Article Text

Abstract
OBJECTIVE To monitor the effect of a novel nicotine delivery device that may produce fewer carcinogens (Eclipse) on cigarette smoking, carbon monoxide and nicotine concentrations, and motivation to give up smoking. The smoker's own brand of cigarette and a nicotine replacement product (Nicotrol inhaler) were used as comparisons.
DESIGN After baseline data were recorded, smokers were randomised to either Eclipse or inhaler for two weeks and then switched to the other product for another two weeks. Thereafter a second baseline was obtained.
SETTING AND PARTICIPANTS Fifty smokers were included and data are reported for the 40 with complete data sets. The smokers were not trying to quit but were interested in trying a new product to reduce their risk. They visited a smoking clinic 10 times during the six week period of the trial.
INTERVENTION No counselling to aid reduction by Eclipse or inhaler was given.
MAIN OUTCOME MEASURES At each visit smoking status and carbon monoxide concentrations were recorded. In half of the visits withdrawal symptoms, attitudes towards smoking, heart rate, and blood nicotine concentrations were also recorded.
RESULTS Eclipse use decreased the number of cigarettes smoked per day (cpd) from 19.1 cpd at baseline to 2.1 cpd (p < 0.001), but increased carbon monoxide concentrations in parts per million (ppm) from 21.0 ppm to 33.0 ppm (p < 0.001). A similar decrease in cigarettes smoked per day was seen with the Nicotrol inhaler, from 19.1 cpd to 4.8 cpd (p < 0.001), but carbon monoxide decreased from 21.0 ppm to 12.7 ppm (p < 0.001). The blood nicotine concentration remained fairly stable with Eclipse, increasing slightly from 16.8 ng/ml to 18.0 ng/ml, while for the inhaler a significant drop was noted, from 16.8 ng/ml to 12.2 ng/ml (p < 0.002). Craving and withdrawal did not increase with Eclipse. Few significant adverse events occurred with Eclipse.
CONCLUSIONS Eclipse can dramatically decrease cigarette consumption without causing withdrawal symptoms or decreases in nicotine concentrations or motivation to quit altogether. Unlike the inhaler, Eclipse produces an increase in carbon monoxide concentration. Thus Eclipse may not be a safer cigarette.
- tobacco
- nicotine
- harm reduction
- nicotine replacement
Statistics from Altmetric.com
The dangers of tobacco smoking are well known and it has been argued that modification of cigarettes could have a great impact on public health.1 The tobacco industry has recently begun to modify their products. The first development was Premier, a cigarette that did not burn but heated tobacco. Premier was never marketed widely, probably because smokers did not like the taste and low nicotine delivery. Premier also came under fire as being a drug delivery system.2
Eclipse—a novel nicotine delivery device—is a product that appears similar to Premier in many ways. It primarily heats rather than burns tobacco related material. In industry studies, when smokers have switched to using only Eclipse, tar exposure decreased dramatically by 70–90%.3 In both industry and independent tests, nicotine blood concentrations were similar between smoking only Eclipse versus usual brand of cigarettes.3 4 In an independent study, carbon monoxide concentration derived from smoking two Eclipse devices was similar to smoking two regular cigarettes.4 In an industry study, smoking only Eclipse for two weeks increased carboxyhaemoglobin by 18%.5 In a recent study by independent investigators respiratory measures improved in heavy smokers who switched to Eclipse for four weeks.6
The manufacturer's marketing claims originally centred on less and “cleaner” environmental tobacco smoke, but more recently explicit health claims—less cancer and lung disease—have been made.7
Although some studies are available,3 4 very little is known from real life studies how smokers use Eclipse and their resultant toxin exposure. For example, the effect of Eclipse on smoking and on motivation to stop using tobacco altogether; which smokers are interested in Eclipse, and the safety of Eclipse compared to conventional cigarettes are unclear.
