Article Text

Abstract
Background: The New Zealand 2003 Smoke-free Environments Amendment Act (SEAA) extended existing restrictions on smoking in office and retail workplaces by introducing smoking bans in bars, casinos, members’ clubs, restaurants and nearly all other workplaces from 10 December 2004.
Objective: To evaluate the implementation and outcomes of aspects of the SEAA relating to smoke-free indoor workplaces and public places, excluding schools and early learning centres.
Methods: Data were gathered on public and stakeholder attitudes and support for smoke-free policies; dissemination of information, enforcement activities and compliance; exposure to secondhand smoke (SHS) in the workplace; changes in health outcomes linked to SHS exposure; exposure to SHS in homes; smoking prevalence and smoking related behaviours; and economic impacts.
Results: Surveys suggested growing majority support for the SEAA and its underlying principles among the public and bar managers. There was evidence of high compliance in bars and pubs, where most enforcement problems were expected. Self reported data suggested that SHS exposure in the workplace, the primary objective of the SEAA, decreased significantly from around 20% in 2003, to 8% in 2006. Air quality improved greatly in hospitality venues. Reported SHS exposure in homes also reduced significantly. There was no clear evidence of a short term effect on health or on adult smoking prevalence, although calls to the smoking cessation quitline increased despite reduced expenditure on smoking cessation advertising. Available data suggested a broadly neutral economic impact, including in the tourist and hospitality sectors.
Conclusion: The effects of the legislation change were favourable from a public health perspective. Areas for further investigation and possible regulation were identified such as SHS related pollution in semi-enclosed outdoor areas. The study adds to a growing body of literature documenting the positive impact of comprehensive smoke-free legislation. The scientific and public health case for introducing comprehensive smoke-free legislation that covers all indoor public places and workplaces is now overwhelming, and should be a public health priority for legislators across the world as part of the globalisation of effective public health policy to control the tobacco epidemic.
Statistics from Altmetric.com
The New Zealand Smoke-free Environments Amendment Act (SEAA) 20031 became law on 10 December 2003. The act introduced a range of tobacco control measures including that all schools and early childhood centres must be smoke free from 1 January 2004, and nearly all other indoor workplaces from 10 December 2004, including bars, casinos, members’ clubs and restaurants.
Smoking was allowed in outdoor “open” areas, including where these were semi-enclosed, provided they did not meet the Ministry of Health’s definition of an enclosed “internal” workplace. The exact definition of an internal and open area was complex (see http://www.moh.govt.nz/smokefreelaw). An online calculator was made available on the Ministry of Health website in September 2005 to help businesses determine if an open workplace area was compliant.
Several partial exemptions were allowed, notably prisons, hotel and motel rooms, and residential establishments such as long term care institutions and rest homes. The smoke-free provisions extended existing restrictions on smoking in many indoor workplaces, which were introduced in the 1990 Smoke-free Environments Act.2 The 1990 provisions included smoking bans in public facilities (including retail areas), most shared offices, and partial restrictions (⩾ half of the area non-smoking) for work cafeterias, restaurants and meal serving areas of pubs and other licensed venues, but did not include restrictions on non-meal serving areas of pubs, members’ clubs, nightclubs or casinos. Smoking was still allowed in many non-office workplaces.
The new legislation followed sustained advocacy efforts in response to evidence of persisting significant workplace exposures, in particular of greater exposure among blue collar workers and Maori (the indigenous people of New Zealand).3–5 Maori make up 14.6% of the New Zealand population (Statistics New Zealand, 2007). The immediate trigger for the legislation was a compelling National Health Committee report to Parliament that recommended the introduction of a complete ban on smoking in all indoor workplaces including in hospitality industry settings.6
The tobacco and hospitality industries expressed strong opposition to the proposed legislation, particularly through the Hospitality Association of New Zealand and Clubs New Zealand. Arguments included warnings of dire economic effects in the hospitality and tourism sectors (both major sources of income for New Zealand); difficulty of enforcement and widespread non-compliance; questioning the health effects of SHS; questioning the right of the government to control smoking in commercial premises; and promoting an alternative strategy of ventilation and smoking areas or rooms.7
This paper reports the key findings of a multifaceted evaluation commissioned by the New Zealand Ministry of Health. The evaluation focuses on the process of implementation and on the outcomes of the parts of the SEAA relating to smoke-free indoor workplaces and public places, excluding schools and early learning establishments.
METHODS
Identification of objectives, principles and evaluation information domains
Objectives and guiding principles were identified from the SEAA and other key documentary sources. The main relevant aim in the SEAA was:
“To prevent the detrimental effect of other people’s smoking on the health of people in workplaces, or in certain public enclosed public areas, who do not smoke or do not wish to smoke there.”1
Since the 2003 amendment involved the extension of existing provisions on smoke-free workplaces and public places), we assumed that the main short to medium term objective was to reduce SHS exposure by extending protection to workers still exposed to SHS in indoor workplaces after the 1990 Smoke-free Environments Act. This was the principal aim described in the National Health Committee report on the SEAA.6
Guiding principles identified from New Zealand Ministry of Health strategy documents8–12 and the National Health Committee report6 were, firstly, that the SEAA should promote equity in health by improving health among groups disproportionately affected by tobacco smoking and SHS exposure, such as Maori, Pacific Island peoples, and low income groups. Secondly, that policies should be congruent with the principles and provisions of New Zealand’s founding agreement between the Crown and Maori, the Treaty of Waitangi (see www.waitangi-tribunal.govt.nz/treaty) including ensuring Maori participation, active protection of Maori interests and reduction of inequalities between Maori and non-Maori.
We developed a logic model (fig 1) with process and outcome indicators to underpin the evaluation, adapted from the evaluation model of the US Centers for Disease Control13 and that used for the evaluation of the Scottish smoke-free legislation.14 Goals and indicators for evaluating smoke-free policy interventions were derived from Starr et al.15 Process indicators include activities and outputs. We differentiated outcomes into core outcomes, which relate to the direct, anticipated impacts (boxes with solid lines) and primary objectives of the legislation; and non-core outcomes, which relate to indirect, possible outcomes (boxes with broken lines) and secondary objectives.

The process and outcomes information areas used to structure the evaluation were as follows:
Process and short term outcome indicators:
Public and stakeholder attitudes and support for smoke-free policies
Dissemination of information, enforcement activities and compliance monitoring.
Core intermediate and long term outcome indicators:
Exposure to SHS in the workplace (principal outcome measure)
Health impacts attributable to active smoking and SHS exposure.
