When Less is More: Vaping Low-Nicotine vs. High-Nicotine E-Liquid is Compensated by Increased Wattage and Higher Liquid Consumption

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
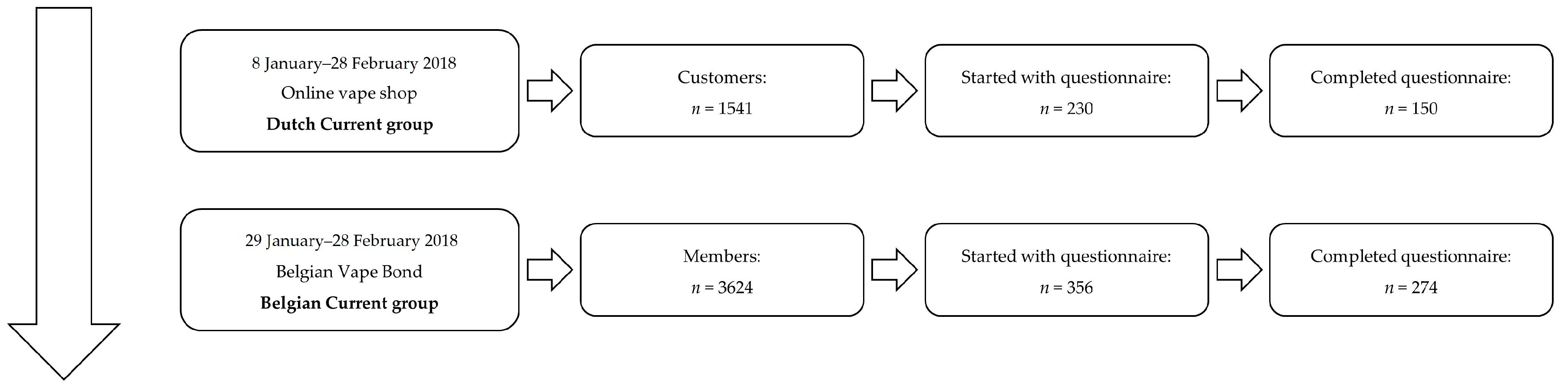
2.1. Participants
2.2. Measures
2.3. Procedure
2.4. Statistical Analyses and Structure of Presentation of Results
3. Results
3.1. Sociodemographic Characteristics
3.2. Smoking History and Smoking Status
3.3. Vaping Status and Technical Aspects
3.4. Reasons for Vaping
3.5. Perceived Harmfulness
3.6. Improvements in Health and Well-Being and Experienced Disadvantages
3.7. Nicotine Dependency
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Variable | Dutch Current Group | Belgian Current Group | ||
|---|---|---|---|---|
| n | M (SD) or % | n | M (SD) or % | |
| Demographic characteristics | ||||
| Age (years) | 150 | 48.5 (11.0) | 274 | 40.9 (10.0) |
| Sex (men/women/X) | 85/63/2 | 56.7/42.0/1.3 | 215/58/1 | 78.4/21.2/0.4 |
| Nationality | ||||
| Belgian | 4 | 2.7 | 234 | 85.4 |
| Dutch | 144 | 96.0 | 21 | 7.7 |
| French | 0 | 0.0 | 17 | 6.2 |
| German | 1 | 0.7 | 0 | 0.0 |
| Dutch-Greek | 1 | 0.7 | 0 | 0.0 |
| Swedish | 0 | 0.0 | 1 | 0.4 |
| Swiss | 0 | 0.0 | 1 | 0.4 |
| Educational degree | ||||
| Primary | 3 | 1.4 | 4 | 1.5 |
| Secondary school | 67 | 44.7 | 139 | 50.7 |
| Higher education, non-university (bachelor degree) | 58 | 38.7 | 75 | 27.4 |
| Higher education, university (master degree) | 16 | 10.7 | 30 | 10.9 |
| Other (e.g., higher professional education - HBO, airplane technology, gardener) | 2 | 1.3 | 15 | 5.5 |
| I prefer not to answer | 3 | 2.0 | 11 | 4.0 |
| Employment status | ||||
| Blue-collar | 71 | 47.3 | 76 | 27.7 |
| Self-employed | 23 | 15.3 | 36 | 13.1 |
| White-collar | 8 | 5.3 | 109 | 39.8 |
| Not working due to illness/disability | 10 | 6.7 | 14 | 5.1 |
| Retired | 6 | 4.0 | 11 | 4.0 |
| Houseman/housewife | 11 | 7.3 | 3 | 1.1 |
| Looking for a job | 3 | 2.0 | 10 | 3.6 |
| Studying | 4 | 2.7 | 5 | 1.8 |
| Other (e.g., job in military) | 8 | 5.3 | 7 | 2.6 |
| I prefer not to answer | 6 | 4.0 | 3 | 1.1 |
| Net income per month (in €) | 2337.7 (1297.0) | 2025.9 (844.4) | ||
| I prefer not to answer | 64 | 42.7 | 97 | 35.4 |
| Variable | Dutch Current Group | Belgian Current Group | ||
|---|---|---|---|---|
| n | M (SD) or % | n | M (SD) or % | |
| Smoking history | ||||
| Ever smoked | 150 | 100 | 273 | 99.6 |
| Age of smoking initiation | 146 | 15.8 (4.0) | 244 | 15.2 (3.3) |
| Characteristics of current smokers | 17 | 27 | ||
| Years smoking | 17 | 23.5 (15.3) | 27 | 23.0 (11.4) |
