Article Text

Abstract
Objective To assess how levels of tobacco control funding for low-income and middle-income countries (LMIC) changed following the 2008–2009 global economic downturn.
Methods In order to estimate the amount of tobacco control funding in LMICs, we created an integrated database of Development Assistance to Control Tobacco (DACT). This database includes data on funding from bilateral and multilateral donors, non-governmental organisations, private foundations and the corporate sector. The database contains information on 1389 disbursements awarded by 30 entities between 2000 and 2012.
Results DACT declined only marginally from US$68.8 million (US$0.016 per adult) in 2009 to US$68.2 million (US$0.016 per adult) in 2011, but deviated significantly from its 2000 to 2009 trend. The sources of funding remain highly concentrated, with nearly a half of the money coming from the Bloomberg Initiative and the Bill & Melinda Gates Foundation in 2011. The relative importance of institutional and research grants has declined.
Conclusions Our findings are consistent with the patterns in general levels of development assistance for health: after a decade of rapid growth, funding for tobacco control activities in LMICs has levelled off. Just as the tobacco control community is beginning to envision the endgame for tobacco, the funding remains erratic, inadequate, and highly vulnerable due to its level of concentration. Innovative financing mechanisms might help to increase the funding pool.
- funding
- development assistance
- aid
- crisis
Statistics from Altmetric.com
Introduction
While most developing countries put the global economic downturn behind them, by 2011 developed countries were still struggling with crisis-related problems.1 ,2 This economic hardship has resulted in deep cuts in development assistance aimed at promoting economic, social, political and health development in low-income and middle-income countries (LMIC). Declines in government revenues have led many donor countries to reduce their development funding. Countries struck hardest by the crisis, such as Spain, Iceland and Greece, cut their aid funding by more than a third from 2008 to 2011.3 With falling stock market prices, many foundations found their assets declining, which drove them to revise their funding decisions. In the USA, where most of the world's wealthiest charitable foundations are based, the foundations’ international giving declined by more than 30% from 2008 to 2010, a drop larger than the decline in overall foundations’ giving.4 Development assistance for health, a vital component of development aid, was not spared. After nearly two decades of sustained growth, aid for health levelled off in 2010–2011.5
Before the global economic downturn, funding for development assistance for health was surging. Between 1990 and 2010, the total amount of development assistance to improve health in LMICs more than quadrupled in nominal terms, from US$5.6 billion to US$26.9 billion.6 ,7 Many new nongovernmental organisations and public–private partnerships were created to join the efforts of the traditional bilateral and multilateral donors in providing health aid for the countries in need.6 Additionally, local public health expenditures in LMICs tripled between 1995 and 2010, as these developing economies strengthened their institutions and public policies, and increased their ability to finance their health needs.5
This golden era for health aid ended in 2010.5 Faced with increased fiscal constraints, donor countries’ bilateral agencies (with a few exceptions, eg, the UK and Australia) chose to constrict their health aid budgets.5 ,8 Health funding by some multilateral agencies, such as WHO, also fell.9 The general levelling-off in health aid since 2010 will soon have its toll in global health outcomes. For example, it is estimated that as an effect of the aid budget sequestration in the US in 2013 fiscal year alone, over 3000 more people will die due to malaria, and another 4200 more will die due to tuberculosis in developing countries.10
Although about 80% of tobacco-related deaths occur in LMICs, little is known about how international tobacco control aid for these countries changed during the recent period of economic hardship. The amounts of tobacco control funding for emerging and developing economies have been estimated by the Development Assistance to Control Tobacco (DACT) database hosted by the American Cancer Society (ACS), but the last data collection for this database took place in 2009.11 Before the global economic downturn, tobacco control as a health focus area had experienced growth in funding similar to that in the entire health sector. DACT increased from US$1.2 million (or US$0.0003 per adult) in 2000 to US$44.2 million in 2009 (or US$0.011 per adult). Additional assistance from domestic public funds reached US$37 million in 2008 (or US$0.009 per adult).11 The rapid growth in the health aid for tobacco control was mainly the result of the contributions of two large donors—the Bloomberg Philanthropies launching its tobacco control initiative in 2006, joined by the Bill & Melinda Gates Foundation in 2008.11