Non-core intermediate and long term outcome indicators:
Exposure to SHS in public places and private places such as homes
Smoking prevalence and smoking related behaviours
Economic impacts.
Evaluation methods
We identified data sources from literature searches and consultations with members of the project team and other key informants. We extracted, appraised and summarised the evidence from each relevant data source. Where practicable we carried out additional analyses or studies if the evidence was judged insufficient. These were: further analysis of data from Health Sponsorship Council (HSC) monitor surveys; an exploration of the experiences and attitudes of key stakeholders to the introduction and implementation of the SEAA; a study of indoor air quality (fine particulate levels) in mainly hospitality industry venues; an analysis of hospitalisation rates for a range of respiratory and cardiovascular diseases in relation to implementation of the SEAA; an analysis of the national quitline data; and a series of analyses using available econometric data. Full details of the evaluation methods and additional analyses and studies are provided in the main report.16
Sources of evidence
Evidence on public and stakeholder attitudes towards and support for smoke-free policies before and after implementation of the SEAA came from two nationally representative telephone surveys. The UMR research survey included around 750 adults, and the HSC monitor surveys included 2000–2500 adults, with a boosted Maori population sample.17 18 We carried out additional analyses of one of the 2003–6 HSC monitor surveys, weighting the findings to the age, sex and ethnicity distributions of the 2001 census.16 We also used the findings of a study of the beliefs and attitudes of a cohort of 541 bar managers (some of whom were also owners) conducted by the HSC from November 2004 to November 2005.19
Evidence on compliance came from observational data from four studies carried out mainly in bars and pubs in 2005–6.20–23 The first was a study investigating changes in cotinine levels in customers visiting 30 bars and pubs in Auckland, Wellington and Invercargill.20 23 Another was an ASH study investigating the level of smoking indoors on Friday evenings before and after the SEAA in 193 venues randomly selected from pubs and bars in 20 urban centres across New Zealand.21 Finally, there were observations of smoking from two studies investigating air quality in 37 pubs and restaurants in Wellington and the Wairarapa.22 We also carried out analysis of data from the Ministry of Health’s complaints line that was established for the public to call in and log complaints of smoking in smoke-free areas.16
Evidence about the experiences and attitudes of key stakeholders to the introduction and implementation of the SEAA came from a review we conducted of key documents including print media coverage, and from a stakeholder interview study in which we performed 33 interviews with representatives of employers, union and the hospitality industry; tobacco control non-governmental organisations; Ministry of Health officials; local enforcement officers; and Maori stakeholders.16
Data on workplace SHS exposure came from self reported exposure among participants in the HSC monitor surveys (2003–6).16 Data from hospitality settings came from the Institute of Environmental Science Research bar customer cotinine study. In this study changes in salivary cotinine were measured in volunteers (3–5 per bar) visiting 30 randomly selected bars in Auckland, Wellington and Invercargill, before entering the bar, and after spending about three hours in the bar during the evening in July–November 2004 and July–November 2005.20 Additional data came from measurement of fine particulate levels (particulate matter, PM2.5) in 17 Wellington central business district bars and restaurants, and nine rural pubs in the Wairarapa and 11 bars in central Wellington in two University of Otago air quality monitoring studies during 2006.16 22 Evidence on SHS exposure in the home came from self reported SHS exposure by adults in the HSC monitor surveys,16 and by children in the national year 10 smoking surveys.24 The latter is a cross sectional questionnaire survey of 14–15-year-old children, which included children’s reports of parental smoking and SHS exposure in the home since 2001. Between 1999 and 2005 an average of over 30 000 students participated each year, representing more than 70% of all eligible schools and year 10 students.
The main sources of information on smoking related behaviours and smoking prevalence came from time series analyses we conducted of the number of caller registrations and nicotine replacement therapy (NRT) exchange cards issued by the national quitline before and after the introduction of the smoke-free legislation25; the frequency of smoking reported by smokers in pubs and bars, restaurant and nightclubs in the HSC monitor surveys16; and from market research data from AC Nielsen on supermarket tobacco sales and Statistics New Zealand data on the amount of tobacco released onto the New Zealand market.16 We also used data on reported parental smoking prevalence among children in the national year 10 smoking survey.24
