Article Text

Abstract
Background Hookahs are increasingly being used in the USA and elsewhere. Despite the popularity of hookah bars, there is a paucity of research assessing the health effects of hookah smoke, and although New York City (NYC) bans indoor tobacco smoking, hookah lounges claim that they only use herbal products without tobacco. This study investigated levels of multiple indices of indoor air pollution in hookah bars in NYC.
Methods Air samples were collected in 8 hookah bars in NYC. Along with venue characteristics, real-time measurements of fine particulate matter (PM2.5), black carbon (BC), and carbon monoxide (CO), and total gravimetric PM, elemental carbon (EC), organic carbon (OC), and nicotine were collected in 1-2 hour sessions.
Results Overall, levels of indoor air pollution increased with increasing numbers of active hookahs smoked. The mean (SD) real time PM2.5 level was 1179.9 (939.4) µg/m3, whereas the filter-based total PM mean was 691.3 (592.6) µg/m3. The mean real time BC level was 4.1 (2.3) µg/m3, OC was 237.9 (112.3) µg/m3, and CO was 32 (16) ppm. Airborne nicotine was present in all studied hookah bars (4.2 (1.5) µg/m3).
Conclusions These results demonstrate that despite the ban on smoking tobacco products, at the very least, some NYC hookah bars are serving tobacco-based hookahs, and have elevated concentrations of indoor air pollutants that may present a health threat to visitors and employees. Therefore, there is an urgent need for better air quality monitoring in such establishments and policies to combat this emerging public health threat.
- Non-cigarette tobacco products
- Secondhand smoke
- Toxicology
- Nicotine
- Surveillance and monitoring
Statistics from Altmetric.com
Introduction
Tobacco use remains the leading preventable cause of death in the USA and globally.1 Between 2000 and 2011, the consumption of cigarettes in the USA decreased 33%. In contrast, the use of alternative tobacco products, such as hookahs (aka water pipes, nargiles, argiles or hubble bubble), cigarillos, cigars, bidis, kreteks and various forms of smokeless tobacco, increased a remarkable 123% over the same time period.2 Approximately 3% of US adolescents reported they were currently using and ∼8% reported having ever used hookahs.3 The Centers for Disease Control and Prevention (CDC) warns that the decrease in cigarette use is being ‘offset by increases in other forms of tobacco’.4
Public health concern stems from the common misconception that hookah smoke is a safer alternative to cigarettes because it is ‘filtered’ through water, despite research showing that hookah water pipes deliver tar, nicotine and carbon monoxide (CO) in even higher doses than cigarettes.5–7 Recent meta-analyses link hookah use to lung cancer, respiratory illness, periodontal diseases and low birth-weight outcomes8 and some studies have linked its use to oesophageal cancer,9 ,10 chromosomal abnormalities,11 decreased pulmonary and cardiovascular function,12 ,13 infertility,14 dental problems15 and infectious diseases.16
According to the Surgeon General’s Report, secondhand cigarette smoke includes more than 7000 toxic chemicals and about 70 have been identified as causing cancer.17 It is well known that secondhand cigarette smoke is responsible for causing ear infections, asthma attacks, respiratory symptoms and infection, and a greater risk of sudden infant death syndrome and thus there should be a health concern for children exposed to secondhand hookah smoke in the home.18 In adults who have never smoked, secondhand smoke (SHS) can cause heart disease and/or lung cancer.18 Most importantly, the report warns that there is no risk-free level of contact with SHS and that even brief exposure can be harmful to health.18
Because of the harmful and even lethal effects of SHS from tobacco products, many states have implemented smoke-free laws that protect patrons and staff from exposure to SHS. Thirty five US states, including New York, have passed laws that require 100% smoke-free workplaces including restaurants and bars.19 ,20 However, legislation is often limited to cigarette smoking or smoking of other nicotine-containing products, thereby exempting indoor smoking of claimed ‘tobacco free’ or ‘herbal’ hookah products.20–24 Among 73 of the 100 largest US cities that have banned cigarette smoking in bars, 69 have exemptions that allow hookah shisha (the plant material used in hookah water pipes that contains a number of components which may or may not include tobacco, non-tobacco plant material, flavouring, odorants, and/or molasses) smoking.24 In New York City (NYC), hookah use is permitted in hookah bars if the shisha does not contain tobacco. Of note, indoor hookah use in public spaces has recently been banned even in countries where hookah use is widespread and culturally rooted such as Lebanon, Kazakhstan, Turkey, parts of India and Saudi Arabia.21
One of the critical challenges faced by policymakers and public health officials is the scarcity of data on the quality of ambient air to which hookah bar patrons and workers are exposed and the health effects of mainstream and secondhand hookah smoking. To the best our knowledge, this is the first study performed in NYC hookah bars to assess indoor air quality for toxins and pollutants, such as particulate matter (PM2.5), black carbon (BC), CO and nicotine.