| Cigarettes smoked per day | 15 | 10.3 (7.0) | 23 | 9.0 (7.1) |
| Made at least one quit attempt | 16 | 94.1 | 25 | 92.6 |
| Number of quit attempts | 16 | 3.25 (1.7) | 24 | 3.79 (3.5) |
| Fagerström Test for Cigarette Dependence (FTCD) | 15 | 3.6 (2.2) | 23 | 4.0 (2.0) |
| Motivation to quit smoking | 17 | 27 | ||
| I don’t want to quit | 11.8 | 3.7 | ||
| I think it is better to quit, but I don’t want to | 23.5 | 3.7 | ||
| I want to quit, but I don’t know when | 47.1 | 25.9 | ||
| I really want to quit, but I don’t know when | 0 | 14.8 | ||
| I want to quit within the next 3 months | 5.9 | 22.2 | ||
| I want to quit within the next month | 5.9 | 7.4 | ||
| I want to quit now | 5.9 | 22.2 | ||
| Smoking cessation methods used/once being effective | 149 | 271 | ||
| Nicotine patches | 61/13 | 40.9/8.7 | 100/17 | 36.9/6.3 |
| Nicotine gum | 54/5 | 36.2/3.4 | 97/10 | 35.8/3.7 |
| Nicotine tablets | 22/2 | 14.8/1.3 | 46/2 | 17.0/0.7 |
| Inhaler | 1/0 | 0.7/0 | 14/0 | 5.2/0 |
| Mouth spray | 5/0 | 3.4/0 | 31/3 | 11.4/1.1 |
| Smoking cessation medication | 20/9 | 13.4/6.0 | 57/20 | 21.0/7.4 |
| Professional help from e.g., a tobacco counsellor | 11/3 | 7.4/2.0 | 32/6 | 11.8/2.2 |
| E-cig | 93/97 | 62.4/65.1 | 217/233 | 80.1/86.0 |
| None/will power | 52/36 | 34.9/24.2 | 104/43 | 38.4/15.9 |
| Other (e.g., book, hypnosis, acupuncture) | 14/11 | 9.4/7.4 | 9/7 | 3.3/2.6 |
| Characteristics of former smokers | ||||
| Years smoking | 149 | 28.6 (21.1) | 270 | 22.7 (10.2) |
| Number of quit attempts before successfully quit | 129 | 11.4 (87.7) | 232 | 4.5 (7.9) |
References
- Van Gucht, D.; Adriaens, K.; Baeyens, F. Online vape shop customers who use c-cigarettes report abstinence from smoking and improved quality of life, but a substantial minority still have vaping-related health concerns. Int. J. Environ. Res. Public Health 2017, 14. [Google Scholar] [CrossRef]
- Volesky, K.D.; Maki, A.; Scherf, C.; Watson, L.M.; Cassol, E.; Villeneuve, P.J. Characteristics of e-cigarette users and their perceptions of the benefits, harms and risks of e-cigarette use: Survey results from a convenience sample in Ottawa, Canada. Health Promot. Chronic Dis. Prev. Can. Res. Policy Pract. 2016, 36, 130–138. [Google Scholar] [CrossRef]
- Tackett, A.P.; Lechner, W.V.; Meier, E.; Grant, D.M. Biochemically verified smoking cessation and vaping beliefs among vape store customers. Addiction 2015, 110, 5. [Google Scholar] [CrossRef] [PubMed]