The New Zealand Health Information Service provided data on hospital admissions for cardiovascular and respiratory illnesses for the years 1996–2005 before the introduction of the ban and during the first 12 months after its implementation.
The main sources of information on economic impacts were routinely collected economic activity data available from Statistics New Zealand, as annual and quarterly time series. This included data series on retail sales and employment by sector. Other data included economic activity data relating to construction in the hospitality industry, gambling expenditure and tourism numbers. Data on patronage of hospitality industry venues were available from the HSC monitor surveys, and on problem gambling (calls to the gambling helpline and referrals for counselling) from the Mental Health Directorate of the Ministry of Health’s Problem Gambling Service Providers data. These data sources were used for a series of analyses we conducted specially for the evaluation of the SEAA.16
RESULTS
Public and stakeholder attitudes towards and support for smoke-free policies
We found evidence of strong and growing support for the new smoke-free legislation and its underlying principles among all population subgroups, including smokers and bar managers. For example, by 2006, the HSC monitor surveys16 showed over 90% agreement, and 6% or less disagreement for the right to live and work in a smoke-free environment; and for indoor workers, including bar and restaurant workers, to work in a smoke-free environment (table 1). One of the most marked changes in the HSC Monitor surveys was the increase in support among smokers for the right of bar workers to work in a smoke-free environment, from 57% in 2003, to 83% in 2006 (table 1).16
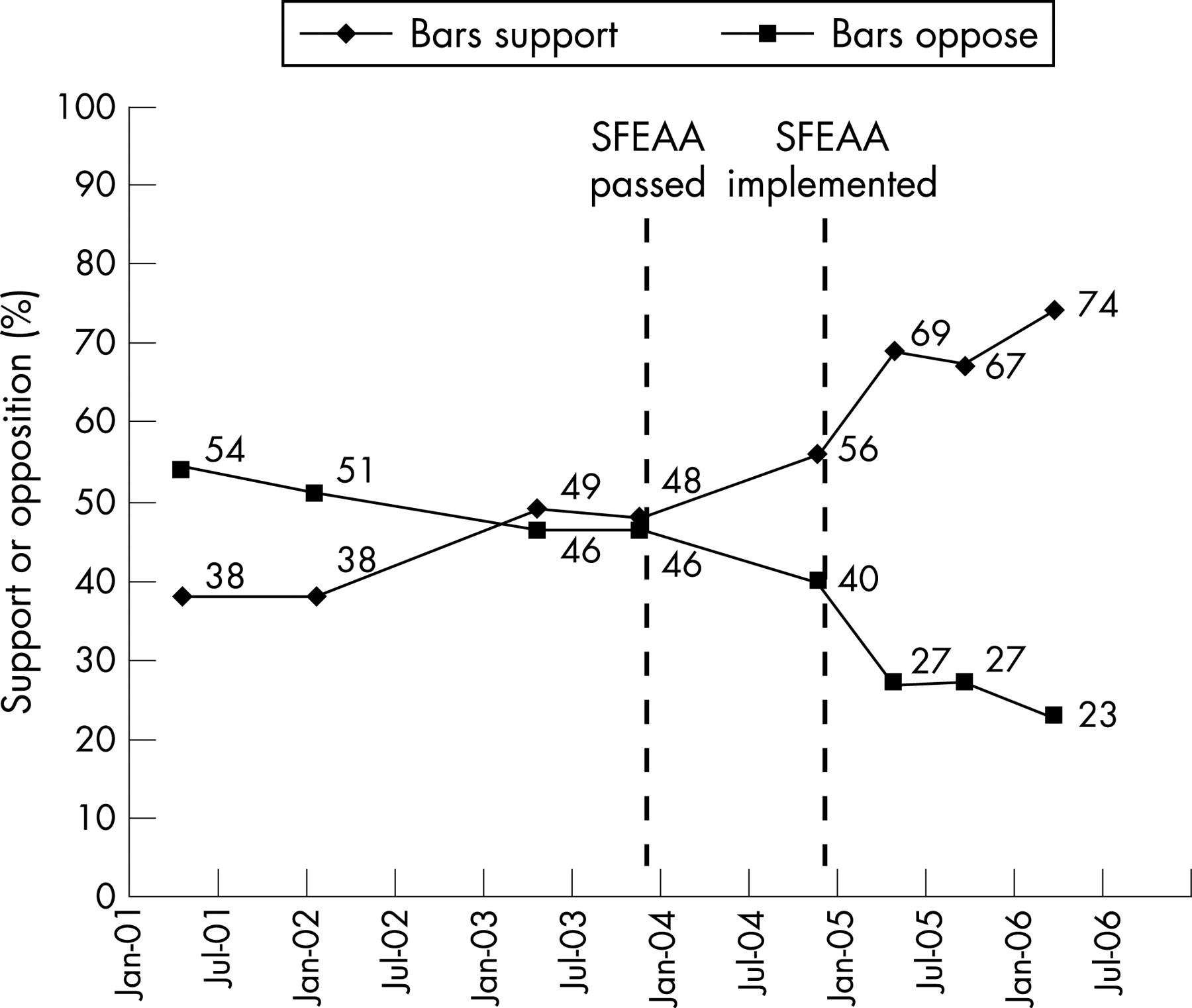
There was a marked increase in support for smoking bans in bars and restaurants in the surveyed population. Figure 2 shows trends in support for smoking bans in bars in the UMR research survey.16 Support for smoking bans in bars increased from 38% in 2001 to 74% by 2006. There was a similar increase in support for smoking bans in restaurants and cafes from 61% in January 2001, to 73% just before SEAA implementation in December 2004, and to 80% in 2006. By 2006 there was roughly equal support versus non-support among smokers for smoke-free bars, and majority support for smoke-free restaurants. Similarly, in the HSC surveys, support for banning smoking in restaurants increased from 73% in 2004 to 90% in 2006 (from 48% to 78% among smokers); and in bars and pubs from 61% to 82% (from 25% to 58% among smokers).16
There was evidence of increasing support among managers from the hospitality industry. In the bar managers cohort study, the proportion supporting (“strongly approve” or “approve”) smoking bans in enclosed areas of pubs increased from 44% at baseline to 60% in November 2005, 11 months after the SEAA (2003) was implemented.19
Dissemination of information, enforcement activities and compliance monitoring
In the years before the SEAA, the HSC and non-government organisations such as Action on Smoking and Health (ASH) periodically ran media campaigns promoting smoke-free homes and workplaces. In August–December 2003, The Quit Group (New Zealand’s national quitline provider) and the HSC ran a campaign, “Let’s Clear the Air,” which drew attention to SHS exposure among hospitality staff in the workplace, and encouraged smokers to smoke outside bars and restaurants.
Before the main implementation of the SEAA in 2004, the Ministry of Health distributed leaflets to businesses throughout New Zealand, and sent three letters to 11 000 hospitality businesses, describing the act and providing information packs and signage. HSC mass media campaigns about the impending law change ran between November 2004 and January 2005, and included Maori language versions screened on Maori television. This campaign was supported by print and radio advertising, leaflets and posters, an information helpline, and a smoke-free law website (www.smokefreelaw.co.nz), as well as by additional promotional material produced by non-governmental organisations, such as the Smokefree Coalition and ASH.
Unlike in other jurisdictions such as Ireland, where there was a proactive programme of inspections of workplaces to monitor compliance, in New Zealand the process of monitoring and enforcement was largely passive. Enforcement officers working within district health boards investigated complaints received largely from members of the public either directly to district health boards or through a national complaints telephone line. The Ministry of Health was responsible for prosecuting persistent offenders. There was no pro-active monitoring and inspection schedule.