Methods
Location selection
Hookah bars in NYC were identified through online search engines ‘Yelp’ and ‘Google Map’ using key search terms ‘hookah/water pipe café’, ‘hookah/water pipe bar’, ‘hookah/water pipe lounge’. Most hookah bars are concentrated in the Lower East Side of Manhattan and a convenience sample of eight different venues, including one that was visited twice, were studied.
Air sampling and monitoring
Sample collection
Air quality data were collected between July and November of 2013. Air sampling occurred between 21:00 and 1:00 on Wednesday, Thursday, Friday or Saturday nights, when hookah bars have the most patrons. The research team entered each venue unannounced for a 1–2 h sampling session with handbags or backpacks containing air monitoring equipment. All equipment was concealed in the bag, except for a small portion of the tubing that protruded from one corner. Venue characteristics such as the number of hookahs being used at the time of sampling, active smokers and the general ventilation status of the bars were recorded in the field.
Styrene, 2-piece cassettes (SKC, Inc; Eighty Four, Pennsylvania, USA) were used to collect total PM samples on polytetrafluoroethylene (PTFE) (low trace element background; Pall Corp, Port Washington, New York, USA) for gravimetric and trace element analyses. Using prebaked (650°C overnight) quartz (Pall) filters, organic/elemental carbon (OC/EC) levels were analysed. The quartz fibre filters were undenuded and thus our samples likely collected a fraction of semivolatile organic vapours. After sampling, the quartz filters were sealed and transferred to a −20°C freezer shortly after collection. Sample flow rates were calibrated before each run using a dry gas metre (BIOS Dry Cal DC-Lite, Brandt Instruments, Prairieville, Louisiana, USA). Nicotine was sampled with an XAD-4 sampling tube (SKC, Inc) at a flow rate of 1.5 L/min and PTFE and quartz filters at 4 L/min. Filters and nicotine were sampled with personal sampling pumps with battery packs (BGI 400, BGI, Inc, Waltham, Massachusetts, USA). The handbags/backpacks also contained a microaethalometer (Model AE51, AethLabs, San Francisco, California, USA), a gas monitor (GrayWolf, Shelton, Connecticut, USA), and a pressure and humidity compensated aerosol monitor (pDR-1500, Thermo Fisher Scientific) to measure real time BC2.5 (1 min intervals), CO, and PM2.5 (1 min intervals) concentrations, respectively. A particle size selection device was attached to the inlet of the aethalometer and pDR-1500 to monitor PM2.5 and BC2.5.
Chemical speciation
Gravimetric analysis of PTFE filters was performed in an environmentally-controlled weighing facility (22°±1°C room temperature and 40%±2% relative humidity) using standard operating procedures. Filters were equilibrated to ambient conditions in the weighing facility for a minimum of 24 h before weighing. Samples collected on PTFE filters were analysed for 35 elements via energy dispersive X–ray fluorescence (XRF) (ARL QUANT'X X-Ray Fluorescence Spectrometer, Thermo Scientific) and the Environmental Protection Agency (EPA) compendium methods for metal speciation as described previously.25 Concentrations of elements were defined as above the detection limit if they were a minimum of three times the uncertainty of the measurements (3σ) and corrected for the mean of blank filters (n=6). Quartz filters were analysed for OC/EC with a Sunset Instruments carbon analyser calibrated with a sucrose solution (4.2 µg carbon/µL). Nicotine was measured by gas chromatography using NIOSH method 2551.26 Approximately 10% of all filters were field or laboratory blanks.
