Article Text

Abstract
Objective: To assess the pharmacy profession’s perceptions of tobacco sales in US pharmacies and explore whether a policy prohibiting sales of tobacco in pharmacies would alter adult consumer shopping behaviour.
Subjects and design: In California, surveys were administered to 1168 licensed pharmacists and 1518 pharmacy students, and telephone interviews were conducted with 988 adult consumers.
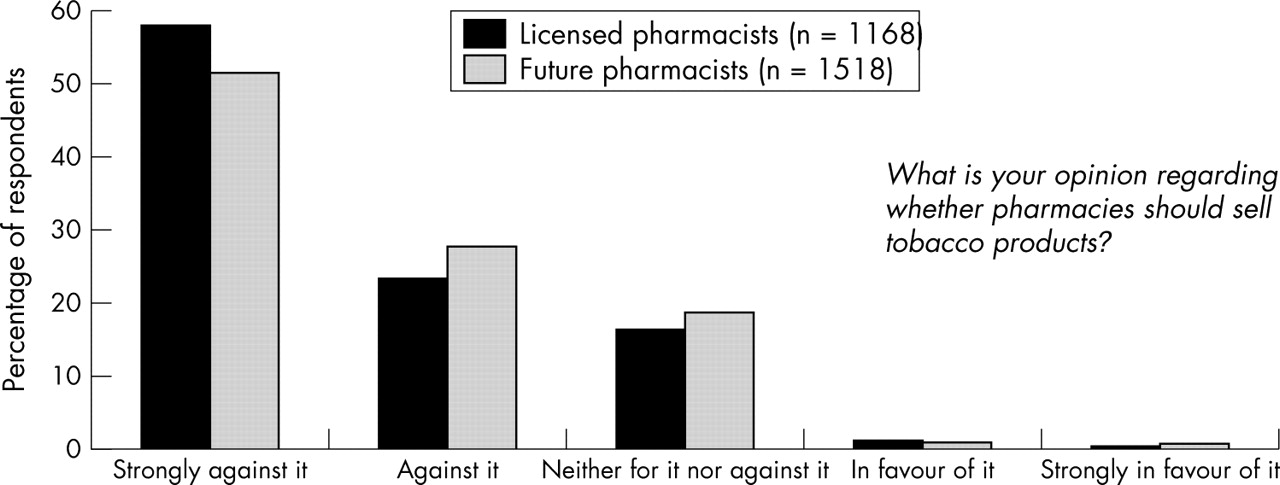
Results: Most (58.1%) licensed pharmacists were strongly against sales of tobacco in pharmacies, 23.6% were against it, 16.7% were neutral, 1.2% were in favour of it, and 0.4% were strongly in favour of it. Pharmacists who were current tobacco users were more likely to be in favour of tobacco sales in pharmacies than were pharmacists who were current non-users (p < 0.005). Similar statistics were observed for pharmacy students. Most consumers (72.3%) disagreed with the statement, “I am in favour of tobacco products being sold in drugstores”; 82.6% stated that if the drugstore where they most commonly shopped were to stop selling tobacco products, they would shop there just as often, 14.2% would shop there more often, and 3.2% would shop there less often.
Conclusion: Little professional or public support exists for tobacco sales in pharmacies.
- health professional
- pharmacist
- pharmacy
- tobacco sales
Statistics from Altmetric.com
According to the World Health Organization, approximately five million premature deaths are attributable to tobacco each year.1 In the USA, cigarette smoking is the primary known preventable cause of death,2 resulting in an estimated 437 932 deaths3 and $157 billion in health related losses annually.4 Each of approximately 22 billion packs of cigarettes sold in the USA in 1999 cost society $3.45 in medical care related to smoking and $3.73 in lost productivity, for a total of $7.18 per pack.4 Despite the known negative health consequences of smoking, in 2003 the tobacco industry spent $15.15 billion toward the advertising of cigarettes in the USA,5 and in 2004 an estimated 20.9% of adult Americans were current smokers.6
Health care providers have a professional obligation to promote the health of their patients. While most health professions have adopted “tobacco-free” policies such as prohibiting the sale of tobacco in hospitals and outpatient facilities, many community pharmacies in the USA continue to sell tobacco products despite numerous resolutions and recommendations set forth by pharmacy organisations over the past three decades.7 In 1970, the American Pharmaceutical Association (APhA) stated that mass display of cigarettes in pharmacies is in direct contradiction to the role of the pharmacy as a public health facility.