The present study focused on comparing Eclipse with conventional cigarettes in regard to several outcomes. In addition a nicotine replacement inhaler was compared because nicotine replacement products are becoming more widely available to smokers. Because nicotine replacement products are much safer than cigarettes,8 some clinicians and scientists have suggested that they should be used in a manner similar to Eclipse—that is, not just as an aid to stop smoking but also as a cigarette substitute.9
The major aim of our study was to monitor the effect of using Eclipse and the nicotine replacement device, Nicotrol inhaler, on reducing the smoking of cigarettes and intake of carbon monoxide and nicotine. Secondary aims were to examine effects on motivation to give up smoking and product preferences. We recruited smokers with little motivation to quit as these are the smokers most likely to use Eclipse.
Methods
SUBJECTS
Fifty smokers from Helsingborg in Sweden were recruited during August and September 1997 following the placement of an advertisement in a local newspaper. The advertisement stated: “NEW PRODUCTS TO REDUCE THE RISK OF SMOKING A new type of cigarette that does not burn but heats tobacco, and a new nicotine replacement product, an inhaler, have recently been marketed. These products emit much less or no passive smoke and they also produce much less or no exposure to many of the harmful substances from smoking. If you don't want to stop smoking within the next months and you can commit yourself to four weeks of intense monitoring, and possible 10 more weeks of less intense monitoring, you are welcome to contact us. Products will be free of charge and you will earn 500 SEK (US$60) for your participation.”
Inclusion criteria were: (a) agree to follow the trial procedure, (b) age 20–65 years, (c) in good general health; (d) good ability to read and understand Swedish; (e) smoke at least five cigarettes daily; and (f) agree to sign an informed consent. Exclusion criteria were: (a) severe or symptomatic cardiovascular disease; (b) pregnancy; (c) breastfeeding; (d) regular psychotropic medication use; (e) abuse of alcohol or any other drug; or (f) use of smokeless tobacco or nicotine replacement therapy. At the time of the study, an Eclipse product—Inside—was being test marketed in Sweden.
The first 30 smokers were included in the order they phoned the clinic. The remaining 20 smokers were selected to provide a similar prevalence of sexes and high/low dependence. Sixty seven per cent of all the smokers who were interested in participating in the study were women, and 77% of the smokers were regarded as being highly dependent—that is, they scored > 3 on the Heaviness of Smoking Index.10The baseline averages (SD) for the 50 smokers were: age 49.2 (9.6) years; cigarettes/day (cpd) 20.2 (7.9); nicotine dependence (Fagerström test for nicotine dependence10) 5.4 (1.7); and number of quit attempts 3.4 (3.6).
DESIGN
The study was conducted in two parts. The first part was a crossover study with a baseline determination followed by two weeks of using one product, then two weeks using the other product, and then a two week return to baseline. The second part was an eight week preference and use study. This article reports the results of the first part.
After a baseline visit, the smokers were randomised to a two week use of Eclipse or the inhaler. At the end of the two weeks, the groups crossed over to the other treatment. The randomisation was made in blocks of two. After the first four weeks, all smokers returned to smoking their own cigarette brand for two weeks. At the end of six weeks (four weeks cross over study and two week wash out) they chose one product (own cigarette brand, Eclipse or inhaler) to use exclusively for the second part of the study. Each smoker visited our clinic for the baseline visit and on the fifth and seventh day of each of the four weeks of the crossover period, and at the six week visit.
PROCEDURE
At the baseline visit subjects recorded demographic data, medical and smoking history, attitudes to smoking, nicotine dependence,10 motivation for quitting, and smoking withdrawal symptoms.11 Also, smoke intake was assessed by measuring carbon monoxide in exhaled air (Bedfont Smokerlyzer Bedfont Scientific Ltd, Upchurch, UK and by plasma carboxyhaemoglobin; nicotine and cotinine concentrations in saliva and blood,12 and heart rate, were also measured and recorded. At all study visits, we recorded the amount of product used, the number of cigarettes smoked per day, carbon monoxide and saliva cotinine concentrations, concomitant medication, and adverse events (via an open ended question). In addition, at visits on days 7, 14, 21, and 28 we recorded withdrawal symptoms on a five point scale (from 0 = “not at all” to 4 = “extremely”) and heart rate, plus blood was taken in addition to saliva for determining plasma nicotine and cotinine concentrations.12 Inquiries into intentions about quitting smoking were repeated only at days 14 and 28.
