Article Text

Abstract
Cigarettes with lower machine measured “tar” and nicotine yields have been marketed as “safer” than high tar products over the last four decades, but there is conflicting evidence about the impact of these products on the disease burden caused by smoking. This paper critically examines the epidemiological evidence relevant to the health consequences of “reduced yield” cigarettes. Some epidemiological studies have found attenuated risk of lung cancer but not other diseases, among people who smoke “reduced yield” cigarettes compared to smokers of unfiltered, high yield products. These studies probably overestimate the magnitude of any association with lung cancer by over adjusting for the number of cigarettes smoked per day (one aspect of compensatory smoking), and by not fully considering other differences between smokers of “high yield” and “low yield” cigarettes. Selected cohort studies in the USA and UK show that lung cancer risk continued to increase among older smokers from the 1950s to the 1980s, despite the widespread adoption of lower yield cigarettes. The change to filter tip products did not prevent a progressive increase in lung cancer risk among male smokers who began smoking during and after the second world war compared to the first world war era smokers. National trends in vital statistics data show declining lung cancer death rates in young adults, especially males, in many countries, but the extent to which this is attributable to “reduced yield” cigarettes remains unclear. No studies have adequately assessed whether health claims used to market “reduced yield” cigarettes delay cessation among smokers who might otherwise quit, or increase initiation among non-smokers. There is no convincing evidence that past changes in cigarette design have resulted in an important health benefit to either smokers or the whole population. Tobacco control policies should not allow changes in cigarette design to subvert or distract from interventions proven to reduce the prevalence, intensity, and duration of smoking.
- tar and nicotine
- lung cancer
- changing cigarette
Statistics from Altmetric.com
Cigarettes with lower machine measured “tar” and nicotine yields have been marketed as “safer” than high tar products over the last four decades,1 2 but there is limited and conflicting evidence about the net impact of these products on the disease burden caused by smoking. The principal uncertainties are the extent to which compensatory smoking behaviours induced by “reduced yield” cigarettes may offset any putative reductions in the toxicity or carcinogenicity of these products, and whether health claims used to promote “Light” cigarettes may delay cessation among smokers who might otherwise quit, or increase initiation among non-smokers. Epidemiological studies have generally focused narrowly on the intrinsic toxicity and carcinogenicity of “reduced yield” products, rather than on their indirect effects on smoking behaviour or the number of people smoking.
This paper critically examines the epidemiological evidence relevant to the health consequences of “reduced yield” cigarettes. It begins by briefly reviewing the historical development of products with lower tar and nicotine yields, as measured by the standard Federal Trade Commission (FTC) protocol of machine smoking.3 It then considers the evidence that smokers “compensate” for reductions in machine measured tar and nicotine by increasing the number of cigarettes smoked per day as well as by increasing the puff volume and number of puffs per cigarette. It discusses the strengths and limitations of several epidemiological approaches that have been used to assess the health effects of “reduced yield” cigarettes. These include analytic (cohort and case–control) studies that compare the risks to smokers who use different types of cigarettes; selected cohort studies that illustrate how the lung cancer risk to smokers has increased over time; and analyses of trends in national death rates from lung cancer by age in relation to age specific smoking patterns.
Historical development of “less hazardous” cigarettes
The postulate that cigarettes with lower tar delivery might be less hazardous emerged from the early research findings on tobacco related diseases. Epidemiological studies repeatedly demonstrated increased lung cancer risk in smokers beginning in the 1950s4-7; experiments showed that painting cigarette smoke condensate on the backs of mice produced skin tumours.8 By 1967, independent scientists and public health authorities recommended to the US Congress that cigarettes with lower particulate yield be developed and marketed to smokers who could not quit.9
The tobacco industry responded to health concerns about cigarette use first by adding filters to some brands of cigarettes beginning in the 1950s, and then by offering cigarettes that delivered progressively less “tar” as measured by machine smoking.3 10 Much of the reduction in “tar” (total particulate matter minus nicotine and water) was achieved by the addition of ventilation holes around the filter to dilute the smoke with entrained air. A method of machine smoking that was developed in the 1930s11 became codified in the Federal Trade Commission (FTC) annual ratings of cigarettes.3 This protocol specifies fixed smoking parameters for the machine: 35 ml puff volume, 2 second puff duration, 1 puff per minute frequency, and a fixed butt length to which the cigarette is smoked.12 Brands that yield approximately 1–6 mg of tar per cigarette by the FTC method are referred to as “Ultralight”; those with approximately 7–15 mg tar as “Light”, and those yielding more than 15 mg tar as “Regular” or “Full flavoured”.13 Before the mid 1950s, unfiltered cigarettes typically yielded 25–30 mg tar by the FTC method.