In 1971, the APhA House of Delegates passed a series of recommendations regarding the dangers of cigarette smoking—the first recommendation was that tobacco products not be sold in pharmacies. In 1973 and again in 1977, the California Pharmacists Association adopted the following recommendation: pharmacists, in the interest of raising the standards for public health and social welfare in the community, shall discourage the sale of tobacco products in the pharmacies in which they practice. While professional pharmacy organisations have been advocating tobacco-free policies for the past 35 years, these recommendations have been largely ignored in the community pharmacy setting. Schroeder and Showstack determined that 93% of non-clinically affiliated pharmacies in San Francisco sold cigarettes in 1976.8 This study was replicated in 20039 and demonstrated significant change among independently owned pharmacies (a reduction from 90.6% to 24.1%), but little change among retail chain pharmacies (100% to 93.8%). In 2003, chain pharmacies accounted for 52% of all pharmacies in the USA.10
Tobacco is the only consumable product that when used as intended will kill at least half of its users.11 As such, tobacco sales through pharmacies directly contradicts the pharmacist’s code of ethics, which states that pharmacists must be committed to the welfare of their patients and must act with honesty and integrity in professional relationships, avoiding actions that compromise dedication to the best interests of their patients.12 Here we describe licensed pharmacists’, future pharmacists’, and adult consumers’ perceptions of tobacco sales in pharmacies in the state of California.
METHODS
The data presented here derive from a series of three studies conducted in California: (1) a survey of 1168 licensed pharmacists; (2) surveys of 1518 pharmacy students, and (3) telephone interviews with 988 adult consumers. Below, the methodology underlying each of these studies is summarised.
Study 1: licensed pharmacists’ opinions about tobacco sales in pharmacies
Questionnaires were distributed in 1999–2000 by mail to all licensed pharmacists in four counties in Northern California: Alameda, Merced, San Francisco, and San Mateo.13 Respondents (n = 1168, 54% response) completed a 10 page questionnaire that assessed factors relevant to tobacco cessation counselling activities. Data reported here include sociodemographics (sex, age, and race/ethnicity), self reported tobacco use status (dichotomised as current user or current non-user), and opinions about tobacco sales in pharmacies. This was assessed by asking, “What is your opinion regarding whether pharmacies should sell tobacco products?” Response options and corresponding codings included “I am strongly against it” (coded 1), “I am against it” (coded 2), “I am neither for it nor against it” (coded 3), “I am in favour of it” (coded 4), and “I am strongly in favour of it” (coded 5). Finally, we assessed pharmacists’ opinions about the profession’s role in (a) preventing the initiation of tobacco use and (b) promoting tobacco cessation.
Study 2: future pharmacists’ opinions about tobacco sales in pharmacies
Measures parallel to those described for study 1 were collected from 1518 pharmacy students over a period of three years (2000, 2001, and 2002) at the then four schools of pharmacy in California (University of California San Francisco, University of the Pacific, University of Southern California, and Western University), and at the newly established University of California San Diego school of pharmacy in January 2003. These items were embedded within a programme evaluation questionnaire and administered following exposure to the Rx for Change: Clinician-Assisted Tobacco Cessation curriculum,14–16 which has been required training (7–8 hours) for all pharmacy students in California since 2000. The response rate for this survey is estimated as at least 88%, based on the number of students enrolled in the course.
Study 3: adult consumers’ opinions about tobacco sales in pharmacies
Using random digit dialling, 988 telephone interviews (69.4% response) were conducted in 2000 with adult residents in six California counties: San Diego, San Joaquin, Orange, Sonoma, San Mateo, and San Luis Obispo. In addition to sociodemographic questions (sex, age, race/ethnicity, highest level of education, employment, and tobacco use status), respondents were asked to specify the extent to which they agreed with the statement “I am in favour of tobacco products being sold in drugstores.” Response options included, “strongly agree”, “agree”, “disagree”, and “strongly disagree”. Participants also were asked: (a) “If you had the choice to shop at a drugstore that carried tobacco products or one that did not carry tobacco products, would you…‘choose the one that carried tobacco products’, ‘choose the one that did not carry tobacco products’, or ‘it would not affect your choice’”; (b) “If your drugstore stopped selling tobacco products, would you shop there ‘more’, ‘less’, or ‘the same’?”, and (c) “How often do you buy tobacco products at a chain drugstore?” Response options for this latter question included “always”, “sometimes (occasionally)”, “rarely”, and “never”.
Analysis
For all three studies, standard descriptive statistics were used to characterise the study population and responses to survey items. T tests and χ2 tests were used, as appropriate, to assess relationships between study variables.
RESULTS
Study populations
Table 1 delineates the sociodemographic characteristics of the study participants. The licensed and future pharmacist populations were primarily Asian or Pacific Islander, and the adult consumer population was primarily white. Approximately half (50.6%) of consumers were employed for wages, 14.0% were self employed, 18.3% were retired, 6.2% were homemakers, 5.2% were students, 3.0% were unemployed, and 2.7% were unable to work. The education level of consumers was distributed as follows: less than a high school graduate, 5.2%; high school graduate or equivalent, 18.8%; technical school, 2.6%; some college, 32.3%; and college graduate, 41.1%.