At the baseline visit the smokers were given product (Eclipse or inhaler) in quantities sufficient to last until the next visit, and a diary card to record product and cigarette use daily through all four weeks. The products were given free of charge. In order to increase compliance smokers were offered reimbursement at the last visit. The smokers' visits to the clinic always occurred in the afternoon at approximately the same time of day. Most visits took no more than 5–7 minutes. The smokers were instructed to smoke as few cigarettes of their own brand as possible without discomfort and instead use as much of the treatment product as needed. No counselling was provided. After four weeks smokers were asked to smoke their own cigarettes (not using Eclipse or the inhaler) for two weeks as a return to baseline.
The study was approved by the local ethics committee and performed according to the ethics code of Helsinki.
TREATMENT PRODUCTS
Eclipse
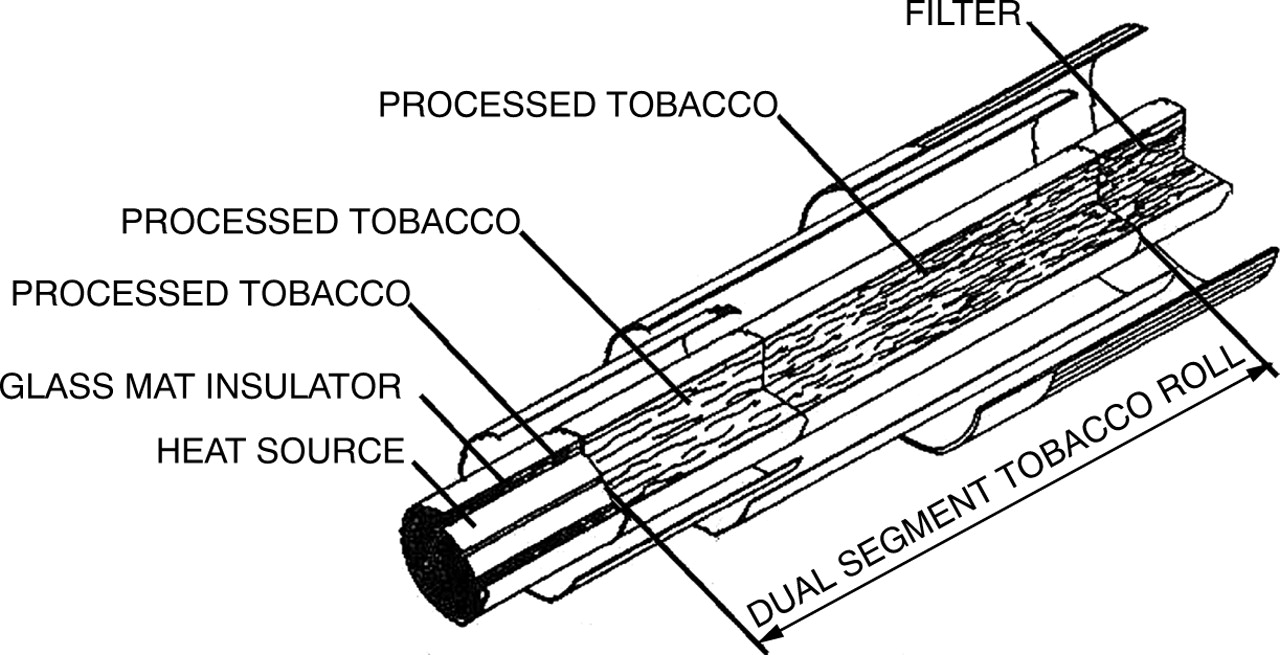
Eclipse is composed of a heating source in the distal end, and two compartments of tobacco and a filter at the proximal end (fig 1). The heating source has three components: a carbon pellet surrounded by glass fibre insulation material that, in turn, is inside a layer of tobacco paper. The more distal of the two tobacco compartments contains glycerin treated reconstituted tobacco. The more proximal compartment is made up of finer cut tobacco similar to regular cigarette tobacco. When the Eclipse is lit, hot air (600–800°C) aerosolises glycerin from the distant tobacco compartment which absorbs nicotine when passed over the tobacco. The machine smoke yield listed on the pack gives it a low yield character of 3 mg tar, 0.2 mg nicotine, and 8 mg carbon monoxide. In scientific studies the manufacturer states Eclipse contains less particulate matter and carcinogens and specifically less formaldehyde, benzene, toluene, and several nitrosamines than light cigarettes.13 Eclipse Regular, called Inside, was provided by Swedish Match, Stockholm, Sweden. The smokers were instructed to use Eclipse in the same way as they smoked cigarettes.