The FTC ratings do not take into account variations in tar and nicotine yield that can be obtained by smokers seeking to maintain a particular intake of nicotine.3 14-16 Smokers who use “reduced yield” products can increase the amount of nicotine and tar extracted from each cigarette by taking more puffs per cigarette, obstructing the ventilation holes around the filter, and inhaling a larger puff volume more deeply into the lungs.17 Smokers can also compensate for reduced yield by smoking more cigarettes per day.17Internal documents from the tobacco industry express scepticism about the efficacy of filter tip and “lower yield” products in reducing the exposure of smokers, even during the years when these products were first heavily marketed to assuage the health concerns of smokers.1 2 A memo from Helmut Wakeham of Philip Morris (dated 24 March 1961) states, “As we know, all too often the smoker who switches to a hi-fi cigarette winds up smoking more units in order to provide himself with the same delivery which he had before”.18
Compensatory smoking
Many experimental studies document that smokers who are switched to cigarettes with lower nicotine yield than their usual brand are able to maintain higher plasma concentrations of nicotine metabolites than would be expected from the FTC ratings. Compensation has been demonstrated experimentally in both short term19-23 and long term studies.24-29 What is less certain is the extent to which smokers compensate by increasing the number of cigarettes smoked per day as opposed to other behavioural changes that extract more nicotine from each cigarette. This distinction is important with respect to the epidemiological studies, since most of these studies adjust for the number of “reduced yield” cigarettes smoked per day, and may thereby over-control for one aspect of compensatory smoking.30