Results
During the peak hours, a number of variations were observed in the eight studied hookah bars, all of which could influence air quality measurements. The number of active hookah water pipes ranged from 4 to as many as 18 with an average of 9 per bar (table 1). The ventilation status also varied among venues, with some having multiple open windows and doors and others having none (table 1).
Hookah bar characteristics
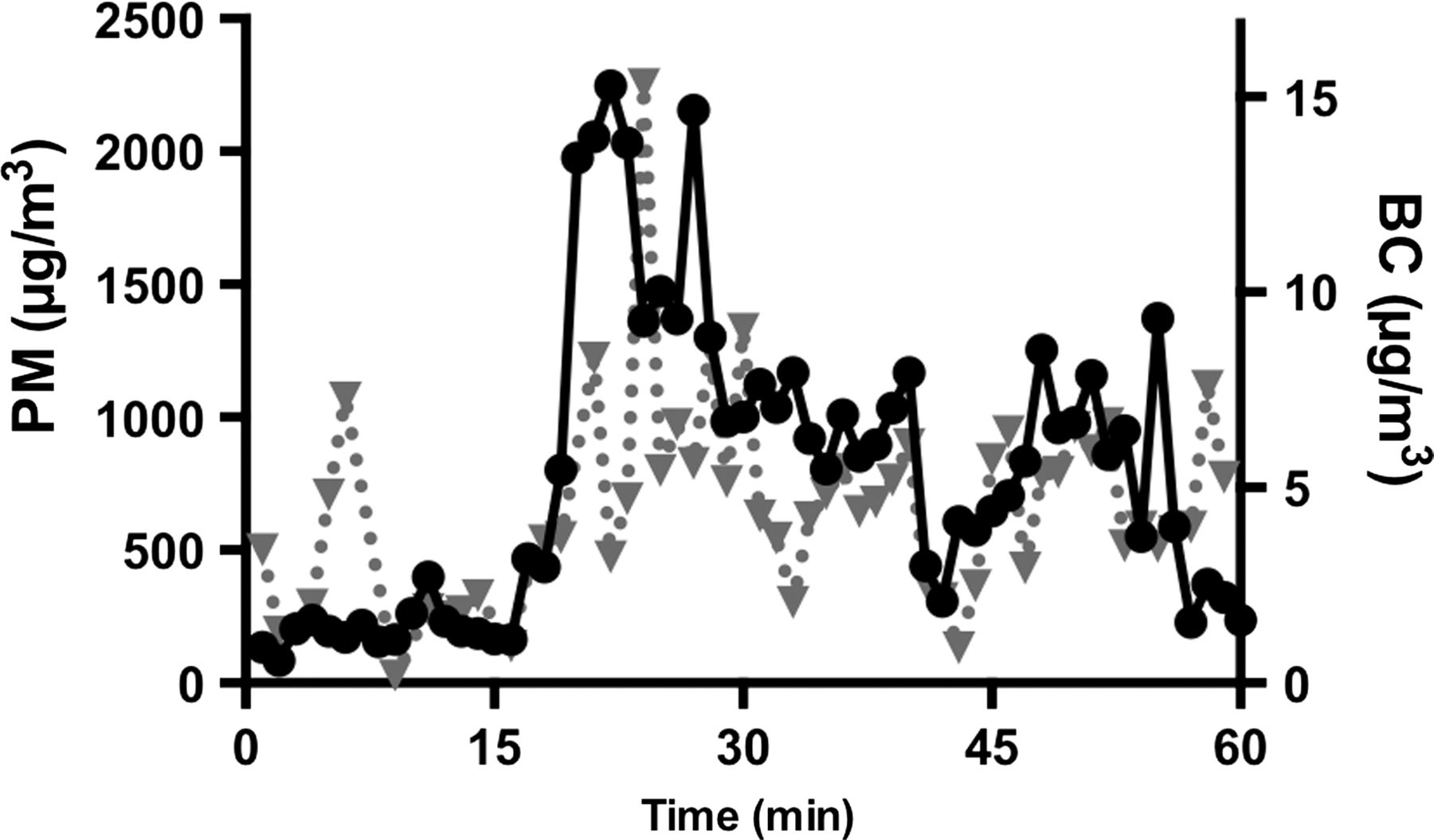
During the 1–2 h sampling periods, the mean real time PM2.5 concentration was 1180 µg/m3 with a range of 481–2986 µg/m3 (table 2). The gravimetric filter-based total PM mean of 691 µg/m3 (range of 109–1270) was lower than the real-time PM2.5 concentration. Both PM2.5 and BC concentrations varied nearly an order of magnitude during the sampling period (figure 1). BC and EC, however, made up only a small fraction of the particle mass. Mean BC level was 4.1 µg/m3 with a range of 1.2–7.6 µg/m3. Although the filter-based EC measurements should generally be equivalent to the real-time BC values, EC was below the detection limit for all but one hookah bar. OC accounted for a larger mass fraction of indoor particles with a mean concentration of 238 µg/m3 and a range of 59–404 µg/m3. Mean CO was 32 ppm with a range of 10–50 ppm.