Schematic illustration of Eclipse.
Inhaler
The Nicotrol inhaler (Pharmacia Corporation) is a licensed nicotine replacement product for smoking cessation. The inhaler comprises a plastic tube containing a plastic pellet that is saturated with 10 mg nicotine and 1 mg menthol. When the inhaler is puffed on it provides air saturated with nicotine. The nicotine concentration of 3–6 mg/l is much lower than that found in the mainstream smoke of a cigarette. The descriptor “inhaler” is somewhat inappropriate since only very tiny amounts of nicotine are absorbed in the lungs14; instead nicotine is absorbed bucally like nicotine gum. Blood concentrations of nicotine resulting from use of the inhaler are typically half of that derived from cigarettes.14 The inhaler does not produce carbon monoxide or carcinogens. Smokers were encouraged to puff much more frequently on the inhaler than their cigarettes and to change to a fresh cartridge as often as they liked, but to use at least four cartridges per day.
STATISTICAL METHODS
Comparisons of baseline and treatment were performed separately for Eclipse and the inhaler using repeated measures analysis of variance (ANOVA), with sequence as a between subject factor. By including a treatment by sequence interaction term in the model, we tested whether the difference between baseline and treatment differed for the two treatment periods. The Wilcoxon signed rank test was used to compare initial baseline values with the values at the return to baseline period. To compare Eclipse and the inhaler directly, we used ANOVA for a 2 × 2 crossover trial. In order to be able to determine if treatment effect differed depending on baseline value, we included baseline as a covariate.15 Analysis using a traditional 2 × 2 crossover ANOVA ignoring baseline gave similar treatment and sequence findings for all outcomes except the withdrawal symptoms scale, where an interaction with baseline value was detected. Only the results for the model including baseline are presented here. For the binary variable “Do you intend to quit smoking in the next six months”, McNemar's test was used to examine changes from baseline for Eclipse and the inhaler, and the Mainland-Gart test was used to test for treatment, sequence, and time period effects when comparing Eclipse and the inhaler.15 A probability value of p < 0.05 was considered to be significant for all analyses.
Results
Four smokers dropped out because of adverse events, two were lost to follow up, and three were lost for other reasons—for example, moving, sickness, could not attend the strict visit times because of work changes, and one did not attend the baseline visit. Of these 10 drop outs, four occurred when using Eclipse and five with the inhaler. Results are reported for 40 subjects that have complete data sets throughout the four weeks.
One subject was omitted from the cigarette per day analysis and one from the carbon monoxide analysis because of extreme values at baseline (values over three standard deviations higher than the mean). For the cigarette per day analysis, the subject consumed 50 cpd while the next highest value was 31 cpd. For the carbon monoxide analysis, the subject had a reading of 46 ppm while the next highest was 34 ppm. For both these measures, inclusion of the outlying subject led to a significant baseline by sequence by treatment interaction that depended only on that one subject. The outlier was omitted because of the questionable generalisability of a three way interaction that is significant solely because of one extreme value. Removal of the outlier did not affect the significance of any other findings for analyses, including main effects for treatment, time period, sequence, or covariates, or any of the two way interactions. One subject was also missing from the carbon monoxide analysis because of missing data at week 4.