Despite the rapid growth from 2000 to 2009, funding for tobacco control remained a very small portion of total health aid. Although tobacco use, is second only to high blood pressure as a risk factor for the global burden of diseases in terms of disability-adjusted life-years (DALYs),12 and is also the only risk factor common to all four leading non-communicable diseases (cardiovascular disease, diabetes, cancer and chronic respiratory diseases),13 tobacco control received less than 0.1% of total health-related development assistance in 2007.11 In 2009, the DACT per person was between 13 and 90 times less than the amount recommended by WHO (US$0.10–$0.72) to control the demand for tobacco in LMICs.11
There is a substantial body of evidence indicating the beneficial effects of tobacco control funding. Numerous studies based on state-level data from the USA have found that tobacco control spending reduces smoking prevalence, smoking initiation among youth, per capita cigarette consumption, lung cancer rates, as well as smoking-related mortality (for comprehensive literature review, see eg, Max, Sung and Lightwood,14 as well as Chattopadhyay and Pieper15); tobacco control measures have been found to be highly cost-effective or, in some cases, even cost-saving.16 One study based on data from over a hundred LMICs found that external tobacco control aid has had positive effects on compliance with key provisions of the WHO Framework Convention on Tobacco Control (FCTC).17
Funding for tobacco control activities in LMICs has been shown to be erratic and inadequate.11 The recent crisis-related hardship that cut funding for many health priorities in the developing economies has also likely affected the already vulnerable DACT. The aim of this study is to assess how the levels of tobacco control funding for LMICs changed during the economic hardship.
Methods
The two major sources of information regarding development assistance for health are the Financing Global Health reports regularly published by the Institute of Health Metrics and Evaluation, and the Creditor Reporting System by the Organisation for Economic Co-operation and Development (OECD) Development Assistance Committee.5 ,18 These two reports, however, do not provide data detailed enough to extract information on tobacco control funding.
To provide an estimate of tobacco control funding for LMICs, as well as to study its sources and foci, we created a database of worldwide DACT. This database has been hosted by the International Tobacco Control Research programme at the ACS since 2008. We measured the DACT by tracking contributions made by public or private institutions from high-income countries to control tobacco use in LMICs.11
The most recent wave of data collection took place from May to December 2012. This was a follow-up to a previous data collection effort that took place in 2008 and 2009. We followed the same data collection method as in the previous waves (for detailed description of the methods, see Ross and Stoklosa11). First, we identified organisations that support tobacco control, or are the intermediaries in the funding process by contacting organisations from the previous data collection, and all other organisations referred to us in the data collection process—a snowball method. If the funding data were not publicly available, we asked the funding organisation to complete a questionnaire. We collected the following information: the title of the project, type of project (advocacy, institutional, research), type of funding (project-specific, general-operating, or a mix of the two), the names of collaborating agencies (if any), country where the project was implemented, name of institutions receiving the funds, the total amount and currency in which funds were provided, and the project's start and end dates. We solicited data about all tobacco control funding provided or channelled through an organisation since 2000. This allowed us to augment the data from the 2008 and 2009 waves with the information about the funding provided after 2009, and also to update information from the first two waves of data collection. During the 2012 wave of data collection, we approached 35 organisations and obtained information from 30 organisations, which gave us a response rate of 86% (see online supplementary appendix 2 for the list of participating agencies). We obtained information about 496 new tobacco control aid projects, and updated information on 114 projects. The entire updated database contains information on 1389 disbursements awarded between 2000 and 2012 to LMICs. The DACT often flows from funding sources through various intermediaries to implementing institutions. To ensure that the funding was counted only once, we manually verified the data and identified 56 projects that were captured in our database on multiple stages. For projects that went on for several years, the amount of the disbursement was divided equally between the years. We augmented our data on tobacco control funding for LMICs with external country-specific information on the adult population,19 the purchasing power parity (PPP),20 and exchange rates.21
Our study focuses on the 146 out of 195 WHO member states that, according to the World Bank classification, have been a low-income or middle-income country for at least 1 year between 2009 and 2012.22 This method excludes countries that have been a high-income country throughout that time (see online supplementary appendix 1 for the list of countries of focus).