Hookah bar air pollution concentrations

{kind=link}
Real time levels of particulate matter (PM)2.5 (solid black line and circles) and black carbon (BC, black carbon; dotted gray line and triangles) in hookah bar number 3 (1 min intervals).
Additionally, airborne nicotine was found in all establishments (table 2), despite the ban on the use of tobacco-based shisha in water pipes in NYC hookah bars. As shown in table 3, the elemental composition of the secondhand hookah smoke PM was dominated by Na, S, Cl, K and Ca. In general, the airborne elemental concentrations were less than 1 µg/m3 with a maximum value of 6 µg/m3 for Cl.
Trace element concentrations (ng/m3) in NYC hookah bars as measured by X-ray fluorescence
Discussion
To the best of our knowledge, this is the first study to assess indoor air quality in hookah bars in NYC, a city with the largest number of hookah bars in the US based on Internet searches. Although there are no indoor regulatory standards for air quality indices, the indoor hookah bar concentrations of ambient air pollutant and toxicants, such as PM2.5 and CO, were found to exceed the 24 h and 1 h US federal standards for outdoor PM2.5 and CO, respectively.27 The levels of EC and nicotine were below the occupational standards promulgated by the Occupational Safety and Health Administration, although these standards are intended for healthy workers and may not be applicable to the general population or susceptible individuals. Perhaps most importantly, measurable airborne concentrations of nicotine were found in all hookah bars studied, suggesting that tobacco-based shisha is, in fact, commonly used in NYC hookah bars, in violation of NYC laws. This suggests that there is an urgent need for official assessment to see if lounges are non-compliant with NYC law. The findings raise serious concerns about potential adverse health effects among patrons and employees of hookah bars. We believe the findings reported provide critical information to assist tobacco policy and public health officials in regulating hookah smoking in hookah bars in NYC.
An increasing number of studies have examined the presence of particulate air pollution in hookah bars. The first published study on indoor air quality of hookah bars measured PM2.5 in 10 hookah lounges in Oregon, USA.28 Those authors suggested that by comparison of the hookah smoke PM2.5 to the USA. EPA ambient air quality standard for PM2.5, the air quality in the hookah bars ranged from ‘unhealthy’ to ‘hazardous’, although it might not be appropriate to compare the 24 h PM2.5 standard to an acute indoor exposure. Subsequently, Cobb et al20 investigated the indoor air pollution, again measuring only PM2.5, in 28 hookah cafes in Virginia and reached similar conclusions. A Canadian study by Zhang et al21 extended these findings by examining not only airborne PM2.5, but also CO and nicotine levels. Their observed levels of CO and nicotine in Toronto hookah bars were 18 ppm and 3 µg/m3, respectively, similar to our findings in NYC. The results from these studies suggested a concern for adverse health effects due to exposure to secondhand hookah smoke in hookah hospitality venues.21 A more recent study of water pipe cafes in Baltimore, Maryland, USA found that concentrations of CO and PM2.5 were substantially elevated in water pipe cafes and were higher than in bars where cigarettes were smoked. While air nicotine concentrations were not as high as in cafes where cigarettes were smoked, the nicotine levels were significantly higher than in smoke-free bars and restaurants.29 The findings from the present study complement and extend those of the previous studies by assessing not only airborne PM, nicotine and CO, but also BC, EC, OC and trace elements in NYC hookah bars.