- Baweja, R.; Curci, K.M.; Yingst, J.; Veldheer, S.; Hrabovsky, S.; Wilson, S.J.; Foulds, J. Views of experienced electronic cigarette users. Addict. Res. Theory 2016, 24, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F. Electronic cigarettes: A survey of users. BMC Public Health 2010, 10, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Goniewicz, M.L.; Lingas, E.O.; Hajek, P. Patterns of electronic cigarette use and user beliefs about their safety and benefits: An internet survey. Drug Alcohol Rev. 2013, 32, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Farsalinos, K.E.; Romagna, G.; Tsiapras, D.; Kyrzopoulos, S.; Voudris, V. Characteristics, perceived side effects and benefits of electronic cigarette use: A worldwide survey of more than 19,000 consumers. Int. J. Environ. Res. Public Health 2014, 11, 4356–4373. [Google Scholar] [CrossRef] [PubMed]
- Chaumont, M.; de Becker, B.; Zaher, W.; Culié, A.; Deprez, G.; Mélot, C.; Reyé, F.; Van Antwerpen, P.; Delporte, C.; Debbas, N.; et al. Differential effects of e-cigarette on microvascular endothelial function, arterial stiffness and oxidative stress: A randomized crossover trial. Sci. Rep. 2018, 10, 10378. [Google Scholar] [CrossRef] [PubMed]
- Ashton, H.; Stepney, R.; Thompson, J.W. Self-titration by cigarette smokers. Br. Med. J. 1979, 2, 357–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodward, M.; Tunstall-Pedoe, H. Self-titration of nicotine: Evidence from the Scottish Heart Health Study. Addiction 1993, 88, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Dawkins, L.E.; Kimber, C.F.; Doig, M.; Feyerabend, C.; Corcoran, O. Self-titration by experienced e-cigarette users: Blood nicotine delivery and subjective effects. Psychopharmacology 2016, 233, 2933–2941. [Google Scholar] [CrossRef] [PubMed]
- Dawkins, L.; Cox, S.; Goniewicz, M.; McRobbie, H.; Kimber, C.; Doig, M.; Kośmider, L. ‘Real-world’ compensatory behaviour with low nicotine concentration e-liquid: Subjective effects and nicotine, acrolein and formaldehyde exposure. Addiction 2018, 113, 1874–1882. [Google Scholar] [CrossRef] [PubMed]
- Qualtrics. Qualtrics; Computer Software; Qualtrics: Provo, UT, USA, 2016. [Google Scholar]
- Fagerström, K. Determinants of tobacco use and renaming the FTND to the Fagerström Test for Cigarette Dependence. Nicot. Tob. Res. 2012, 14, 75–78. [Google Scholar] [CrossRef] [PubMed]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0; Computer Software; IBM Corp: Armonk, NY, USA, 2016. [Google Scholar]
- Benowitz, N.L.; Jacob, P. Daily intake of nicotine during cigarette smoking. Clin. Pharmacol. Ther. 1984, 35, 499–504. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, G.; Colard, S.; Breiev, K.; Sulzer, P.; Biel, S.S.; Cahours, X.; Pritchard, J.D.; Burseg, K.M.M. An experimental method to determine the concentration of nicotine in exhaled breath and its retention rate following use of an electronic cigarette. J. Envion. Anal. Chem. 2015, 2. [Google Scholar] [CrossRef]
