B) Economic losses attributable to tobacco and tobacco tax revenues as a proportion of the country's gross domestic product. *Thirty-five years of age and older. COPD, chronic obstructive pulmonary disease; CV, cardiovascular.
In 2020, the healthcare systems of these eight countries spent US$22.8 billion in direct medical costs to treat the conditions caused by tobacco consumption (table 2 and figure 1B). This represented an average of 8.1% of all national health expenditures, ranging from 6.0% in Colombia to 11.7% in Peru.
Annual economic burden attributable to tobacco, by cause and country for 2020 (US$ millions)
The economic burden for lost productivity attributable to tobacco amounted to $16.2 billion because of premature death ($6.4 billion) and disability ($9.8 billion). Caregiver costs represented an additional burden of $10.8 billion. In total, the economic losses attributable to tobacco in 2020 were $49.8 billion, representing an average of 1.4% of the GDP of each of these countries, from 0.9% in Colombia, Costa Rica and Mexico to 1.9% in Brazil. All countries were far from recovering tobacco-attributable economic losses through tobacco tax collection. Tax revenues from cigarette sales are lower than the direct medical costs generated by tobacco consumption in all countries and account for 15.1% of the negative impact of smoking on their economies (ranging from 4.4% in Peru to 29.2% in Chile).
Effects of tobacco control measures
The four tobacco control interventions analysed could substantially reduce the tobacco burden on health and on countries’ economies (table 3). If countries achieved the retail price rise modelled in this study, the expected number of smoking-attributable deaths in the next 10 years would decrease by 271 000, representing a decrease in overall adult deaths (≥35 years) ranging from 4.0% in Argentina to 10.0% in Brazil (figure 2). The raised cigarette taxes would prevent 1.6 million cardiovascular, cancer and other disease events over the next 10 years; additionally, 10.6 million healthy life-years would be gained. Overall, the proposed tax increases in these countries will result in a total economic benefit of $63.8 billion. An important proportion of this benefit results from increased tax revenues ($20.5 billion). Although price rise will result in reduced tobacco consumption, tobacco tax revenues will increase in all countries. Healthcare costs averted because of reduced tobacco consumption ($16.7 billion), and productivity and caregiver costs averted ($17.2 billion and $9.4 billion, respectively) are the other components of the economic benefits expected over the next 10 years if the proposed tax increases are implemented. In a hypothetical scenario with incremented illicit trade as a result of tax measures, the benefits of raised cigarette taxes would decrease but remain large: 183 000 deaths averted and $49.3 billion in economic benefits over the next 10 years (a 32% and 23% reduction, respectively, compared with the base case).
Projected 10-year accumulated health and economic effect of the four main public policy measures for tobacco control

{kind=link}
{kind=link}
Main benefits of the four public policy measures for tobacco control: proportion of tobacco-attributable adults’* deaths that could be averted and economic gains (as a proportion of countries' gross domestic product). *Thirty-five years of age and older.
Implementing plain packaging in the eight countries could prevent 78 000 deaths and 450 000 disease events and would result in economic benefits of $12.3 billion over the next 10 years. Plain packaging would be the second most effective intervention in Brazil and Colombia, after tax increases, and the third most effective measure in Argentina, Chile, Costa Rica, Ecuador and Peru (table 3 and figure 2).
Latin American countries have included in their legislation advertising and sponsorship bans. In addition to the benefits that restrictions in force are already producing, advancing to a complete ban on advertising could reduce adults’ deaths by between 0.4% (Colombia) and 3.9% (Peru), representing 71 000 deaths averted over the next 10 years in the eight countries, and more than $11.4 billion in economic benefits. In Argentina, Chile, Costa Rica and Peru, the full adoption of advertising bans is the most beneficial intervention after the tax increase measure.
Similar to advertising bans, if these countries advanced to the highest level of adoption and enforcement of smoke-free air measures, an additional 39 000 deaths and 217 000 disease events would be avoided, with economic benefits of $5.7 billion over the next 10 years. In Mexico, the adoption of smoke-free air is the second intervention with the greatest potential for health and economic benefits after the tax increase.
Discussion
Our results show that, despite decades of tobacco control efforts, smoking remains a leading cause of health and economic burden in Latin America. Nearly a thousand people die every day as a result of tobacco use in these eight countries, and, in 2020, it was estimated to cause over 2 million disease events, including cardiovascular events, cancer, stroke, COPD and other diseases. These results are consistent with the estimations of the Global Burden of Disease Project,22 which show that, regardless of the relative decrease in tobacco prevalence in the last decades (19.8% (16.9%–22.5%) decrease),23 age-standardised rates of deaths and DALYs for smoking-attributable diseases remain high in Latin America, a region hard hit by the epidemic.