Among the selected locations, the real time mean PM2.5 concentration was 1,179 µg/m3 with a peak mean value of 2986 µg/m3 at one hookah venue. These values were higher than those reported for SHS levels in bars where and when cigarette smoking has been permitted in the USA, Scotland30 and Asia.31 In comparison, the gravimetric PM concentrations were, as expected, lower than the real time PM2.5 concentrations, likely due to measurement error possibly resulting from the presence of water, on the airborne secondhand hookah smoke particles, which may be removed (potentially along with volatile and semi-volatile compounds) during the PTFE filter equilibration period in the climate-controlled weighing facility. Regardless, the indoor particle concentrations were considerably higher than the ambient outdoor values, which were generally 5–15 µg/m3, as measured with the real time monitor just prior to entering and after exiting the NYC hookah bars (data not shown).
While ascertaining the indoor concentration of PM in hookah bars is critical in risk evaluations, particle composition is also important. The concentration ratio of combustion products of plant material used in shisha, including organic and EC compounds, depends on combustion efficiency and the burning/charring temperature of the shisha. This is the first study to report that the indoor BC concentration in hookah bars (4.1 µg/m3) was greater than outdoor ambient BC levels previously measured in the boroughs of NYC.32–34 However, BC accounted for less than 1% of the airborne particle mass in the secondhand hookah smoke, suggesting that it may not significantly contribute to the adverse effects of secondhand hookah smoke. On the other hand, OC (238 µg/m3) constituted a larger fraction of the secondhand hookah smoke and therefore, may play a more important role in adverse health effects. XRF analysis of trace elements was also performed and the results (table 3) show that Ca, Na, Cl, K, S and Mg are present in the greatest amounts in secondhand hookah smoke. As with BC, these elements accounted for a small fraction of the total PM mass concentration. Based on our limited sampling, however, the large variability in trace element concentrations among the hookah bars suggests that the source of the particles, that is, the charcoal and the shisha, differed from bar to bar.
This study also found that levels of CO, a gaseous component with a mean of 32 ppm and a peak value of 50 ppm observed in one hookah bar, were considerably higher than EPA's National Ambient Air Quality Standard (NAAQS) for 8 h and approached the 1 h standard of 35 ppm.27 Recent studies have examined exhaled CO in patrons of hookah bars and demonstrated that exposure to CO via inhalation of mainstream and secondhand hookah smoke can result in exhaled CO concentrations that are similar to those observed with cigarette smoke.35 Although symptoms from acute CO poisoning are non-specific, including dizziness, irritability, nausea, vomiting, syncope, and chest pain, prolonged exposure can have dire consequences such as myocardial infarction, cerebral oedema, coma and even death.36 Acute CO poisoning in hookah users has been documented in several case reports, with patients presenting to the emergency department with syncope, confusion, slurred speech, and a serum carboxyhaemoglobin level as high as 30% after hookah use.37–41 Although these studies have not partitioned out the contribution from mainstream versus secondhand hookah smoke, it has been determined that the majority of CO produced by a hookah water pipe stems from the inefficient burning of charcoal, rather than the heating of shisha itself,42 suggesting an inherent danger of hookah smoking, regardless of the composition of shisha.