For 82 of the 146 LMICs (56%) that reported to WHO assigning a part of their national budget for tobacco control activities,23 we were able to merge our database with WHO data, and compare the DACT to domestic public funding for tobacco control. As different countries provided information on their domestic public funding for different years, we compared the DACT with the domestic public funding for those years the information on the domestic public funding was provided.
We were able to attribute 83% of the disbursements to specific target countries, and adjust this funding for PPP to reflect differences in price levels between the countries. However, these country-specific disbursements represent only 48% of the total funding. This is mainly because some of the largest contributions in our database are not country-specific. For example, 35% of DACT funding goes to the WHO Tobacco Free Initiative, and the information about its budget allocation is not country-specific.
Since we included updated information on some projects, and engaged new organisations in the survey, our updated figures for years prior to 2010 are higher than those presented by Ross and Stoklosa.11 As the data for 2012 could not be complete due to data collection taking place that year, we focused our analyses on the 2000–2011 time period only.
When using the term ‘global economic downturn’, we refer to the declines in global gross domestic product between the years of 2008 and 2009.2 By ‘economic hardship’, we refer to economic problems that occurred after 2009, which followed the global economic downturn.1 ,2
Results
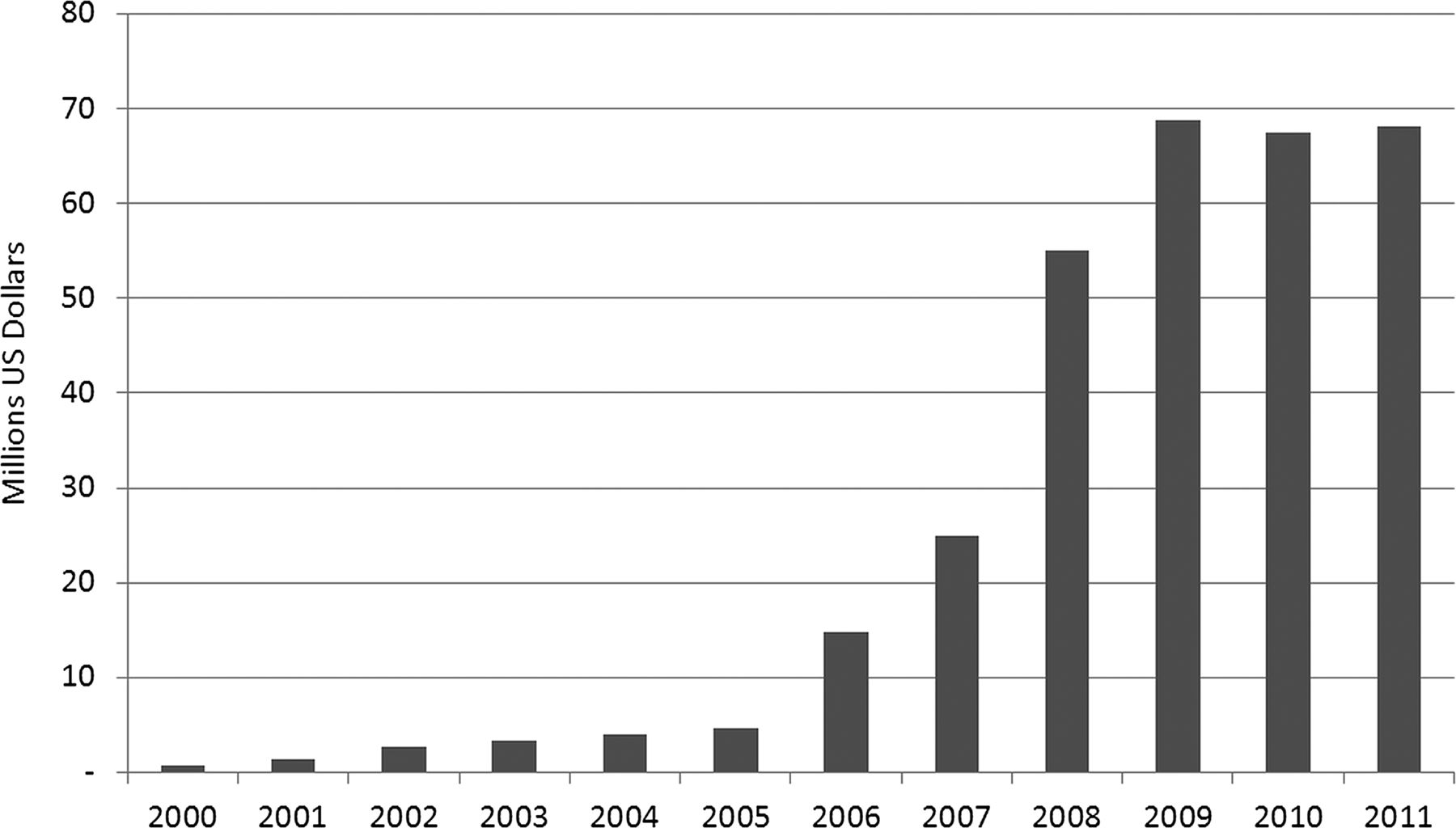