- Armitage, A.K.; Dixon, M.; Frost, B.E.; Mariner, D.C.; Sinclair, N.M. The effect of tobacco blend additives on the retention of nicotine and solanesol in the human respiratory tract and on subsequent plasma nicotine concentrations during cigarette smoking. Chem. Res. Toxicol. 2004, 17, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Schere, G.; Lee, P.N. Smoking behavior and compensation: A review of the literature with meta-analysis. Regul. Toxicol. Pharmacol. 2014, 70, 615–628. [Google Scholar] [CrossRef] [PubMed]
- Etter, J.F. A longitudinal study of cotinine in long-term daily users of electronic cigarettes. Drug Alcohol. Depend. 2016, 160, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Soar, K.; Kimber, C.; McRobbie, H.; Dawkins, L.E. Nicotine absorption from e-cigarettes over 12 months. Addict. Behav. 2018. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.N. Summary of the epidemiological evidence relating snus to health. Regul. Toxicol. Pharm. 2011, 59, 197–214. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.N. The effect on health of switching from cigarettes to snus—A review. Regul. Toxicol. Pharm. 2013, 66, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.N. Epidemiological evidence relating snus to health—an updated review based on recent publications. Harm. Red. J. 2013, 10, 36. [Google Scholar] [CrossRef] [PubMed]
- Mills, E.J.; Thorlund, K.; Eapen, S.; Wu, P.; Prochaska, J.J. Cardiovascular events associated with smoking cessation pharmacotherapies: A network meta- analysis. Circulation 2014, 129, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Rodu, B. The scientific foundation for tobacco harm reduction, 2006–2011. Harm. Red. J. 2011, 8, 19. [Google Scholar] [CrossRef] [PubMed]
- Nitzkin, J.L. The case in favor of e-cigarettes for tobacco harm reduction. Int. J. Environ. Res. Pub. Health. 2014, 11, 6459–6471. [Google Scholar] [CrossRef]
- Van Gucht, D.; Baeyens, F. Health professionals in Flanders perceive the potential health risks of vaping as lower than those of smoking, but do not recommend using e-cigarettes to their smoking patients. Harm. Reduct. J. 2016. [Google Scholar] [CrossRef] [PubMed]
- Royal Society for Public Health. Nicotine “No More Harmful to Health than Caffeine”. 2015. Available online: https://www.rsph.org.uk/about-us/news/nicotine--no-more-harmful-to-health-than-caffeine-.html (accessed on 25 January 2019).