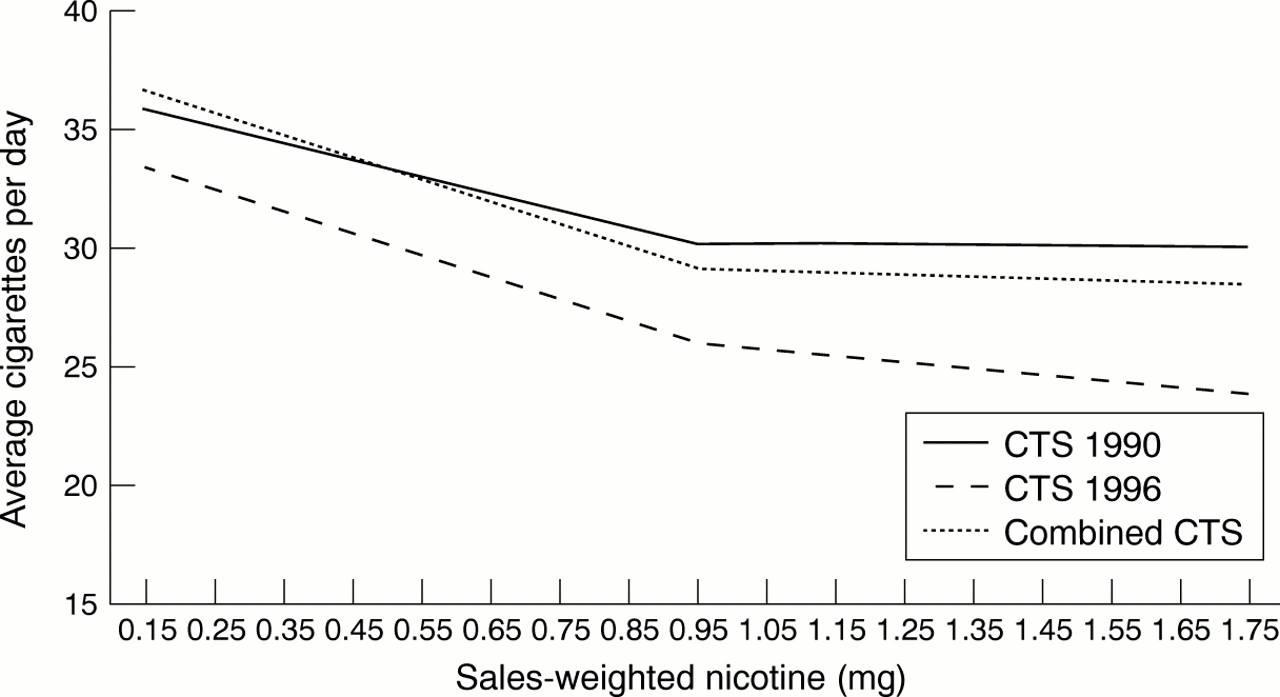
We assessed the relation between daily cigarette consumption and the FTC rating of nicotine yield in several additional large studies, the American Cancer Society Cancer Prevention Study I (CPS-I) cohort, and the 1990 and 1996 California Tobacco Surveys (CTS).30 In the CPS-I cohort, questionnaires were administered periodically during the follow up to document changes in smoking behaviour or cigarette brand. Based on these data, fig 1 shows the mean change in cigarettes smoked per day in relation to the change in nicotine yield among 169 610 white male smokers who changed brands between enrollment in 1959 and the end of follow up in 1972.27 Each milligram decrease in machine measured tar yield was associated, on average, with an increase of 2.31 cigarettes smoked per day. This prospective analysis controlled for age, cigarettes smoked per day before the switch, and tar and nicotine yields of the cigarette smoked before the switch. A similar relation was seen in the 1990 and 1996 CTS for cigarette brands with less than 0.95 mg nicotine yield (fig 2). This analysis was restricted to adult smokers, age 25–64 years, who smoked at least five cigarettes daily during the year before the survey and had not attempted to quit smoking in the previous 12 months. The intent was to limit these analyses to persons with relatively stable smoking patterns31 32 and less likelihood of having changed their smoking because of illness. These studies suggest a small but demonstrable increase in the number of cigarettes smoked per day among smokers of lower yield cigarettes. Previous reports14 28 29 33 34 have been less consistent, perhaps because of smaller sample sizes and the inclusion of people with less stable smoking patterns.