Four studies examined compliance using observational data, mainly from pubs and bars. In the ASH study in 193 bars, people smoking indoors were present in only five bars (3%) after the SEAA implementation, compared with 183 (95%) before the new law in July 2004. Smokers represented only 0.23% of the total patrons present inside the bars after the new law.21 In the Institute of Environmental Science Research bar customers cotinine study, of 9610 patrons observed in the 30 bars in Auckland, Wellington and Invercargill in the spring and winter of 2005 only one was seen smoking indoors.20 In the two University of Otago air quality studies, none of the 3038 patrons and staff observed in 37 bars and restaurants at three time points was smoking indoors, but one person was observed smoking outside of the observation period inside a rural pub, as the investigators left.22
Indirect evidence of compliance came from the HSC bar managers’ cohort study, where participants were asked how often they saw patrons smoking inside their venue in the last month. In November 2005, 8% reported seeing smoking on several, most or all shifts, 31% very rarely,and 60% not at all.19
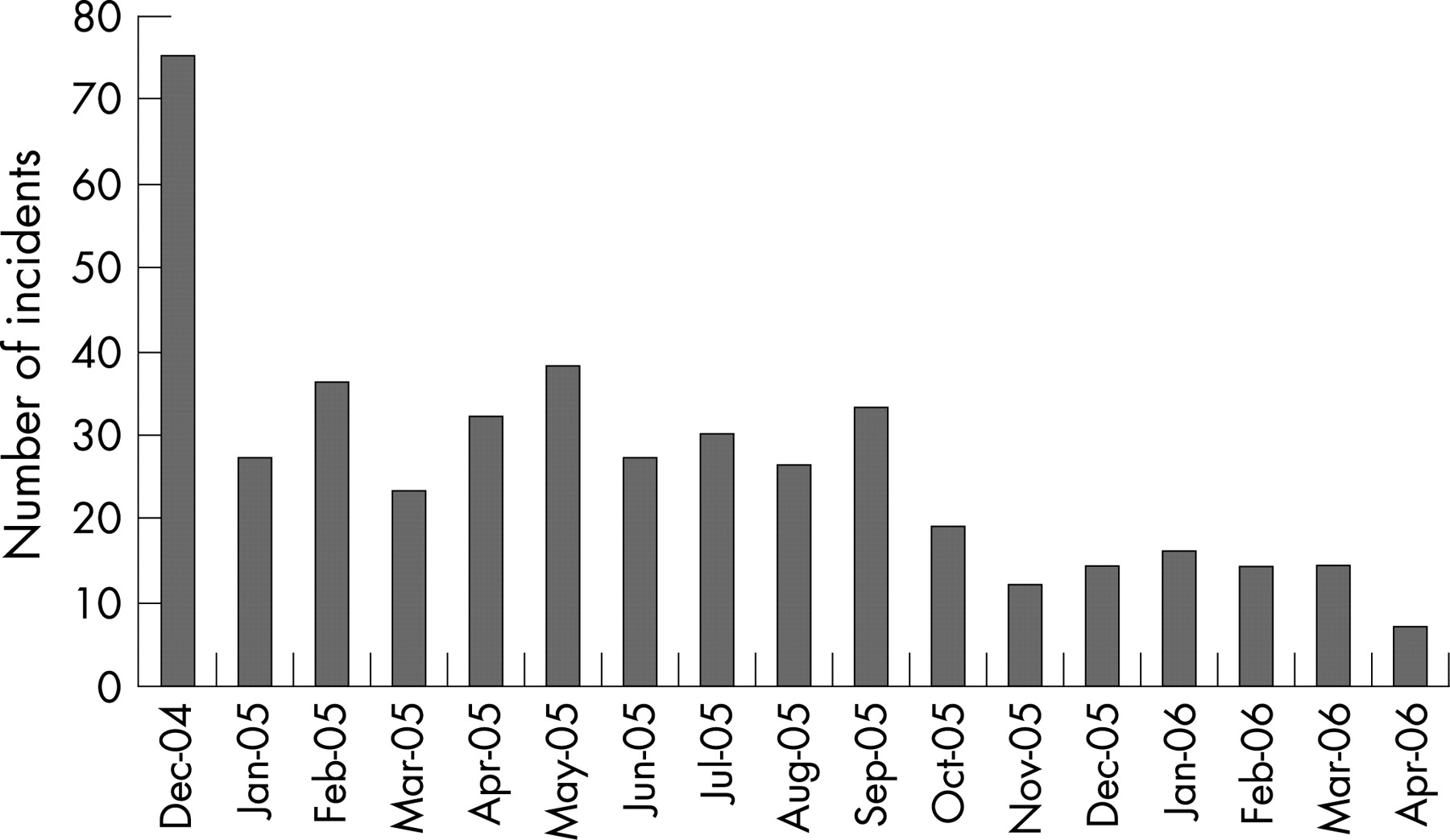
Data from the complaints line database relating to smoking in smoke-free areas are summarised in figure 3. Most (56%) of the complaints were about smoking on licensed premises, and 25% about smoking in other workplaces.16 The number of complaints fell rapidly from 75 in the first month to fewer than 20 per month since October 2005. Most were resolved through letters, telephone calls and visits by enforcement staff. Only five resulted in prosecutions.

Most of the interviewees in the stakeholder study were positive towards the SEAA.16 The legislation was seen as effective at extending protection to staff from SHS exposure, and the implementation process was largely supported, especially the way in which non-governmental organisations were involved in implementation. Maori stakeholders were also largely supportive of the legislation and its implementation. The interviews with Hospitality Association of New Zealand officials and review of the organisations’ official communications revealed a shift from opposition to mostly acceptance of the SEAA, though some concerns were raised.
Concerns identified by the interviewees included confusion over the definition of non-enclosed outdoor areas, a lack of resources for enforcement, failure to prosecute sufficiently promptly establishments that were persistently non-compliant, and problems relating to implementation in workplaces that were partially exempted from the legislation. Some interviewees suggested that there might be persisting non-compliance in licensed premises in remote rural areas, and in smaller businesses with a high proportion of smokers.