- Jackler, R.K.; Ramamurthi, D. Nicotine arms race: JUUL and the high-nicotine product marker. Tob. Control 2019. [Google Scholar] [CrossRef] [PubMed]
- Tokle, R.; Pedersen, W. “Cloud Chasers” and “Substitutes”: E-cigarettes, vaping subcultures and vaper identities. Sociol. Health Illn. 2019. [Google Scholar] [CrossRef] [PubMed]

| Variable | Dutch Current Group | Belgian Current Group | ||
|---|---|---|---|---|
| n | M (SD) or % | n | M (SD) or % | |
| Ever Vaped | 150 | 274 | ||
| Yes | 96.7 | 99.6 | ||
| Vaping frequency (in ever vapers) | 145 | 273 | ||
| Every day | 98.6 | 94.5 | ||
| Some days a week | 1.3 | 2.6 | ||
| Former vapers | 0.0 | 2.9 | ||
| Months vaping (in ever vapers) | 46.8 (21.8) | 37.1 (35.6) | ||
| Motivation to quit vaping | 145 | 265 | ||
| I don’t want to quit | 33.8 | 55.8 | ||
| I think it is better to quit, but I don’t want to | 28.3 | 14.0 | ||
| I want to quit, but I don’t know when | 26.9 | 19.2 | ||
| I really want to quit, but I don’t know when | 7.6 | 9.8 | ||
| I want to quit within the next 3 months | 2.8 | 1.1 | ||
| I want to quit within the next month | 0.7 | 0.0 | ||
| I want to quit now | 0.0 | 0.0 | ||
| Inhalation | 145 | 265 | ||
| Usually mouth-to-lung inhalation | 66.9 | 16.2 | ||
| Usually direct lung inhalation | 17.2 | 60.8 | ||
| Both | 15.9 | 23.0 | ||
| Dry hit | 145 | 265 | ||
| Never | 8.3 | 6.8 | ||
| Seldom | 54.5 | 83.4 | ||
| Regularly | 5.5 | 4.9 | ||
| I don’t know what a dry hit is | 31.7 | 4.9 | ||
| Variable | Dutch Current Group | Belgian Current Group | ||
|---|---|---|---|---|
| n | M (SD) or % | n | M (SD) or % | |
| Volume of e-liquid (mL/week) | 141 | 21.8 (15.2) | 263 | 62.9 (51.0) |
| Nicotine concentration (mg/mL) | 143 | 8.9 (5.3) | 263 | 3.3 (3.9) |
| PG/VG ratio | 145 | 63.5/36.5 | 265 | 36.8/63.2 |
| Coil resistance (ohm) | 116 | 1.3 (0.7) | 249 | 0.4 (0.4) |
| Power (W) | 82 | 26.6 (36.9) | 253 | 61.0 (40.4) |
| Type of device | 145 | 264 | ||
| with possibility to regulate wattage or voltage with temperature control | 16.6 | 61.0 | ||
| with possibility to regulate wattage or voltage but no temperature control | 41.4 | 22.7 | ||
| no possibility to regulate wattage/voltage/ temperature | 35.9 | 16.3 | ||
| I don’t know | 6.2 | 0.0 | ||
| Reasons for Vaping | Dutch Current Group | Belgian Current Group | ||
|---|---|---|---|---|
| Start (n = 145) | Continue (n = 145) | Start (n = 273) | Continue (n = 265) | |
| To quit smoking | 74.7 | 39.3 | 81.8 | 49.6 |
| Because it is healthier than tobacco cigarettes | 54.0 | 44.0 | 48.2 | 44.9 |
| Financial reasons | 32.0 | 20.0 | 16.4 | 7.7 |
| To smoke less | 12.7 | 8.7 | 22.3 | 5.8 |
| Out of curiosity | 15.3 | 2.7 | 16.8 | 0.4 |
| Different flavours | 7.3 | 5.3 | 14.6 | 26.3 |