COMPARISON OF TREATMENT WITH BASELINE
Eclipse use decreased the number of cigarettes smoked per day from a mean of 19.1 cpd to 2.1 cpd (p < 0.001) (fig 2), but increased carbon monoxide concentrations from 21.0 ppm to 33.0 ppm (p<.001). Inhaler use decreased cigarette consumption from 19.1 cpd to 4.8 cpd (p < 0.001) and decreased carbon monoxide concentrations from 21.0 ppm to 12.7 ppm (p < 0.001).

{kind=link}
{kind=link}
Baseline, treatment, and return to baseline values for number of cigarettes smoked per day, carbon monoxide concentration, plasma nicotine concentration, and motivation to quit smoking.
There were no significant changes in nicotine and cotinine concentrations with Eclipse, while with the inhaler nicotine decreased from 16.8 ng/ml to 12.2 ng/ml (p < 0.002) and cotinine decreased from 330 ng/ml to 259 ng/ml (p < 0.001). Ratings of missing cigarettes on a five point scale increased with both treatments, from 0.4 to 1.5 for the Eclipse (p < 0.001) and from 0.4 to 2.2 for the inhaler (p < 0.001). Subjects used an average 15.5 Eclipses per day and 7.0 inhaler cartridges per day. Craving decreased with Eclipse from 2.3 to 1.9 (p < 0.04) but was unchanged with the inhaler, from 2.3 to 2.1. For other withdrawal symptoms no differences were seen with either product.
On motivation to quit smoking (visual analog scale of 10 cm) an increase was noted for Eclipse users from 5.4 cm to 6.8 cm (p < 0.005). For the inhaler a non-significant trend from 5.4 cm to 5.9 cm was seen (p < 0.16). On the intention to give up smoking within the next six months an increase was seen for both treatments from 48% of smokers at baseline to 68% (p < 0.01) for Eclipse, and from 48% to 72% (p < 0.002) for the inhaler. No significant effects on heart rate were found.
The number of cigarettes smoked per day and carbon monoxide concentrations regained their initial levels when smokers entered the return to baseline period. Motivation to stop smoking was not measured during the return to baseline.
ECLIPSE AND INHALER COMPARISONS
When Eclipse was used fewer cigarettes were smoked, but carbon monoxide, heart rate, nicotine and cotinine concentrations, and motivation to give up were higher than when the inhaler was used (table1). Intention to give up smoking in the next six months did not differ between products.
Comparisons of the main effects of Eclipse and Nicotrol inhaler
There was no difference in craving between the products, but Eclipse produced fewer withdrawal symptoms (p < 0.01) and less missing of cigarettes (p < 0.001). For cigarettes smoked per day, there was a period effect (p < 0.02) owing to fewer cigarettes being smoked per day with both the inhaler and Eclipse in the first treatment period compared to the second. A similar effect was found for missing cigarettes (p < 0.01), with less missing for both treatments in the first treatment period compared with the second. For withdrawal symptoms, there was a baseline by treatment by sequence interaction (p < 0.01). Stratified analysis indicated that for subjects with low initial withdrawal symptoms, symptoms increased with the inhaler but not with Eclipse (p < 0.002), while for subjects with high initial withdrawal symptoms, symptoms decreased with both the inhaler and Eclipse in the second treatment period compared to the first (p < 0.003).
SUBJECTIVE EVALUATIONS OF THE INHALER AND ECLIPSE
After two weeks, before being crossed over, subjects were asked to compare the inhaler and Eclipse with cigarettes. Eclipse was rated as stronger than the inhaler (1.83 v 1.15 on a four point scale; Wilcoxon signed rank test, p < 0.05). Eclipse was less embarrassing than the inhaler (0.13 v0.55, p < 0.05). Liking of the product compared with cigarettes was similar at 1.40 and 1.35 for Eclipse and inhaler, respectively. The taste compared with cigarettes did not differ between the inhaler and Eclipse (0.95 v 1.30). The flavour rating compared with cigarettes was better for the inhaler than Eclipse (3.30v 2.2, p < 0.01). The draw resistance on a three point scale (0 = too light and 2 = too hard) was similar; 1.4 for the inhaler and 1.5 for Eclipse.