Exposure to SHS in the workplace
Before the SEAA, an estimated 17–20% of the adult workforce was exposed to SHS in the workplace during work time and 33% during breaks, with higher exposure among Maori and blue collar workers.5 16 The greatest SHS exposure was among workers in the hospitality sector.26
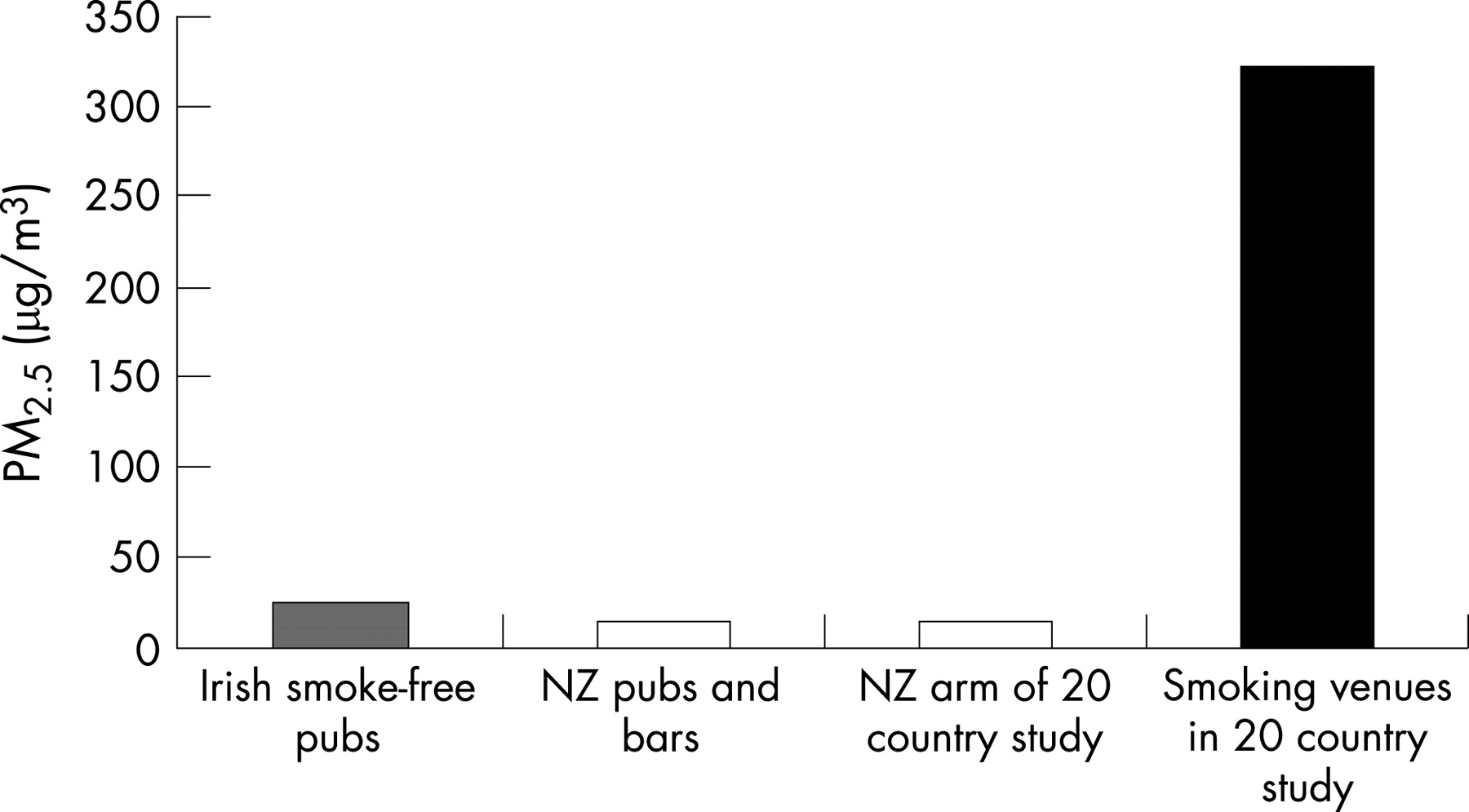
There was good evidence of reduced SHS exposure and improvements in air quality, particularly in hospitality settings. In the Institute of Environmental Science and Research bar customers survey, salivary cotinine was measured in volunteers (3–5 per bar) visiting 30 randomly selected bars in Auckland, Wellington and Invercargill, before entering the bar, and after spending about three hours in the bar during the evening.20 23 The mean salivary cotinine increase post-SEAA was 0.08 ng/ml, a 90% decrease from the pre-SEAA mean increase of 0.66 ng/ml. In the University of Otago air quality studies, the mean fine particulate (PM2.5) levels were measured using methods used in a series of air quality studies around the world.27–30 Mean levels of fine particulates in samples of urban and rural pubs and bar areas and urban restaurants varied between 13 and 22 μg/m3. Indoor particulate levels were similar to those in the outdoor air. The levels were also similar to measurements from a range of other smoke-free venues in New Zealand included in an international comparative study,28 and in studies from smoke-free pubs in other countries such as Ireland.31 Levels in the bars and restaurants were far lower than found in international studies from hospitality venues where smoking is allowed (fig 4).28 There was preliminary evidence that particulate levels in semi-enclosed outdoor smoking areas were high in some pubs and bars.22
Self reported SHS exposure indoors at work in the previous week among HSC survey participants fell from around 20% in 2003, to 8% in 2006 among employed adults (fig 5).16 There were greater reductions among Maori. Workplace exposure in 2006 was highest among men (12% vs 4% among women), and for workers in blue collar jobs such as labouring and operating machinery (up to 17%).32

Health impacts caused by active smoking and SHS exposure
Hospitalisation rates for acute asthma, acute stroke, unstable angina, and exacerbations of chronic obstructive pulmonary disease were lower in the 12 months after implementation of the SEAA relative to the preceding 12 months but these findings were not confirmed in a more rigorous Poisson regression analysis which adjusted for longer term trends and other potential influences on hospitalisation rates.16 There was therefore no clear evidence that the hospitalisation rate for these health outcomes reduced in the first 12 months after implementation of the SEAA.
SHS exposure in the home and other settings
Self reported SHS exposure in the home among participants in the HSC monitor surveys fell from 20% in all households (42% of households with one or more smokers) in 2003, to 9% (30% of households with one or more smokers) in 2006.16 In the same surveys, the proportion of homes reported as smoke free (no smoking was allowed indoors) also increased during this time period. For example, the proportion of homes reported as smoke free, where there were one or more smokers and one or more children living, increased from 64% in 2003 to 70% in 2006. Reductions in self reported SHS exposure and increases in smoke-free home policies were more marked in Maori households, particularly among households with one or more smokers.
In the year 10 survey, the proportion of students reporting that smoking occurred in their home decreased from 30.5% in 2001 to 26.5% in 2005, with no change in the downward trend between 2004 and 2005.24 Figures for 2006 were not available.
An interesting finding from the Institute of Environmental Science and Research study was a decrease in the mean cotinine level of the volunteers before visiting the bars, from 0.25 ng/ml in winter 2004 and 0.17 ng/ml in summer 2004 before the SEAA, to 0.05 ng/ml in winter and spring 2005 after the act was implemented.20 As all the participants were non-smoking volunteers who reported no regular SHS exposure in the home or at work, this provides evidence of a general reduction in SHS exposure in other settings such as public places.