Although hookah bars in NYC are not allowed to use tobacco-based shisha in hookah water pipes, nicotine was found in each venue with a mean concentration of 4.2 µg/m3. We can think of no alternative explanation for the ambient levels of nicotine found, other than that the nicotine emanated from the smoke generated by the hookah use. Potentially, cigarette smoking by patrons and employees in back rooms may occur, but no cigarette smoking was observed in the main room of the hookah bars surveyed in this study. In addition to its potential for addiction and as a gateway to the use of other tobacco products, nicotine is known to have myriad harmful health consequences, such as teratogenic effects on neurodevelopment,43 ,44 ‘altering the formation, survival, and differentiation of brain cells, eliciting deficits in structure, synaptic function and behavioral performance’,45 and alteration in neurotransmitters,46 as well as being associated with fatal arrhythmias,47 low birth weight from prenatal exposure,48 hearing loss,49 tooth decay50 and hyperactivity.51 ,52
In a typical hookah smoking session, a user inhales as much as 100 L of mainstream smoke53 containing numerous toxicants and carcinogens.5 ,54 ,55 In addition to the large amount of mainstream hookah smoke inhaled during a typical session, the effects of SHS are of particular concern. Although it must be noted that the composition of mainstream and secondhand hookah smoke differs from that produced at the higher temperatures occurring in cigarette smoking, these data strongly suggest that active and passive hookah smokers, including individuals working in such settings, may be at as great or greater risk for tobacco-related adverse health effects than those using or exposed to smoke from cigarettes.
Limitations in the present study must be considered in applying the results broadly to other hookah venues and cities. The selection of the eight NYC hookah bars was not random as we assessed ones that were popular among young urbanites based on ratings on two internet sites. Moreover, the measurements were performed on nights with the greatest occupancy. Although the sample size of this study was sufficient to demonstrate that air quality in the selected hookah bars was hazardous to health, one should use caution in generalising this finding to all the hookah venues in NYC, where over 100 such venues exist, or other cities. Additional potential factors that may have affected the observed variability among hookah bars’ indoor air quality include the number of open windows and doors, the size of the venues, air handling and the number of active hookah water pipes and smokers. Interestingly, so-called ‘smoke-eaters’, which are commonly used to remove smoke, were not observed at any of the hookah bars. Although the present study extended basic measurements of PM and CO to OC/EC, nicotine and trace elements, it was limited in the amount of sampling equipment that could be carried unannounced into hookah bars. Important toxic and carcinogenic components of tobacco smoking, such as polynuclear aromatic hydrocarbons and 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol, should be assessed in future studies.
The findings of this study provide evidence that hookah bars in NYC serve tobacco-based shisha in hookahs and generate levels of SHS potentially hazardous to the health of patrons and employees. This information is critical to informing tobacco control policies and regulations for SHS generated from hookahs—perhaps the most rapidly adopted alternative tobacco products in the USA. These findings raise profoundly important and difficult public health policy questions, such as how one would obtain a random sample of sufficient size in NYC and elsewhere to make generic decisions about regulating hookah bars locally or nationally. That is, what public policies could be created and put into place to monitor hookah lounges in an ongoing fashion? In addition, there is a clear need to extend research to focus not only on the indoor air quality of public hookah bars, but also the toxicant exposure and health effects of home hookah users and those who reside with them. Moreover, there is a need to investigate whether non-tobacco based shishas, similar to tobacco-based product, present a major public health hazard, which would then lead to policy debates about how municipalities, states and the federal government would regulate the use of these forms of shisha.
What this paper adds
This is the first study to show that many hookah bars in New York City (NYC) serve tobacco-based shisha.
NYC hookah bars contain concentrations of indoor air pollutants and toxicants that may present a significant health threat to visitors and employees.
There is an urgent need for better air quality monitoring and tobacco control policies in hookah bars.
Acknowledgments
The authors would like to thank Dr George Thurston for the use of sampling equipment.
References
Footnotes
Contributors SZ and TG were integral from the conceptualisation, design and execution of the study. Ms Zhou drafted the initial manuscript and submitted the study. MW, RV, JW, NL, ES, MT, L-CC, and RP all had substantial contribution to all stages of this study, especially in collecting and analysing data. They also helped draft the initial manuscript, interpreted results, critically reviewed and revised the manuscript and approved the final manuscript as submitted.
Funding This work was supported by NIEHS Center of Excellence grant number ES000260, and NCI grant number 3 P30 CA016087-33S1.
Competing interests None
Provenance and peer review Not commissioned; externally peer reviewed.