ADVERSE EVENTS
A total of 64 adverse events were reported; 32 for each of the devices. The adverse events were generally the same for both. The most frequent symptoms reported were headache and coughing (six times) and gastritis (five times). The few symptoms that tended to differ were dry mouth (four reports with Eclipse versus one with the inhaler) and gastritis/dyspepsia (two reports with Eclipse versus six with the inhaler). Three subjects on Eclipse and one on the inhaler dropped out because of adverse events. None of the adverse events was serious.
PREFERENCE
At six weeks the subjects could choose to use Eclipse, the inhaler or their own brand of cigarettes for another eight weeks. All three products would be provided free of charge. For the 39 subjects participating in this part of the study 15 (38%) chose cigarettes, 14 (36%) the inhaler, and 10 (26%) Eclipse.
Discussion
Our major findings were threefold: (a) Eclipse produced a dramatic decrease in the number of cigarettes in smokers trying to reduce smoking with no increase in craving or withdrawal; (b) despite the dramatic reduction in smoking, Eclipse increased carbon monoxide to a clinically significant degree; and (c) using Eclipse did not change nicotine concentrations and did not appear to undermine motivation to quit.
Eclipse is currently marketed with claims such as less second hand smoke and lower risk of cancer and lung disease.7 However, when labelled a less risky product and given to smokers not interested in quitting and asked to reduce, Eclipse use was associated with a 85% reduction in the number of cigarettes smoked per day. The large magnitude of this effect and its reversibility with the return to baseline strongly suggest Eclipse actively suppressed cigarette use. Several lines of evidence suggest that Eclipse was functioning as an adequate cigarette substitute: (a) the number of Eclipse used per day plus the number of cigarettes smoked per day appeared to remain constant; (b) use of Eclipse and < 5 cpd did not result in increased withdrawal or craving; and (c) the liking for Eclipse was similar to that of cigarettes.
Even though the number of cigarettes per day decreased by 85% with Eclipse, the concentration of carbon monoxide increased by 50%. Importantly carbon monoxide declined upon switching to the inhaler after cessation of Eclipse. This strongly suggests Eclipse was actively increasing carbon monoxide. This is important as carbon monoxide is predictive of increased risk of heart attacks21 and a 12 ppm increase could be clinically significant.
Our finding of a 50% increase in carbon monoxide would not be predicted from data from smoking machines listed on the Eclipse pack. Our increase in carbon monoxide was larger than that seen in the industry study,5 despite the fact that both Eclipse and cigarettes were used by smokers in our study whereas only Eclipse was available in the industry study. The industry study included US smokers who smoked more than 20 cpd and thus had higher baseline carbon monoxide concentrations than the Swedish smokers in our study. Whether our lower carbon monoxide concentrations are caused by differences in US or Swedish cigarettes or by differences in the smoking pattern of US versus Swedish smokers is unknown. It may be that our greater increase in carbon monoxide is because our smokers began with lower concentrations. The industry study reported carbon monoxide in the form of carboxyhaemoglobin. In the present study carboxyhaemoglobin was also analysed but it was decided to report the more commonly used carbon monoxide in expired air since the effects on carboxyhaemoglobin and carbon monoxide were similar.
One concern is that because Eclipse can be seen as a safe way to smoke and can be used to escape the stop smoking message of smoking restriction, its availability may undermine motivation to quit. This concern is magnified by recent findings that smokers who switched to what were previously considered to be “safer cigarettes”—that is, low tar cigarettes—were less likely to go on to stop smoking than those who did not switch.16 In the current study, Eclipse may have actually increased motivation to stop smoking. This increase may have been caused by the large reduction in smoking with Eclipse in the absence of craving and withdrawal increases. On the other hand, because we did not measure motivation during the return to baseline, the increase in motivation may have been simply caused by participating in an experiment in which one focuses on their smoking. At any rate, our data certainly suggest Eclipse does not decrease motivation to quit.