Funding for tobacco control in LMICs dropped in absolute terms from US$68.8 million (US$0.016 per adult) in 2009 to US$68.2 million (US$0.016 per adult) in 2011 (figure 1). This diversion from the 2000 to 2009 trend is statistically significant (see online supplementary appendix 3). However, the number of disbursements increased from 135 in 2009 to 165 in 2011.

Tobacco control aid for low-income and middle-income countries.
The change in DACT varied by donors. Bloomberg's and Gates’ grants, which remained the largest DACT contributions, increased by 9%: from US$29.0 million (42% of DACT) in 2009 to US$31.7 million (46% of DACT) in 2011. On the other hand, WHO, the largest multilateral donor, decreased the budget of the Tobacco Free Initiative by 5% from 2009 to 2011. The amounts of US government grants from the National Institutes of Health (NIH)/National Cancer Institute (NCI) fell by 13% from 2009 to 2011, while aid from Pfizer Foundation/Pfizer, the largest corporate donor, fell by over 80% at the same time.
While 44% of total funding awarded in 2009 went to tobacco control research, this percentage dropped to 20% in 2011. Similarly, the percentage of institutional grants supporting various tobacco control agencies in LMICs diminished from 7.3% of total funding in 2009 to 1.3% in 2011.
Five organisations that historically have supported tobacco control activities (Atlantic Philanthropies, Canadian Cancer Society, Canadian Tobacco Control Research Institute, National Health and Medical Research Council, Open Society Institute, and the Rockefeller Foundation) are now inactive in this area of health assistance, meaning that they reported no tobacco control-related funding after 2009. On the other hand, two organisations that during the previous data collections reported not being involved in tobacco control (Cancer Research UK and World Bank) are now investing in DACT. Their contribution to DACT, however, is still relatively small.