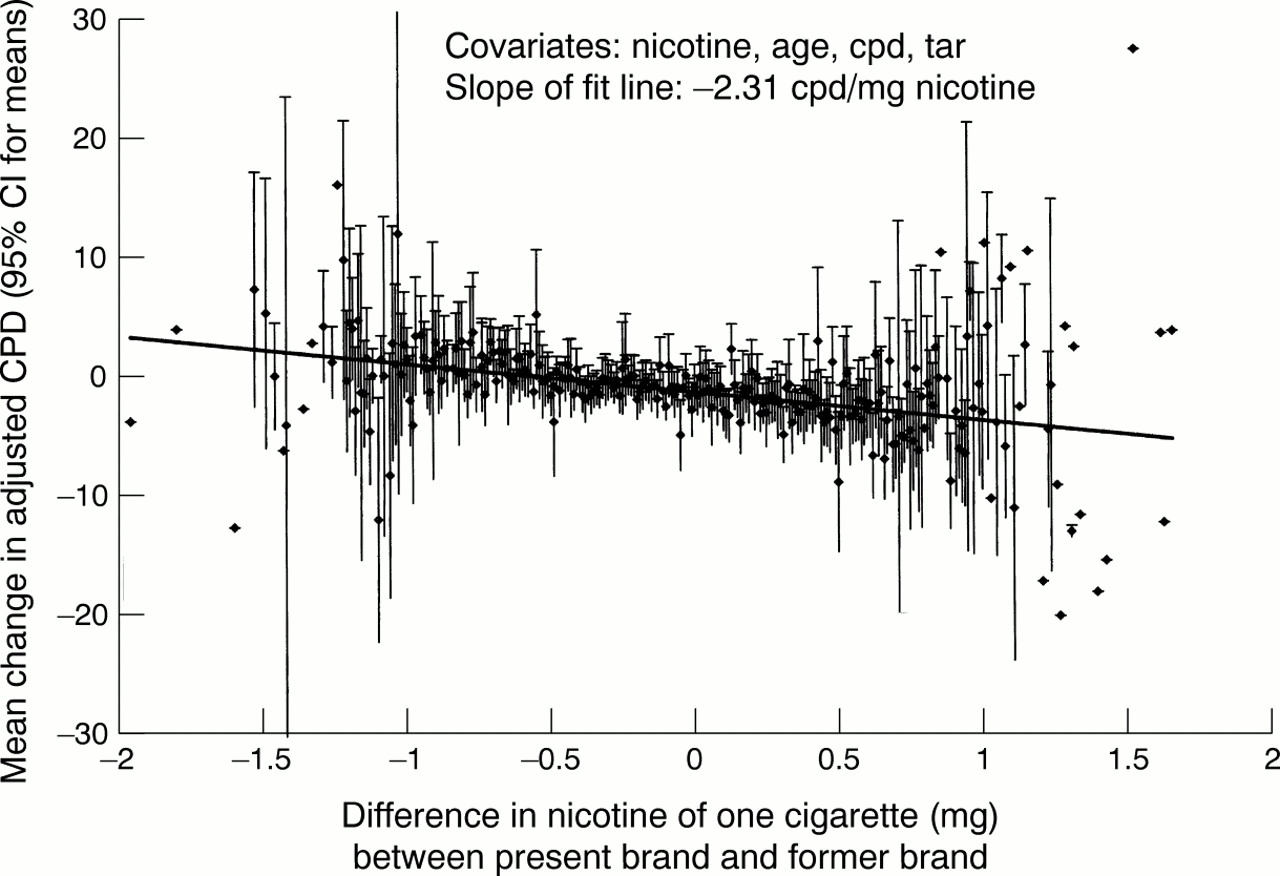
Mean change in adjusted cigarettes smoked per day (CPD) reported for subjects changing brand smoked versus change in machine measured nicotine yield per cigarette: white male smokers (n = 169610), American Cancer Society Cancer Prevention Study I (CPS-I) study, followed 1960 to 1972. Each milligram decrease in machine measured tar yield among CPS-I smokers who changed brands between enrollment in 1959 and end of follow up in 1972 was associated with an increase of 2.31 cigarettes smoked per day. Based on 169610 white male smokers.30

Piecewise linear regression of cigarettes smoked per day by sales-weighted nicotine yield of the brand smoked (California data), illustrating the inverse relation between cigarettes smoked per day and machine measured tar yield below approximately 1 mg. Based on the 1990 and 1996 California Tobacco Surveys.30
Epidemiological studies
COHORT AND CASE–CONTROL STUDIES COMPARING DIFFERENT TYPES OF CIGARETTES
Over 50 epidemiological studies have compared disease risks among smokers who use different types of cigarettes.35-89 These studies, discussed elsewhere,30 typically measure the occurrence of lung cancer,35-78 coronary heart disease,39-42 44 45 51 56 64 67 79-82 and respiratory diseases caused by smoking39 42 45 67 83-89 in smokers who use filter tip products compared to those who use unfiltered, “high yield” products. Most of these studies report lower lung cancer risk among smokers who use “reduced yield” products, relative to those who smoke unfiltered, “higher yield” cigarettes. They do not consistently report lower risk of coronary heart disease, total stroke, or chronic obstructive pulmonary disease (COPD).