| Other (e.g., reduce nicotine intake, pregnancy) | 6.7 | 15.3 | 6.9 | 10.9 |
| Because smoking is prohibited in certain places | 12.0 | 8.7 | 3.3 | 1.8 |
| Others offered it | 6.0 | 0.0 | 6.2 | 0.4 |
| To pass time | 4.0 | 7.3 | 2.2 | 19.7 |
| Dual use | 2.0 | 2.0 | 2.9 | 2.2 |
| Others do it | 0.7 | 0.0 | 0.4 | 0.0 |
| Because it is tasty and I enjoy it | 44.7 | 42.0 | ||
| Variable | Not Harmful at All | Not That Harmful | Neutral | Harmful | Very Harmful |
|---|---|---|---|---|---|
| Smoking | 0.0/0.04 | 0.0/0.0 | 1.3/1.1 | 20.7/17.5 | 78.0/81.0 |
| Vaping | 7.3/31.8 | 40.0/52.6 | 28.0/9.9 | 22.7/4.7 | 2.0/1.1 |
| Smoking cessation medications | 7.3/2.6 | 14.0/11.7 | 50.0/39.1 | 27.3/39. 1 | 1.3/7.7 |
| NRT | 7.3/5.8 | 24.0/21.9 | 45.3/47.1 | 21.3/20.1 | 2.0/5.1 |
| Variable | Totally Disagree | Disagree | Neutral | Agree | Totally Agree | Ws | z | Mdn Belgian | MdnDutch |
|---|---|---|---|---|---|---|---|---|---|
| My craving for a tobacco cigarette has decreased | 0.5 | 1.4 | 3.8 | 11.2 | 83.0 | 54,861.0 ** | −3.04 | 1 | 1 |
| I could decrease my smoking consumption | 2.2 | 1.9 | 5.7 | 12.2 | 78.0 | 53,818.0 *** | −3.97 | 1 | 1 |
| I could quit smoking | 1.9 | 4.5 | 5.5 | 6.7 | 81.3 | 53,887.5 *** | −4.14 | 1 | 1 |
| I have fresher breath | 0.2 | 0.7 | 8.1 | 19.1 | 71.8 | 53,664.0 *** | −3.80 | 1 | 1 |
| My physical condition and health has improved | 1.0 | 1.2 | 8.9 | 16.7 | 72.2 | 54,289.5 ** | −3.14 | 1 | 1 |
| I can breathe better | 0.5 | 2.2 | 12.2 | 21.8 | 63.4 | 51,672.5 *** | −5.49 | 1 | 2 |
| I gain more pleasure from vaping than from smoking | 1.4 | 3.8 | 14.8 | 14.6 | 65.3 | 49,844.0 *** | −7.39 | 1 | 2 |
| I have improved smell | 0.2 | 2.2 | 17.9 | 20.1 | 59.6 | 52,220.0 *** | −4.81 | 1 | 2 |
| I have improved taste | 0.5 | 2.2 | 17.2 | 22.5 | 57.7 | 51,649.5 *** | −5.30 | 1 | 2 |
| I bother bystanders less | 2.9 | 7.9 | 20.8 | 23.0 | 45.5 | 24,348.0 *** | −5.45 | 2 | 1 |
| My appetite has improved | 0.2 | 4.8 | 42.6 | 19.9 | 32.5 | 53,479.5 ** | −3.37 | 2 | 3 |
| My quality of sleep has improved | 1.4 | 5.7 | 46.2 | 19.4 | 27.3 | 50,710.0 *** | −5.90 | 2 | 3 |
| I am in a better mood | 1.2 | 4.8 | 50.5 | 20.3 | 23.2 | 53,882.0 ** | −3.06 | 3 | 3 |
| I can vape in more contexts | 12.2 | 16.0 | 23.7 | 16.7 | 31.3 | 21,742.0 *** | −7.56 | 3 | 1 |
| I have more technical issues | 13.2 | 27.0 | 31.8 | 18.7 | 9.3 | 28,920.0 | −1.28 | 3 | 3 |
| Variable | Never | Seldom | Sometimes | Often | Always | Ws | z | MdnBelgian | MdnDutch |
|---|---|---|---|---|---|---|---|---|---|
| Dry mouth | 36.9 | 28.2 | 27.6 | 6.5 | 0.8 | 25,919.5 ** | −3.31 | 2 | 1.5 |
| Dry throat | 46.6 | 30.1 | 20.6 | 2.4 | 0.3 | 28,059.0 | −1.37 | 2 | 1 |
| Increased weight | 64.2 | 14.4 | 11.7 | 8.1 | 1.6 | 53,675.0 | −0.66 | 1 | 1 |