When analysing the funding that has been assigned to specific countries, we found that, despite the general levelling-off in DACT, there were 31 countries where PPP-adjusted tobacco control assistance increased from 2009 to 2011. PPP-adjusted DACT grew among large tobacco consumers, such as China, Bangladesh, Egypt, Ukraine, and Pakistan. On the other hand, PPP-adjusted DACT declined in other large tobacco-consuming and tobacco-producing countries, such as Brazil, India, Indonesia, Mexico, Philippines, Russia, Thailand, Turkey and Vietnam. Countries from sub-Saharan Africa were among the countries that experienced the largest percentage increase in DACT (Botswana, Madagascar, Mozambique, South Africa and Togo), as well as the largest decline in DACT from 2009 to 2011 (Burkina Faso, Eritrea, Gabon, Senegal and Tanzania).
Only 57 of the 146 countries (39%) received more than one tobacco control grant between 2009 and 2011. This indicates the continued irregularity of DACT. There are a few exceptions, such as China and India, that received funding on a regular basis (over 30 grants each between 2009 and 2011), and Bangladesh, Indonesia, Vietnam and the Philippines, which each received ≥15 tobacco control grants in that time period. In terms of the amount of funding, Dominican Republic, Hungary, Jamaica, Lebanon, Mauritius, Togo and Uruguay were in the top 10 countries with the largest per-adult PPP-adjusted DACT in 2009 and 2011 (figure 2).

{kind=link}
{kind=link}
Development assistance to control tobacco in 2011 (per adult, in purchasing power parity (PPP)-adjusted US$). Note: Does not include multinational disbursements (about 52% of total funding) and apply to the population aged 15+ based on World Health Statistics.19
In addition to DACT amounting to an overall average of US$0.016 per adult each year from 2009 to 2011, some LMICs decided to use a portion of their national budget to fund tobacco control activities. For those LMICs that reported their amount of domestic public funding to WHO,23 the general level of domestic public funding was lower than DACT, averaging US$0.010 per adult.
Discussion
Our findings are consistent with the general pattern of development assistance for health.5 After a period of exponential growth from 2000 to 2009, DACT levelled off. By 2010, funding had already lost its momentum, and even dropped compared to 2009. Some of this loss has been recovered by 2011, a pattern similar to that in overall health assistance.5
Despite the general levelling-off in DACT, there were regions where the assistance for tobacco control increased. Countries in sub-Saharan Africa were among those with the largest increase in PPP-adjusted DACT. Tobacco use is growing rapidly in the region,24 and various donors, including the Bill & Melinda Gates Foundation, and the International Development Research Centre, have realised that many deaths can be averted if action is taken at an early stage of the tobacco epidemic.
Another promising sign is the return of the World Bank to tobacco control. The absence of tobacco control in the Millennium Development Goals, a framework of eight international development-related goals that the UN member states committed to help achieve by 2015, had made it difficult to secure adequate funding for WHO FCTC implementation, especially in the LMICs.25 By stepping back into tobacco control, the World Bank can help to place tobacco control on the UN's post-2015 Development Agenda.26
Despite these positive signs, the general level of tobacco control funding remains low relative to the health impact of tobacco use. DACT is still far below the WHO-recommended amounts needed to control tobacco in LMICs.27 The momentum that was observed in the funding levels in the 2000s has been lost. If the current level of funding is not substantially increased to fund global tobacco control activities, approximately one billion people will die due to tobacco use in the 21st century.13
In most LMICs, domestic public funding for tobacco control is also miniscule. Tobacco control in many of the largest tobacco-consuming countries, such as China, India, Indonesia, Bangladesh, Mexico, Pakistan, Egypt, Philippines and Vietnam, must still rely more on foreign assistance than on domestic public funding.
While there has been only a slight decline in the total DACT from 2009 to 2011, the amount for tobacco control research grants dropped by over half, and institutional grants by over 80% in that period. This would not be surprising, if tobacco control institutions in LMICs had been funded long enough to become well established, and if enough research evidence on tobacco epidemic in LIMCs had been generated. At least for research, this is not true: there is a general scarcity of data and research evidence in LMICs. Yet, research using local data can provide the strongest support for adopting evidence-based policies.