The studies that compare different types of cigarettes have at least two limitations that complicate their interpretation. First, they focus mostly on differences in the intrinsic pathogenicity of “reduced yield” cigarettes compared to unfiltered, higher yield products without adequately considering the indirect adverse effects that lower yield cigarettes may have on smoking behaviour. For example, the studies compare risk among smokers who use different types of cigarettes but do not assess whether some smokers have deferred quitting because of health claims about “reduced yield” products. Lung cancer risk increases exponentially with longer duration of smoking.90 Factors that delay cessation may outweigh any putative reductions in tar yield, increasing rather than decreasing the lung cancer risk for an individual smoker. Furthermore, health claims used to market “Light” cigarettes could worsen the population burden of disease by trivialising the actual hazards of smoking, thus promoting initiation or resumption of smoking.1 2
Secondly, the published cohort and case–control studies may overestimate the magnitude of any attenuation in lung cancer risk by inappropriately controlling for the number of cigarettes smoked per day and by under controlling for other factors that could reduce risk. In adjusting for the number of cigarettes smoked per day, the epidemiological studies assume that smokers who switch to “reduced yield” cigarettes do not compensate for the lower yield by increasing their daily cigarette consumption. Some adjustment for cigarettes per day is needed to assess the intrinsic carcinogenicity of the cigarette, but this adjustment is inappropriate if it obscures an adverse effect of compensatory smoking. Furthermore, smokers who are able to switch to cigarette brands with lower nicotine yield “reduced yield” products may have other characteristics that attenuate their lung cancer risk, relative to smokers who cannot switch. Their change in brands may reflect comparatively less dependence on nicotine and other addictive components of smoking. Smokers who switch may have smoked less intensively in the past and be more likely to quit during the follow up. Epidemiological studies have not historically measured nicotine addiction or related parameters such as puff volume, puffs per cigarette, or depth of inhalation. Prospective studies that have assessed smoking behaviour only at the time of enrolment cannot control for differences in cessation rates during follow up. Thus, the relatively lower risk of lung cancer among smokers who switch may result, not from switching per se, but rather from behavioural differences related to addiction. Some or all of what has been interpreted as efficacy may actually reflect selection bias or residual confounding.
COHORT STUDIES OF LUNG CANCER RISK IN DIFFERENT GENERATIONS OF SMOKERS