Most studies of tobacco burden focus on the disease component,5 or, if these include the economic dimension, they centre on direct medical costs.4 24 This represents an important underestimation of the burden of tobacco use, as several studies have shown that direct medical costs accounted for less than 50% of the total economic burden. When indirect costs are included, the total economic cost of smoking may reach 1.8% of the world’s annual GDP.25 A significant contribution of our study is the estimation of the economic burden due to lost productivity and caregiver costs, representing over 56% of the total economic burden. Considering direct and indirect costs, we show that tobacco use produces economic losses of $49.8 billion in the eight countries, the equivalent to 1.4% of their combined GDPs.25 Studies in the USA,26 Canada27 and Australia28 have also demonstrated that labour productivity losses account for a considerable proportion of the total economic costs attributable to smoking. In Latin America, a study in Brazil found that labour productivity costs attributable to tobacco consumption represented R$17.5 million, over 30% of Brazil’s total economic burden of smoking.11 Although no studies on the economic burden of informal caregivers associated with tobacco were found, a systematic review showed that the inclusion of informal care in economic evaluations can have a strong impact on cost-effectiveness outcomes under certain circumstances.29 Moreover, informal care is an activity with scarce recognition and strongly feminised, a key element of gender inequalities worldwide.30
Despite the significant burden produced by smoking, tobacco products are still too affordable in the region.31 The price increase through taxes has shown the greatest potential to reduce the tobacco burden and produce the most important economic benefits. As seen in the literature, taxation increase is a very effective measure to reduce cigarette use.32 Even in the most pessimistic scenario, where illicit trade increases because of higher taxes, our results show that health and economic benefits would still be significant and surpass all potential losses produced by illicit trade.
Importantly, this analysis considers the benefits currently being achieved in each country, which allows estimating the true additional benefit expected if these measures are taken to their maximum implementation level. For these reasons, in Argentina, Colombia, Costa Rica, Ecuador and Peru, the smoke-free air measure yields fewer additional benefits because their current legislation and implementation have already advanced significantly.19 Moreover, in Brazil and Chile, with the most comprehensive legislation and the highest adoption levels of this measure,19 no additional benefit could be expected. The opposite occurs in Mexico, lagging behind in terms of smoke-free measures, where our results show this intervention’s substantial potential to reduce the tobacco-attributable burden. A recent reform of the Mexican tobacco control law,33 which enforces smoke-free environments and bans tobacco advertising, will take advantage of the significant benefits of these two interventions.
After the tax increases measure, plain packaging can provide the greatest benefits considering the eight countries together (78 000 deaths and $12.3 billion in costs averted), followed by advertising bans (71 000 deaths and $11.4 billion in costs avoided). Similar to smoke-free air measures, the potential benefits of these interventions are related to the current adoption level. Colombia, with medium-sized warnings in cigarette packages, can expect greater benefits moving towards plain packaging; while Mexico and Peru, which, until now, had the lowest level of restriction on advertising, would obtain the greatest relative benefits with the full implementation of a complete ban.
As in all model-based studies, an important limitation is the quality of the inputs; although we used the best available information and applied a uniform and replicable method, availability and quality of epidemiological and cost information in Latin America are heterogeneous. The 10-year benefit estimates depend on the fact that several factors remain unchanged (eg, smoking behaviours or medical cost), which will not necessarily be the case. There is no conclusive evidence on the true impact of interventions, on how this evidence could be transferred to other settings, or on how to estimate the effects of interventions applied concurrently; therefore, it would be incorrect to simply add up the benefits of the interventions analysed here. The model was calibrated and validated for each country, and we included an estimate of the uncertainty regarding the size of the effect of the interventions, but the model does not account for other potentially relevant sources of uncertainty (eg, epidemiological or cost parameters). Although our study did not include all Latin American countries, the countries analysed comprise 80% of the population, and represent a varied sample. Despite these limitations, this is the most comprehensive assessment of tobacco burden and the potential benefits of control interventions in Latin America, using the most up-to-date and locally generated information at the country level and a robust economic model developed in the region. This enormous tobacco-attributable burden is probably a conservative estimate as other dimensions impacted by tobacco were not included.34
Although taxation, plain packaging, advertising bans and smoke-free laws are the central interventions recommended by the WHO and the best strategy to curb the tobacco epidemic, no country in Latin America has fully adopted these four measures. Taxation falls short of WHO recommendations, cigarettes remain affordable, legislation is lacking to advance with the main control measures, and the implementation and compliance levels are suboptimal. Our results show that tobacco imposes a disproportionate burden on population well-being and countries’ economies that could be avoided with appropriate policies. The four tobacco control interventions analysed could successfully avert deaths and disability and significantly ease the tobacco-attributable economic burden. Every tobacco-attributable death or disease event affects individuals, their families and society as a whole. In 30 years from now, the Latin American population will still be affected by the decisions made today—or even worse, suffering from the consequences of the decisions not made.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was not required for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @APichonRiviere, @Cesar Loza@CsarLoza12, @AlfrePalacios13
Correction notice The article has been corrected since it was published online. The paper has now open access CC BY-NC licence. 24th May 2023.
Contributors Conceptualisation—AP-R, AB, FA, AA. Data curation, AP-R, AB, FC, AP, LMR-S, BL, MP, BSDMJ, TV, EPT, NA, CL, MC-R. Formal analysis—AP-R, AB, AA, FC, AC, LP, FA, AP, LMR-S, BL, MP, BSDMJ, TV, EPT, NA, CL, MC-R. Funding acquisition—AP-R, AB, AA. Investigation—AP-R, AB, AC, LP, FA, AA, AP, LMR-S. Methodology—AP-R, AB, AC, AP. Project administration—AP-R, AB, AA. Software—AP-R, AC. Supervision—AP-R, AB, AP, JR, AA. Validation—AP, AA, FA, LMR-S, MP, BSDMJ, TV, EPT, NA, CL, MC-R. Visualisation—AP-R, JR. Writing—AP-R, AA, AB, FC, AP. Original draft and writing—AP-R, AA, AB, AP. Review and editing of manuscript—all authors. AP-R is the guarantor for overall content.
Funding International Development Research Centre (IDRC), Canada.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.