Smoking prevalence and smoking related behaviours
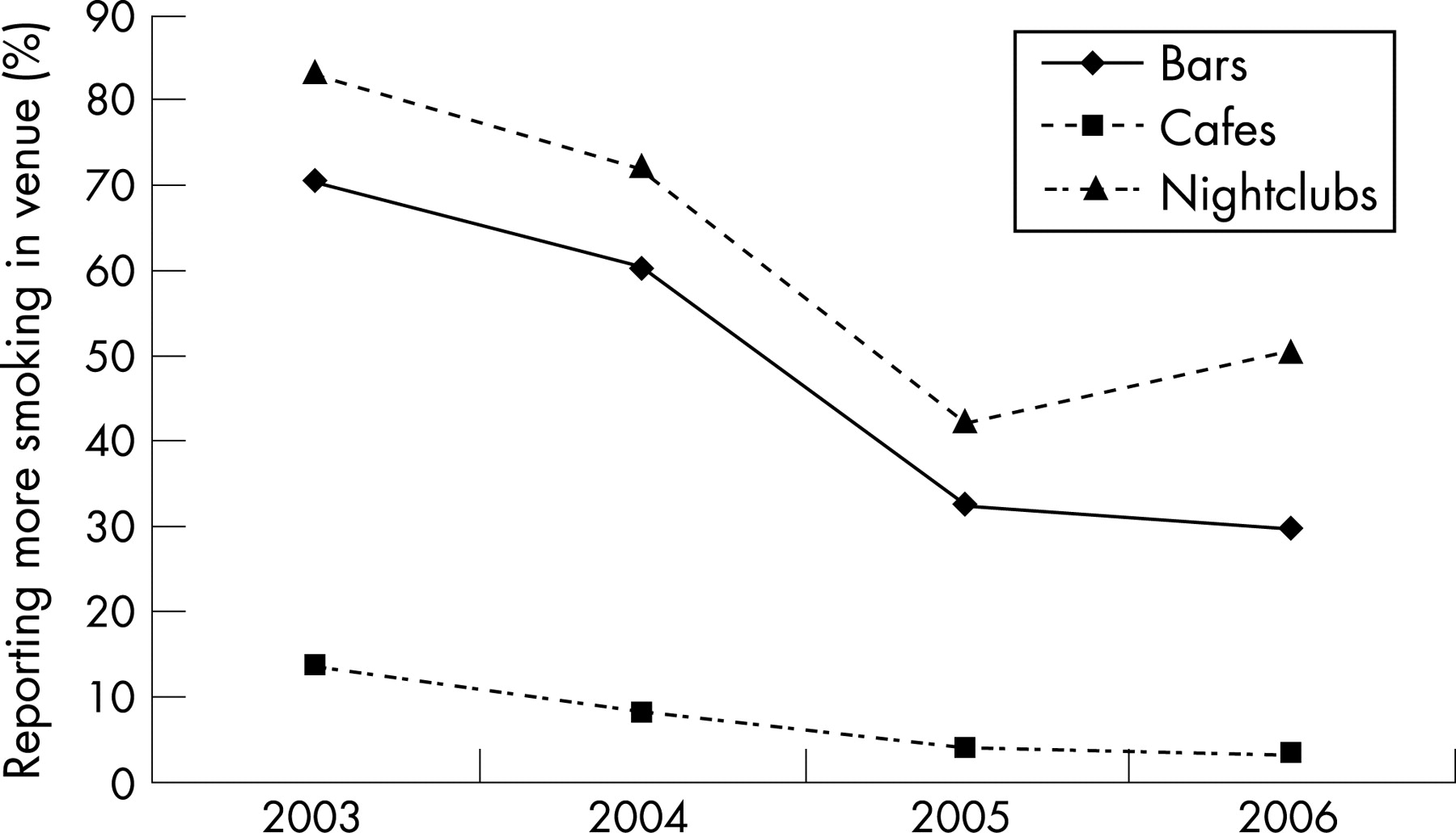
Analysis of the quitline caller data showed that the expected summer dip in caller registration and issuing of NRT vouchers disappeared in December 2004/January 2005. Numbers of calls remained elevated each month compared to the previous year until March 2005, and the monthly number of NRT vouchers issued was higher until May 2005.25 This pattern was observed despite a marked reduction in advertising expenditure on smoking cessation promotion in early 2005, partly implemented to reduce demand. As a result, caller registrations per dollar of smoking cessation advertising spend for the six month period after implementation of the SEAA increased 2–4-fold compared to the four preceding six month periods, and for issuing of NRT exchange vouchers increased 3–5-fold. In a time series analysis adjusted for advertising expenditure and media coverage of tobacco control issues, implementation of the SEAA was significantly associated with a significant short term increase in monthly caller registrations (p = 0.025). The increase in NRT vouchers issued after implementation of the SEAA did not reach statistical significance. Socially cued smoking (smoking more than normal) at bars, nightclubs, casinos and cafés substantially declined between 2003–4 and 2005–6 (fig 6).

Youth smoking rates decreased significantly between 2004 and 2005, but in line with long term trends with no discernable effect of the SEAA.24 There was also a small reduction in reported parental smoking in the year 10 survey between 2004 and 2005.24 The per capita release of tobacco onto the New Zealand market (a marker for overall consumption) was fairly constant from 2003–5, with no evidence of any change in 2005 following implementation of the SEAA.16 There was a small decline in tobacco supermarket sales after the law change though this reflects only a small proportion of the tobacco market, and may have represented the continuation of long term trends.16
Economic impacts
Data from the HSC monitor surveys revealed little change in the reported patronage of bars and pubs between 2003–4 and 2005–6.16
Figure 7 shows total annual retail sales in the three main sectors of the hospitality industry and, to explore possible displacement effects, of alcohol sales in stores where alcohol is sold for home consumption (specialist liquor retailers). There has been a downward trend in annual retail sales in bars and clubs since 2002 (fig 7), which continued in 2005. Similarly liquor stores sales had been increasing slightly since 2003, and continued to do so in 2005. Regression analysis of quarterly data series suggested that after adjustment for long term trends, there was probably a modest additional reduction (around 4%) in retail sales of bars and clubs in the first quarter of 2005, with some evidence of displacement to liquor retailers for home sales.16 However, the effect was not sustained, and subsequent figures were in line with pre-existing trends. Patronage and sales for cafes and restaurants have increased steadily since 2002. The rate of increase was maintained or possibly slightly greater after implementation of the SEAA. Trends in employment in these hospitality sectors largely mirrored the retails sales data.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The 1990 smoke-free legislation did not cover casinos, but through a 1997 amendment casinos were required to ensure that at least 25% of the floor areas was smoke free. Following implementation of the SEAA casinos were made fully smoke free. In addition, much of the gambling in New Zealand is in bars, using “pokie” (slot) machines. It is plausible therefore that smoke-free legislation could reduce problem gambling, a particularly important problem in New Zealand—for example, if smokers having to take a break outside to smoke reconsidered whether to continue gambling. There was evidence of decreased expenditure on gambling, and large falls in the numbers accessing the problem gamblers’ helpline and face to face counselling services in the period after SEAA implementation. This followed many years of increases in all these indicators. For example, 2875 new clients contacted the gambling helpline in 2005, a 33.1% decrease from 2004.16
The number of overseas visitors and their expenditure increased by 1.5% and 3.3% respectively in 2005, to record levels.16 This increase was slightly less than that predicted from the long term trend, but followed a year with record numbers of visitors and the biggest annual percentage increase in a decade. The increases in visitor numbers and expenditure in 2005 occurred despite an unusually high value of the New Zealand dollar against the currencies of the three countries with the greatest numbers of international visitors to New Zealand.