Several major cohort studies of smoking and disease have bridged the period when the greatest reduction occurred in the tar ratings of cigarettes. The British Doctors' Study examined lung cancer rates in relation to smoking behaviour among British physicians over a 40 year period.91 Age standardised incidence rates among smokers were compared between the intervals 1951–1971 and 1971–1991. A similar comparison was made in the USA where the American Cancer Society (ACS) conducted two large cohort studies of comparable design begun 23 years apart: Cancer Prevention Study I (CPS-I), begun in 1959, and CPS-II, begun in 1982.92 93
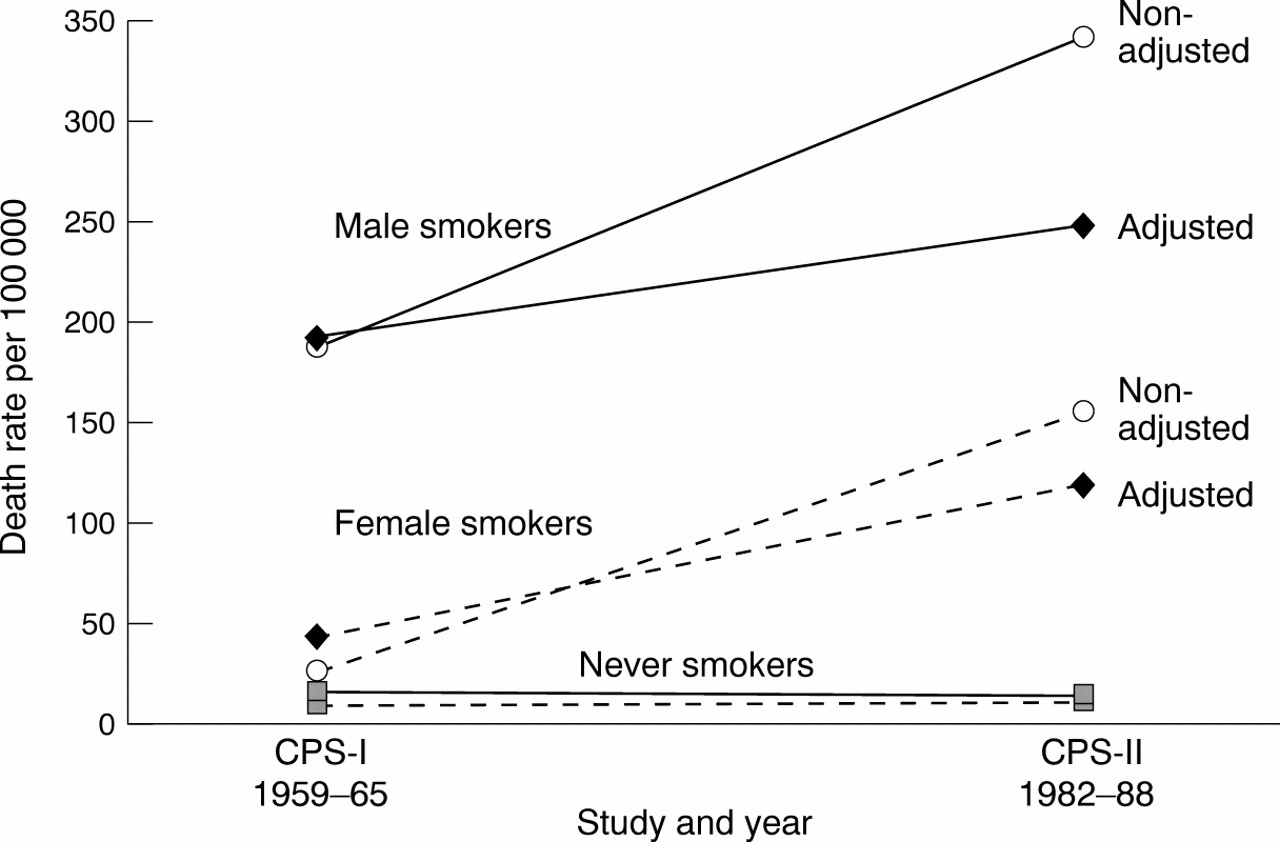
In both the British Doctors' Study91 94 and the two ACS cohorts92 93 lung cancer risk increased among smokers from the 1950s to the 1980s. This increase occurred despite a dramatic decrease in the machine measured tar level of cigarettes in both countries during this time period.94 Among the British doctors, the age standardised lung cancer incidence increased by 19%, from 264 per 100 000 to 314 per 100 000 from the first to the second 20 year period.94 In the ACS studies, an even larger increase occurred in the age standardised lung cancer death rate among both male and female smokers from CPS-I to CPS-II, while this rate remained essentially constant in lifelong non-smokers (fig3).95 The age standardised rate increased from 187 to 341 (deaths per 100 000 person years) among male current cigarette smokers and from 26 to 155 among female smokers from CPS-I to CPS-II. The slope of the increase was reduced, but not eliminated, when the rates were adjusted for differences in the number of cigarettes smoked per day and duration of smoking, as reported at the time of enrolment. The ACS analyses are restricted to the first six years of follow up to enhance comparability.

Death rates from all lung cancers by smoking status, CPS-I and CPS-II (adjusted for current amount and duration of smoking). The “non-adjusted” points indicate the age standardised death rate from lung cancer among male and female current cigarette smokers and lifelong non-smokers in CPS-I (1959–1965) and CPS-II (1982–1988). The “adjusted” values signify the results adjusted for age, cigarettes smoked per day, and years of smoking as reported at enrolment into the study.
These cohort studies indicate that the absolute risk of lung cancer continued to increase rather than decrease among older smokers despite the widespread adoption of “reduced yield” cigarettes. The substitution of filter tip products among smokers in CPS-II, for the unfiltered, very high yield cigarettes used extensively by smokers in CPS-I did not prevent a sustained increase in lung cancer among female smokers over age 45 and male smokers over age 50. Only among younger male smokers, ages 40–45, were lung cancer death rates lower in CPS-II than in CPS-I.95 These studies help to put into perspective the relative attenuation in lung cancer risk seen in the earlier cohort and case–control studies that compare one type of cigarette to another. Whatever the relative impact of “reduced yield” products, their absolute impact was clearly inadequate to prevent a major increase in lung cancer risk among older smokers.