| Cough tendencies | 54.2 | 36.0 | 8.9 | 0.8 | 0.0 | 53,839.5 | −0.47 | 1 | 1 |
| Bad taste upon inhaling | 50.7 | 41.5 | 7.9 | 0.0 | 0.0 | 52,087.5 * | −2.20 | 1 | 2 |
| Unpleasant sensation in throat when inhaling | 58.3 | 32.8 | 8.1 | 0.3 | 0.5 | 51,247.0 ** | −3.07 | 1 | 2 |
| Bad taste (“vaper’s tongue”) | 64.0 | 25.5 | 9.8 | 0.8 | 0.0 | 25,499.5 *** | −4.14 | 1 | 1 |
| Worrying about my health | 74.0 | 14.6 | 8.9 | 2.4 | 0.0 | 51,612.0 ** | −2.98 | 1 | 1 |
| Sleeping difficulties | 78.9 | 12.5 | 4.9 | 3.3 | 0.5 | 51,867.0 ** | −2.93 | 1 | 1 |
| Headache | 74.3 | 17.3 | 7.3 | 0.8 | 0.3 | 53,726.0 | −0.68 | 1 | 1 |
| Bad physical condition | 80.5 | 12.7 | 3.8 | 2.2 | 0.8 | 51,546.5 ** | −3.29 | 1 | 1 |
| Increased heart rate or palpitations | 79.7 | 14.1 | 6.0 | 0.3 | 0.0 | 52,056.0 ** | −2.72 | 1 | 1 |
| Throat ache | 75.6 | 20.6 | 3.5 | 0.3 | 0.0 | 52,335.5 * | −2.31 | 1 | 1 |
| Breathing difficulties (shortness of breath, breathlessness) | 79.4 | 14.4 | 5.1 | 1.1 | 0.0 | 51,141.0 *** | −3.88 | 1 | 1 |
| Coughing up slimes | 79.4 | 14.4 | 5.7 | 0.5 | 0.0 | 52,316.0 * | −2.45 | 1 | 1 |
| Unpleasant odors | 87.0 | 10.6 | 2.2 | 0.3 | 0.0 | 53,084.5 | −1.81 | 1 | 1 |
| Bad sense of smell | 89.4 | 8.4 | 1.1 | 1.1 | 0.0 | 52,493.0 ** | −2.850 | 1 | 1 |
| Bronchitis | 90.5 | 8.4 | 0.5 | 0.3 | 0.3 | 28,512.0 | −1.72 | 1 | 1 |
| Variable | Dutch Current Group | Belgian Current Group | ||
|---|---|---|---|---|
| n | M (SD) or % | n | M (SD) or % | |
| Nicotine dependency | 145 | 64.8 (27.9) | 264 | 41.9 (29.4) |
| Afraid to start smoking again or to completely switch back to tobacco cigarettes | ||||
| Current vapers with a smoking history | 96 | 1.6 (2.5) | 215 | 1.7 (2.6) |
| Dual users | 18 | 3.0 (2.2) | 31 | 4.2 (3.4) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smets, J.; Baeyens, F.; Chaumont, M.; Adriaens, K.; Van Gucht, D. When Less is More: Vaping Low-Nicotine vs. High-Nicotine E-Liquid is Compensated by Increased Wattage and Higher Liquid Consumption. Int. J. Environ. Res. Public Health 2019, 16, 723. https://doi.org/10.3390/ijerph16050723
Smets J, Baeyens F, Chaumont M, Adriaens K, Van Gucht D. When Less is More: Vaping Low-Nicotine vs. High-Nicotine E-Liquid is Compensated by Increased Wattage and Higher Liquid Consumption. International Journal of Environmental Research and Public Health. 2019; 16(5):723. https://doi.org/10.3390/ijerph16050723
Chicago/Turabian StyleSmets, Jorien, Frank Baeyens, Martin Chaumont, Karolien Adriaens, and Dinska Van Gucht. 2019. "When Less is More: Vaping Low-Nicotine vs. High-Nicotine E-Liquid is Compensated by Increased Wattage and Higher Liquid Consumption" International Journal of Environmental Research and Public Health 16, no. 5: 723. https://doi.org/10.3390/ijerph16050723