Characteristics of licensed pharmacists (n = 1168), future pharmacists (n = 1518), and California consumers (n = 988)
Study 1: licensed pharmacists’ opinions about tobacco sales in pharmacies
Of 1168 licensed pharmacists surveyed, 1.6% were either in favour (1.2%) or strongly in favour (0.4%) of tobacco sales in pharmacies (fig 1). These perceptions differed by tobacco use status (p < 0.001), with the average opinion score for the 40 (3.5%) licensed pharmacists who were current tobacco users being 2.08, compared to 1.61 for current non-users of tobacco (possible range, 1 = strongly against tobacco sales in pharmacies to 5 = strongly in favour of tobacco sales in pharmacies). Overall, 7.5% of current tobacco users and 1.4% of current non-users were in favour of tobacco sales in pharmacies (χ21df = 8.77, p < 0.005). Approximately 82.3% of respondents believed that the pharmacy profession should be more active in preventing onset of tobacco use, and 86.4% believed it should be more active in promoting tobacco cessation; these perceptions did not differ based on opinions about tobacco sales in pharmacies. Current tobacco users (n = 40) were less likely than were non-users to believe that the professions should be more active in promoting cessation (75.0% v 86.8%; χ21df = 4.61, p < 0.05). Perceptions about the profession’s role in preventing the initiation of tobacco use did not differ by smoking status.

{kind=link}
Licensed and future pharmacists’ opinions about sales of tobacco products in pharmacies.
Study 2: future pharmacists’ opinions about tobacco sales in pharmacies
Of 1518 future pharmacists surveyed, 2.0% were either in favour (1.1%) or strongly in favour (0.9%) of tobacco sales in pharmacies (fig 1). Average opinion scores for the 114 (7.7%) pharmacy students who were current tobacco users was 2.18, compared to 1.68 for current non-users of tobacco (p < 0.001). Overall, 5.3% of current tobacco users and 1.6% of current non-users were in favour of tobacco sales in pharmacies (χ21df = 7.52, p < 0.01). Approximately 86.4% of students believed that the pharmacy profession should be more active in preventing onset of tobacco use, and 93.5% believed it should be more active in promoting tobacco cessation. These perceptions did not differ based on opinions about tobacco sales in pharmacies but did differ based on tobacco use status, with current tobacco users being less likely than current non-users to believe that the professions should be more active in preventing the initiation of tobacco use (74.1% v 87.5%; χ21df = 15.83, p < 0.001) and in promoting cessation (81.3% v 94.6%; χ21df = 30.28, p < 0.001).
Study 3: adult consumers’ opinions about tobacco sales in pharmacies
Nearly three quarters of 988 adult consumers either disagreed (39.5%) or strongly disagreed (32.8%) with the statement “I am in favour of tobacco products being sold in drugstores”; 2.7% strongly agreed, and 24.9% agreed. In choosing a drugstore, 25.4% would choose to shop at a drugstore that did not carry tobacco products, 3.2% would choose a drugstore that did carry tobacco products, and 71.4% indicated that sales of tobacco products would not affect their choice. When asked, “If your drugstore stopped selling tobacco products, would you shop there more, less, or the same?”, 82.6% stated that if the drugstore where they most commonly shopped were to stop selling tobacco products, they would shop there just as often; 14.2% would shop there more if tobacco products were no longer sold; and 3.2% would shop there less. Almost three quarters of 155 self reported tobacco users interviewed either rarely (25.3%) or never (46.8%) bought tobacco at pharmacies; fewer tobacco users indicated they purchased tobacco in pharmacies sometimes (20.1%) or always (7.8%).