There are at least three possible explanations why lung cancer risk increased among smokers despite a dramatic decline in the machine measure tar yield of the cigarettes being smoked. One is that smokers who became addicted during and after the first world war presumably smoked less intensively as adolescents and young adults than did smokers who initiated smoking during and shortly after the second world war.94 95 Manufactured cigarettes were less available and relatively more expensive after the first than the second world war. Consequently, earlier generations of smokers who consumed predominantly unfiltered, high yield products may have been spared the full consequences of early life smoking that affected later generations. While the CPS-I and CPS-II analyses adjusted for the usual number of cigarettes smoked per day, as reported at the time of enrolment into the studies, this might not reflect large differences in early life smoking. Adverse changes in smoking behaviour may have overwhelmed any putative change in tar yield.
Two alternative explanations for the higher lung cancer risk among smokers in the second world war, compared to the first world war generation, involve a shift in the demographics of smokers and/or an increase, rather than decrease in the carcinogenicity of “reduced yield” cigarettes. Contemporary smokers are less educated and affluent, and have less healthy dietary patterns than previous generations of cigarette smokers.96-99 Persons who continue to smoke despite repeated health warnings may also be more addicted and smoke more intensively.95 Neither of these explanations would suggest that design changes in contemporary cigarettes have compensated adequately for the increased vulnerability of smokers or for adverse changes in smoking behaviour.
National trends in lung cancer mortality at specific ages
Several analyses100-102 have examined trends in national lung cancer death rates by age in relation to age specific smoking patterns. Studies based on national trends are called “ecological” because they lack data on individual behaviours and outcomes, and cannot separate disease occurrence in current smokers from events in former or never smokers. However, the trends in national rates do reflect accurately the extent of progress towards reducing disease occurrence in the overall population.
One approach is to compare the trend in lung cancer death rates for a particular age group with the trends in smoking prevalence at younger ages. This approach does not integrate all of the relevant parameters of smoking behaviour, nor does it consider the time lag that occurs between the initiation of smoking and the onset of lung cancer, but it does allow a visual comparison of trends in age specific prevalence with trends in lung cancer in adjoining birth cohorts. Figure 4 shows the trends in lung cancer death rates for men and women, ages 35–39 in the USA and UK between 1965 and 1997, compared to the trend in cigarette smoking prevalence at ages 25–34 over the same time period. Among US men, the decrease in lung cancer mortality essentially parallels the decrease in cigarette smoking prevalence (fig 4A), whereas for men in the UK, the proportionate decrease in lung cancer mortality is much steeper than the decrease in smoking prevalence (fig4B). Among US women, the lung cancer death at ages 35–39 changed very little over this time period despite a 40% decline in smoking prevalence (fig 4C). Among women of corresponding ages in the UK, both lung cancer and smoking prevalence decreased by 38% over the interval (fig 4D). The temporal trends in lung cancer mortality in women are more difficult to interpret than those in men, because of the much larger recent changes in the ages when women initiated smoking and increases in the intensity of adolescent smoking.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Lung cancer death rates at ages 35–39 and cigarette smoking prevalence at ages 25–34. The graphs indicate the temporal trend in lung cancer death rates at ages 35–39 and in cigarette smoking prevalence at ages 25–34 among men in the USA (A) and UK (B) and among women in the USA (C) and UK (D).
Reductions in the tar yield of cigarettes are one possible explanation for the very rapid decline in lung cancer death rates at younger ages among men in the UK94 and the more gradual decreases elsewhere in Europe, North America, and Australia100 in recent decades. However, design changes in cigarettes are not the only potential explanation. The particularly high rates of lung cancer that prevailed among men in the UK until the 1950s and that are seen presently in some Eastern European countries may also reflect the exacerbating effects of diet, or reductions in occupational exposures or air pollution from coal burning that could potentiate the risks from smoking. Other potentially important parameters that have not been directly considered in these temporal and geographic comparisons include differences in cigarette composition across countries, and variations in the age of initiation, intensity of smoking at various ages, and age at cessation, both within and across countries. Thus, the analyses based only on national trends cannot convincingly separate the contribution of “reduced yield” cigarettes from other factors that might affect lung cancer risk.