DISCUSSION
Summary and discussion of findings
Overall, we found many positive results and few negative ones from a public health perspective. There was convincing evidence of strong and increasing public support for the smoke-free aspects of the SEAA, and the underlying principles of protecting the rights of non-smokers from SHS exposure in workplaces and public places. There was increasing evidence of acceptance, if not full support, of the SEAA by the hospitality industry, which had vigorously opposed its introduction.
Enforcement processes and infrastructure have mostly worked well. The available evidence suggests that compliance is high within the hospitality industry, including bars and pubs where most enforcement problems were expected. The high level of compliance suggests that smoke-free policies were largely self policed, by smokers themselves, or by other patrons and hospitality staff. Compliance may have been increased and enforcement facilitated by broad support for the SEAA. This would have been helped by work to promote and explain the policy to the public, and involve and inform key stakeholders that started well before and continued during implementation. This was carried out by the Ministry of Health, supported by non-governmental organisations.
High levels of compliance were achieved despite a largely passive system of monitoring and enforcement, concerns about limited resources available for enforcement and implementation, and the perception by some of a missed opportunity to demonstrate rigorous enforcement through early prosecutions of non-compliant workplaces. Ministry of Health officials argue that their approach reflected a policy decision to focus on educating and working with employers, including establishments reported to have breached the law, with prosecution for cases of repeated and flagrant violation (personal communication) used as a last resort.
There was evidence from self reported data that SHS exposure in the workplace decreased, the primary objective of the SEAA. The decrease was reported among groups disproportionately exposed to SHS after the 1990 Smoke-free Environments Act—for instance, the disparities between Maori and non-Maori were removed. There was also evidence from studies of particulate levels in restaurants and bars, and cotinine levels of volunteers visiting bars that air quality substantially improved in the hospitality sector. There was still a significant proportion (around 8%) of the workforce, particularly men in industrial settings, who reported exposure to indoor SHS in the workplace, indicating considerable further scope for enforcement and health promotion work.
We found no evidence for an impact on hospitalisation rates for SHS associated diseases in the general population in the year following SEAA implementation. This contrasts with findings from other settings.33–35 Possible reasons for failure to identify reduced hospitalisation rates include: changes in exposure to the other causes for these conditions masking the effect of changes in SHS exposure; the limited amount of disease attributable to SHS exposure for these conditions (for example, in comparison with active smoking); that the SEAA only directly addressed smoking in the workplace, whereas much SHS exposure occurs in the home and other private settings; and that the SEAA could only reduce SHS exposure among workers still exposed to SHS indoors in the workplace at the time of implementation, a small minority by 2004.
There is strong evidence that SHS exposure results in adverse health effects,36 37 and good evidence that implementation of the SEAA reduced SHS exposure in the workplace, in New Zealand and probably in other settings. Therefore, despite the failure of the hospitalisation study to demonstrate unequivocal health benefits, possibly because of limitations in the study design, it is likely that health benefits as a result of the SEAA have occurred and will continue to accumulate over time.
There had been speculation by opponents that comprehensive smoke-free legislation would increase SHS exposure in the home, as smokers were no longer able to smoke in pubs and bars.38 We found no evidence to support this speculation. On the contrary, there was evidence that SHS exposure in homes reduced following implementation of the SEAA. Ideally, confirmatory objective evidence is required, using biomarkers to investigate these trends.
There was no convincing evidence of an impact of the SEAA on smoking prevalence and consumption. This may be because of a lack of robust data, and the short timeframe for evaluation after implementation. There was clear evidence of reductions in socially cued smoking and also of increased calls to the quitline in the period after implementation, suggesting that the SEAA had other positive impacts on smoking related behaviours, which may result in reductions in smoking prevalence in the long term. However, the opportunity to maximise the number of smokers making a quit attempt as a response to the introduction of the SEAA changes was missed, partly because there was a planned reduction in advertising of the quitline in the period after SEAA implementation in order to help manage demand for the service.
The economic data that were available suggested a broadly neutral effect, with no evidence of a significant impact on the tourist industry or a sustained impact, beyond the first quarter of 2005, on the hospitality industries including bars, where opponents had predicted the most severely negative effects. There was some evidence of a positive impact on the restaurant and cafe sector. There was evidence of a reduction in gambling expenditure and problem gambling, but attributing this change to the SEAA alone is difficult as new gambling legislation introducing stricter controls over licensing of venues with non-casino gaming machines, and limits on the number of machines per venue were implemented between May and December 2004. It is also possible that other factors affected recorded gambling spending in New Zealand, such as a transfer of spending to online gambling outside the country.
Strengths and weaknesses of the evaluation
The available data came from a mix of specially commissioned studies, ongoing studies and routine statistics. There were some important gaps and weaknesses in the evidence available for the evaluation.
Routine data often have limitations since it is not usually collected in a way that would maximise usefulness for policy evaluation. This is certainly true of the economic data, where it would have been useful to have detailed data series such as turnover, profits and employment for specific subsectors; as well as comprehensive information on possible confounding factors such as changes in population income, price of products and services in the sector and changes to other relevant regulations. Similarly, for the health impacts data, the evidence was limited by being based on routinely available hospitalisation data. For example, there was no information on the rates of exposure to SHS and smoking, and changes in other risk factor levels among those admitted with potentially smoking or SHS related diseases. There were also no studies of highly exposed groups, such as bar workers. This was a major omission from the evaluation of the SEAA, and contrasts with the approach taken in Ireland38 39 and Scotland.14 We would recommend that such studies should be carried out wherever possible to evaluate and document the impact of smoke-free legislation on health in other jurisdictions.
The ongoing and specially commissioned studies were generally of high quality. The biggest potential problems were:
low response rates in some surveys which may have resulted in selection bias
use of self reported SHS exposure without corroborating information from biomarkers data
lack of coverage of some key areas—for example, small numbers of rural pubs and non-hospitality workplaces in studies of compliance and air quality; and failure to investigate health impacts among heavily exposed workers, such as bar workers.