Innovative financing mechanisms might help to increase the pool of tobacco control funding for LMICs. Among the mechanisms are: special levies on large and profitable companies, levies on currency and other financial transactions, bonds, excise tax on unhealthy food, tourism taxes, and tobacco and alcohol excise taxes.28 Because the funds available through traditional development assistance channels are not sufficient to reach health-related development goals, developed and developing countries are encouraged to explore new financing mechanisms.29 Some of these funding mechanisms are already in place. In France, for example, most of the funds generated by the ‘mandatory solidarity levy’ on airline tickets goes to UNITAID to support the scaling-up of treatments for HIV, tuberculosis and malaria.8 There is potential to implement similar funding mechanisms to support international tobacco control. For example, the solidarity tobacco contribution, a concept developed by WHO, recommends that countries consider dedicating a part of their tobacco tax revenue toward international health-financing purposes, and suggests that some of these funds are dedicated toward international tobacco control.29
The lack of tobacco control funding is a struggle for LMICs. As countries move from the middle-income to the high-income category, they often lose their eligibility to receive development assistance, including tobacco control funding. Some of the former biggest recipients of the Bloomberg funds, such as Uruguay, Chile, Poland and the Russian Federation, may be no longer eligible for Bloomberg funding because of the change in their income level. Inability to receive external tobacco control aid can have severe consequences, especially in those countries where tobacco companies have a strong presence. For example, the percentage of cigarette smokers among the 15–24-year age group in the Czech Republic, a country with a strong tobacco industry influence,30 has recently increased from 36.7% in 2009 to 43.4% in 2012.31 ,32 Among other factors, this hike was likely influenced by the lack of tobacco control resources in the country.
Although the World Bank country classification is a convenient criterion to use when determining countries’ eligibility for development assistance, donors should keep in mind that the classification is based on discretionary thresholds and is influenced by floating indicators, such as exchange rates. Therefore, donors should exercise good judgment when deciding which countries should receive funding and which should not. Our database indicates that there are some international donors (eg, Pfizer Foundation) that are willing to fund tobacco control activities in high-income countries.
Our system of data collection is not comprehensive.11 For example, we were not able to obtain data from funders like the Swedish International Development Agency or the NCI in France. On the other hand, we managed to capture data from organisations that were not included in the previous waves of data collection (eg, Canadian Institutes of Health Research). Even with some funding information missing, we captured data from all major international donors, which allows us to assess the general trend in tobacco control funding for LMICs.
In the process of collecting the DACT data, we encountered many challenges that could have been avoided if the information about tobacco control funding was publicly available. A good example of an increased effort to make the funding information publicly available is Canadian Research Information System,33 which contains detailed data on grants and awards funded by a number of (but not all) Canadian institutions. Even though WHO FCTC Article 21.1(c) calls for reporting and exchange of information on financial and technical assistance provided or received for tobacco control, the parties’ reports do not provide any data on the amounts of funding received. There is no systematic approach to collect and monitor tobacco control funding.
Conclusions
As recognised by signatories to WHO FCTC, the tobacco epidemic is an international problem. Since the transnational tobacco companies operate on the global scale, the epidemic can be stopped only through international involvement. The aid for low-income and middle-income countries to control tobacco is necessary because these economies lack resources (financial and institutional) to control the tobacco epidemic.
Even though the first decade of the twenty-first century marked great achievements in global tobacco control, funding for tobacco control in LIMCs levelled off. Just as the tobacco control community is beginning to envision the endgame for tobacco, it is imperative that the funding that is needed to finish the fight is secured.
What this paper adds
-
This article explores how tobacco control funding for low-income and middle-income countries changed in the era of economic hardship.
Acknowledgments
We would like to thank Teresa Aluku for her help with the data collection, Brian Le for his help with data cleaning and processing, as well as John Daniel for editing assistance. We are also grateful to all the donors listed in online supplementary appendix 1 who agreed to provide their funding information to us, and to all reviewers of this manuscript for providing valuable comments.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors MS and HR contributed to the entire manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.