DISCUSSION
By selling tobacco products, pharmacies convey tacit approval to their purchase and use; this, in turn, sends a mixed message to consumers, who typically patronise pharmacies to receive health care services. Although the studies described here were conducted in the USA, other countries (for example, Canada17 and Australia18) have similarly encountered this issue. In the USA, several grass roots efforts in recent years have attempted to encourage pharmacies to quit selling tobacco, such as the California Medical Association Foundation’s Prescription for Change project, which successfully enlisted more than 900 tobacco-free pharmacies throughout California and provided an online index to aid consumers and health professionals in identifying tobacco-free pharmacies in their community. Despite this project’s success in engaging segments of the profession and in raising awareness for this issue through edgy, broad scale media campaigns, its efforts to influence the decision makers within chain drugstore management were unsuccessful. While pharmacies that sell tobacco often state that they carry tobacco products as a convenience to customers, our results suggest that most consumers are not in favour of tobacco sales in pharmacies, the majority of tobacco users do not routinely purchase their cigarettes at pharmacies, and if tobacco sales were to cease, the impact on profits is likely to be small. Indeed, a report from the Physicians for a Smoke-Free Canada concluded that despite initial predictions, banning cigarette sales in pharmacies did not result in pharmacy closures in the province of Ontario.17
In addition to lack of support by consumers, our data also indicate that only a small minority (fewer than 2%) of the pharmacy profession in California is in support of tobacco sales in pharmacies. Even among tobacco users, few (7.5% of pharmacists and 5.3% of students) were in favour of tobacco sales in pharmacies. Clearly, there is a logical and ethical disconnect between the sales of tobacco in pharmacies and the pharmacist’s code of ethics.12 As the majority of US schools of pharmacy integrate comprehensive tobacco cessation training through implementation of the Rx for Change: Clinician-Assisted Tobacco Cessation curriculum,14–16 we anticipate that social norms within the profession will change, and pharmacists of the future will be more vocal against tobacco sales in their practice environments. Indeed, exposure to the Rx for Change programme has been demonstrated to strengthen (p < 0.001) California pharmacy students’ opposition toward tobacco sales in pharmacies.16
The prevalence of current tobacco use among California pharmacists is low (3.5%), and this value is similar to that observed (4.5% current smokers) in a recent, national survey of 403 pharmacists.19 Individual smoking behaviour has been shown to be associated with health professionals’ tobacco cessation counselling practices,20 and our results demonstrate that tobacco users are less likely to believe that the profession should be more active in promoting cessation. As such, it is worrisome that the 7.7% prevalence of tobacco use among pharmacy students is more than double that of the licensed pharmacists in our study. Currently, tobacco cessation programmes are being developed specifically for health professionals through collaborations with the Robert Wood Johnson Foundation and the Smoking Cessation Leadership Center at the University of California San Francisco (http://smokingcessationleadership.ucsf.edu/).
Our study results should be generalised with caution, given that all three studies were conducted in California, where the prevalence of tobacco use is lower than the national median.21 Additionally, the response rate for the survey of licensed pharmacists (54%) is subject to response bias, although the pharmacists’ perceptions were notably similar to the student pharmacists’ perceptions. Generalisability of the pharmacy student data is supported by evidence that 3.5% of 3064 pharmacy students surveyed throughout the USA are in favour of tobacco sales in pharmacies,22 a proportion that is similar to that obtained from our sample of pharmacy students in California.
The reasons that pharmacies cite for selling tobacco have been described as “weak and unconvincing”.23 Given the current national shortage of pharmacists, the window of opportunity is wide open for licensed and future pharmacists to make public their opinions and negotiate with employers for tobacco-free practice settings, thereby continuing to raise awareness of this issue and ultimately leading to the removal of the single most important cause of preventable death in our country from pharmacy shelves. Physicians and other health care providers can support this effort by referring their patients to community pharmacies that do not sell tobacco.
What this paper adds
Despite the fact that tobacco sales in US pharmacies contradict the pharmacist’s code of ethics, many community pharmacies in the USA sell tobacco products. Grass roots efforts in recent years have attempted to encourage pharmacies to cease selling tobacco; however, these efforts have been largely unsuccessful. Efforts to convince pharmacy management to remove tobacco products from pharmacy shelves are in need of convincing, published data.
This report presents data from a series of three studies conducted in California: (1) A survey of 1168 licensed pharmacists; (2) a survey of 1518 pharmacy students; and (3) telephone interviews with 988 adult consumers. In sum, there is little-to-no support for tobacco sales in pharmacies among currently licensed pharmacists (1.6% in favour) and future pharmacists (2.0% in favour). Most smokers do not purchase tobacco products from pharmacies, and only 3.2% would shop at their pharmacy less often if it stopped selling tobacco, compared to 14.2% who would shop there more. In conclusion, there is little professional or public support for tobacco sales in pharmacies.
Acknowledgments
Special thanks to our faculty colleagues at the schools of pharmacy that contributed student data toward this report: Drs Eunice Chung, Berit Gundersen, Lisa Kroon, Candis Morello, Leanne Sakamoto, and Renu Singh.
Data for this report were collected under funding from the University of California Tobacco-Related Disease Research Program (grants 7IT-0169 and 10ST-0339 to K Hudmon and grant 8BT-2301 to K Hudmon and M Shreve) and the Department of Health Services Tobacco Control Section grant 94-20949 to the California Medical Association Foundation. Analysis and writing were supported by National Cancer Institute grant 1 R25 CA90720 to K Hudmon and Robert Wood Johnson grant 047139 to S Schroeder.
This research was approved by the Human Investigations Committee (Yale University) and the Committee on Human Research (University of California San Francisco).
REFERENCES
Footnotes
-
↵* Also Department of Clinical Pharmacy, University of California San Francisco School of Pharmacy, San Francisco, California, USA
-
Competing interests: none declared