Furthermore, it should be noted that, while the decline in lung cancer death rates at younger ages is encouraging, there is no certainty that these trends will be sustained into the future. Recent vital statistics data suggest that reductions in lung cancer death rates among young adults in the USA have slowed and possibly reversed, as a result of adverse changes in smoking behaviour among the young.102To the extent that health claims about “reduced yield” cigarettes defer cessation, this could also interfere with the progression of favourable trends into older ages where most lung cancers occur.
Other comprehensive reviews
Recent reviews by the Institute of Medicine1 and the National Cancer Institute2 have examined the evidence for a reduction in disease risks associated with the use of low yield cigarettes. Their conclusions reinforce the cautions raised by the UK Royal College of Physicians.103 The Institute of Medicine report on The scientific base for tobacco harm reduction stated: “There have been many efforts in the past to develop less harmful cigarettes, none of which has proved to be successful.”1 The National Cancer Institute review concluded: “Epidemiological and other scientific evidence, including patterns of mortality from smoking caused diseases, does not indicate a benefit to public health from changes in cigarette design and manufacturing over the last 50 years.”2
Conclusions
In summary, there is no convincing evidence that changes in cigarette design between the 1950s and the mid 1980s have resulted in an important decrease in the disease burden caused by cigarette use for either smokers as a group or for the whole population. While many epidemiological studies have found attenuated risk of lung cancer among people who smoke these products, the extent to which these studies may overestimate the magnitude of the lung cancer association remains unclear. No studies have adequately assessed whether health claims used to market “reduced yield” products delay cessation among smokers who might otherwise quit or increase initiation or relapse among non-smokers. The widespread shift from unfiltered, high yield cigarettes to filter tip, lower yield products that occurred in the USA and UK since the 1950s did not prevent continuing increases in lung cancer risk among older smokers in large cohort studies. While one can postulate that lung cancer rates among older smokers might have risen even further in the absence of “reduced yield” cigarettes, other explanations are also possible. The temporal decrease in lung cancer risk at younger ages has been encouraging, but may be short lived if health claims about lower yield cigarettes are allowed to discourage or delay genuine cessation efforts by smokers. Furthermore, the extent to which changes in age specific lung cancer death rates reflect modifications in cigarette design versus changes in smoking behaviour including initiation and cessation has yet to be proven. There is no consistent evidence that “reduced yield” cigarettes have attenuated the risk of other smoking attributable diseases besides lung cancer.
A central challenge in tobacco policy is to prevent the misuse of unproven health claims to promote novel products. Alternative nicotine delivery devices may ultimately help to mitigate the harm caused by smoking to the approximately 47 million Americans who continue to smoke.1 However, the evidence base required to market these products should correspond to the evidence required for any new drug delivery device. Furthermore, the publicity and marketing of these products must not distract attention away from interventions proven to reduce the prevalence, intensity, and duration of smoking.
Acknowledgments
This paper summarises material from a chapter on disease risks associated with light cigarettes from the upcoming National Cancer Institute Monograph 13: Risks associated with smoking cigarettes with low machine-measured yields of tar and nicotine.30 The authors wish to thank the many colleagues who contributed to our thinking on this topic, including Sir Richard Peto, Drs Gary Giovino, Theodore Holford, Scott Leischow, Jay Lubin, Jonathan Samet, and Robert Tarone. We thank Michael Pleasant for preparation of the manuscript.
Source of support: American Cancer Society and University of California Tobacco-Related Disease Research Program; grant 8RT-0094.
References
Supplementary materials
- Authors' correction
Readers should please note that the legend to Figure 1 and the text in the sixth line of the second paragraph of the section headed 'Compensatory smoking' should say, "Each milligram decrease in machine-measured nicotine .." rather than "Each milligram decrease in machine-measured tar..."