Although we have focused our discussion on Eclipse, we did find some interesting things out about the inhaler. It too dramatically decreased smoking without worsening craving and withdrawal, and it too may have increased motivation to quit. Importantly, unlike Eclipse, the inhaler decreased rather than increased carbon monoxide. On the other hand, the inhaler was less able to maintain nicotine concentrations, was rated as more embarrassing, and did not substitute for missing a cigarette as well as Eclipse.
In the USA, neither Eclipse nor the inhaler are currently promoted for reducing smoking, although Eclipse, since it is unregulated and easily available, could be used to reduce smoking. Whether promoting reduced smoking among smokers not trying to quit will produce a net public health benefit is unclear for several reasons.17 First, although early data are encouraging,18 it is unclear whether smokers can make a large reduction in smoking and maintain this for long periods. Second, whether reductions in cigarettes smoked per day will be accompanied by reductions in other toxins or be negated by compensatory smoking is unclear. Third, whether reduced smoking will increase motivation to quit or will undermine quitting is also unclear. In this and one other study,19 the inhaler appeared to give positive results in all three of these areas. Thus, further studies, especially those on the long term use of Eclipse for smoking reduction, are indicated.
One asset of our study was that it used a within smokers crossover design with a return to baseline, providing a direct comparison of cigarettes, Eclipse, and inhaler. Another asset was that smokers could use both Eclipse and their own cigarettes, thereby replicating the conditions likely to prevail in the real world. A third asset was our choice of clinically relevant measures such as carbon monoxide as a marker for toxin exposure, withdrawal discomfort, motivation to stop smoking, and preference among products.
One limitation of our study was our short test condition. It is possible that with further use of Eclipse, carbon monoxide might have decreased. Another limitation is that we did not measure carcinogen concentrations; thus, we do not know whether Eclipse would have dramatically decreased these concentrations as it did in a study by the manufacturer.3
Eclipse has not sold well either in the USA or in Europe. This is thought to be because of its poor taste, problems in lighting it, etc. In addition, recent studies (published after we completed our study) indicate smoking Eclipse can result in inhalation of glass fibres.20 Thus, whether Eclipse itself will become widely used is unclear. However, given the increasing call for cigarette regulation and some statements by the tobacco industry that traditional cigarettes might be harmful, we believe it highly likely that reduced risk products will be marketed by the tobacco industry in the future. Our results indicate such products must be tested carefully because their net public health effect is unclear. For example, assume a clinician, or a smoker, saw the smoking rate decline from 18 cpd to 1.5 cpd while using a product that claims to have 90% less carcinogens and no increase in nicotine and carbon monoxide concentrations. The clinician might conclude that Eclipse had produced a positive benefit to his or her patient. However, our results indicate the patient would probably have a carbon monoxide concentration that was even higher than that derived from smoking his or her own cigarettes. Given that death from cardiovascular disease appears to be linked to carbon monoxide, the switch to Eclipse may not reduce the smoker's risk for cardiovascular disease and may even increase it.21 Finally, given that Eclipse may have a higher risk for cardiovascular disease and possibly for lung diseases (as a result of ingestion of glass fibres), we believe that, as with nicotine replacement products, further testing should be mandatory before allowing Eclipse to be marketed.
Acknowledgments
The authors express their gratitude and thanks to Dr Urbain Säwe at Pharmacia & Upjohn for help in planning and analysing this study, and to Bodil Jahnström and Dr Lars Ek at the department of pulmonary medicine at Helsingborg Hospital for excellent management of the study. Pharmacia & Upjohn Consumer Healthcare in Helsingborg, Sweden sponsored this study. Dr Hughes's efforts were sponsored by Research Scientist Development Award 00109 and grant 11935 from NIDA, and by sabbatical support from Pharmacia & Upjohn. Karl Fagerström was an employee of Pharmacia & Upjohn at the time the study was carried out.