Finally, nearly all the studies described in this report used a before-after approach, without any comparison control group(s). Smoking prevalence, smoking related behaviours which influence SHS exposure, levels of health and illness, and economic indicators are changing over time. These trends may have been influenced by implementation of the SEAA, but also by a wide range of potential confounding determinants. Without a long run of observations before and after implementation of the SEAA, and detailed information on changes in possible confounding determinants, it is not possible to deduce precisely the long term trends and the independent effect of the SEAA. Generally the information about confounders was very limited, and most of the data series are restricted to a few time points before the legislation, and data from only 12–18 months after. Therefore, except where there were dramatic changes after introduction of the SEAA as, for example, with the reduction in the increase in cotinine levels after bar visits in the Institute of Environmental Science and Research study and improvements in air quality in hospitality settings, conclusions about the scale of the impact of the SEAA are subject to some uncertainty. However, the mostly positive nature of the impacts is likely to be robust.
Implications for further research and policy development
From the perspective of how to best improve and protect public health, further research is needed on many aspects of secondhand smoke exposure and the smoke-free legislation in New Zealand. This should include research into the extent of the problems posed by smoking in outdoor areas, particularly where semi-enclosed or adjacent and open to indoor smoke-free areas; the extent, and implications, of smoking on marae (traditional Maori meeting places); the extent of, and trends in, SHS exposure in adults and children, using biomarkers of exposure in population based samples; further efforts to quantify health impacts; and investigation of the experience and impact of the SEAA in schools and early learning establishments.
Developments in policy and regulation are also imperative. The fact that reduced promotion of the quitline was considered necessary to “manage demand” after implementation suggests that increased resources are required to meet that demand. We believe that future important tobacco control interventions should be accompanied by planned increases in the provision of resources for cessation promotion and support, including promotion of the quitline service. Also, while the available data show overall high levels of compliance with the smoke-free provisions in pubs and bars, more proactive monitoring of compliance and enforcement of the smoke-free provisions of the SEAA is needed in non-hospitality, non-office settings where indoor workplace SHS exposure commonly persists. Finally, additional approaches, including the possibility of regulatory action, may be required to protect hospitality workers and non-smoking customers from smoking in semi-enclosed outdoor areas, and to protect workers and non-smoking residents in currently exempted institutions such as prisons and residential homes.
Conclusion
This evaluation of smoke-free legislation in New Zealand adds to an extensive and rapidly growing body of supportive and consistent evidence from countries and states such as Ireland, Norway, Scotland, New York and California that have introduced similar legislation.40 The scientific and public health case for introducing comprehensive smoke-free legislation that covers all indoor public places and workplaces is now overwhelming, and should be a public health priority for legislators across the world as part of the globalisation of effective public health policy to control the global tobacco epidemic.
What this paper adds
This paper describes a comprehensive, multifaceted evaluation of a national smoke-free law in New Zealand (implemented in 2004). The findings are mostly positive for each of the key process and outcome measures investigated. There is evidence of strong and growing support for the smoke-free legislation; high compliance in pubs and bars; reduced secondhand smoke (SHS) exposure for all indoor workers, with self reported exposure falling from around 20% in 2003, to 8% in 2006; and broadly neutral or slightly positive economic effects.
Novel findings included the lack of evidence for any displacement of smoking into homes, with evidence instead of reduced SHS exposure in the home. The experience from New Zealand also underlined the need to increase the resources available for cessation support following the introduction of smoke-free legislation.
Acknowledgments
We thank the members of the advisory group: Shane Allwright, John Britton, Becky Freeman, Hayden McRobbie, Leigh Sturgiss and Yannan Xiang for advice on the full report of the 2003 Smokefree Amendment Act evaluation.
Sharron Bowers and Christine Groves provided administrative support.
Clare Bear, Candace Bagnall and Courtenay Mackie of the Ministry of Health provided general support. Courtenay Mackie and Ashley Bloomfield provided helpful comments on this manuscript.
The Health Sponsorship Council (HSC) provided additional support and access to their datasets. Specifically: Kiri Milne and Nigel Guenole provided data from the bar managers study; Kiri Milne information about the HSC media campaigns; Stella McGough gave helpful comments and advice for the HSC monitor survey analysis, and access to a draft analysis of SHS exposure by job titles and occupational setting.
Kamalesh Venugopal of the Department of Public Health, University of Otago, Wellington performed the weightings and preliminary analysis for the additional HSC monitor survey analyses. Robert Templeton of Public Health Intelligence at the Ministry of Health provided additional advice on the weighting procedure.
Mark Tisdall Associates carried out the bulk of the recruitment of participants and interviews for the stakeholders study.
Graham Gillespie and the Public Health Directorate of the Ministry of Health, provided information about the Ministry’s enforcement processes and resources for the SEAA (2003); and Brendon Baker and Olivia Tuatoko provided information about the complaints database
Michele Grigg, Judy Li and other Quit Group staff supplied the relevant quitline data, and funded the purchase of advertising expenditure data relating to the quitline (kindly supplied by Jodi Hogan of Graham Strategic).
The Smokefree Coalition obtained tobacco data from Statistics New Zealand.
Mark Travers of the Roswell Park Cancer Institute and IARC, Lyon, loaned air quality monitoring equipment. Anthony Maher, Jenny Näthe and Rafed Jalali assisted with data collection in bars and restaurants for the air quality studies. Rod Lea of Environmental Science Research helped with the discussion of the Environmental Science Research study cotinine data.
Robyn Whittaker of the University of Auckland helped with the health impacts study; and Gary Jackson and Dean Lapa at Counties Manukau District Health Board helped with the hospitalisation data.
Statistics New Zealand provided datasets for the economic impacts analysis.
We thank the reviewers of Tobacco Control for helpful comments on the draft manuscript.
REFERENCES
Footnotes
Funding: The evaluation and some of the primary data collection were funded by the New Zealand Ministry of Health. Other primary research studies were funded by a variety of agencies detailed in the relevant publications. The views expressed are those of the authors and do not necessarily represent those of the Ministry of Health.
Competing interests: GT, NW, MG, DO’D and ML have previously undertaken contract work for not for profit organisations involved in tobacco control. MG is on the advisory board for Pfizer Champix, and has been on similar boards for GSK Zyban in the past, and carried out contract work for Novartis training Aukati Kai Paipa in use of NRT many years ago.