Article Text

Abstract
Objective: To compare nicotine pharmacokinetics and subjective effects of three new smokeless tobacco potential reduced exposure products (PREPs; Ariva, Revel and Stonewall) with moist snuff (Copenhagen) and medicinal nicotine (Commit lozenge).
Methods: 10 subjects completed a randomised, within-subject, crossover study. Subjects used one product for 30 min at each of the five laboratory sessions. Maximal nicotine concentration (Cmax) was determined and area under the concentration time curve (AUC) was calculated for a 90-min period (during use and 60 min after use). Nicotine craving, withdrawal symptoms and ratings of product effects and liking were measured during product use.
Results: Nicotine AUC and Cmax were higher for Copenhagen than for any other product (p<0.002) and higher for Commit than for either Ariva or Revel (p<0.001). Cmax for Commit was also higher than for Stonewall (p = 0.03). Craving was lowest during use of Copenhagen (p<0.03). Craving during use of Stonewall, Ariva and Commit was lower than during use of Revel (p<0.05). Withdrawal symptom score during use of Copenhagen was lower than during use of Revel (p = 0.009). Copenhagen scores were higher (p<0.005) than all other products in several measures of drug effects and liking (feel good effects, satisfaction, liking and desire for product, and strength of product).
Conclusion: The new smokeless tobacco PREPs result in lower nicotine concentrations and equivalent or lower reductions in subjective measures compared with medicinal nicotine. Since health effects of PREPs are largely unknown, medicinal nicotine should be preferentially encouraged for smokers or smokeless tobacco users wishing to switch to lower-risk products.
- AUC, area under the concentration–time curve
- Cmax, maximal nicotine concentration
- PREP, potential reduced exposure product
- Tmax, maximal tobacco concentration
Statistics from Altmetric.com
- AUC, area under the concentration–time curve
- Cmax, maximal nicotine concentration
- PREP, potential reduced exposure product
- Tmax, maximal tobacco concentration
Over the past several years, a number of new tobacco products have been introduced, some of which are being marketed, either implicitly or explicitly, as having reduced toxicant exposure or decreased health risks. To assist in evaluating these potential reduced exposure products (PREPs), the United States Food and Drug Administration in 1999 asked the Institute of Medicine to formulate methods and standards by which PREPs could be assessed.1 More recently, an expert panel was convened to develop guidelines for the evaluation of PREPs on both individual and population levels. Among the topics addressed was human clinical testing, which included recommendations on methods and biomarkers to assess PREPs.2,3 The recommended evaluation of PREPs included conducting studies on the pharmacokinetic properties of the products and assessing misuse liability by measuring subjective responses to the products and ability of the products to suppress withdrawal.3
The use of smokeless tobacco products, in lieu of cigarettes, has been suggested as a promising method by which to reduce tobacco-related health consequences.4 Currently, tobacco companies including major cigarette-manufacturing companies are test marketing smokeless and spitless tobacco products (eg, Camel Snus by Reynolds American, Taboka by Philip Morris) as a substitute for smoking. Although overall morbidity and mortality associated with the use of moist snuff or chewing tobacco is lower than the risks associated with cigarette smoking, health consequences such as increased rates of oral and pancreatic cancers remain.5,6 Furthermore, health effects of all forms of smokeless tobacco are not equivalent. For example, an evaluation of the content of tobacco-specific nitrosamines found large differences between the various forms and brands of smokeless tobacco.7 In a human study, a significant decrease in the uptake of tobacco carcinogens has been observed when users of conventional brands of smokeless tobacco switch to Swedish snus.8 A comparison of several brands of moist snuff products found significant differences between brands in the amount of unionised (free) nicotine9–11 and in exposure to nicotine and heart rate response after use of a single dose of each product.12 To accurately assess the potential health effects of a product and the factors associated with consumer use, it is therefore necessary to test each smokeless tobacco product individually, including evaluating the nicotine pharmacokinetics.
The purposes of this study were to assess the pharmacokinetics and subjective responses of smokeless tobacco users when using three new PREPs and to compare them with a commonly used brand of moist snuff (Copenhagen) and the medicinal nicotine lozenge (4 mg Commit). The new smokeless tobacco products studied were (1) Ariva, a compressed powdered tobacco lozenge manufactured to contain low tobacco-specific nitrosamines by Star Scientific marketed for use by smokers when they cannot or choose not to smoke; (2) Stonewall, another compressed powdered low tobacco-specific nitrosamine tobacco lozenge from Star Scientific marketed as a spit-free alternative for users of traditional moist snuff smokeless tobacco products; and (3) Revel, a spit-free smokeless tobacco packet marketed by US Smokeless Tobacco for smokers seeking a discrete alternative to smoking.
METHODS
Study design
We conducted a randomised crossover study in which nicotine concentrations and subjective responses were assessed during and after the use of each of five nicotine/tobacco products (Ariva, Stonewall, Revel, Commit and Copenhagen). The order of product use was randomised between subjects. Therefore, each subject completed a total of five laboratory sessions and had used each product once. At each laboratory session, the tobacco product was used for 30 min. Subjective measures were obtained during product use, and plasma nicotine concentrations were obtained during product use and for the subsequent hour (for a total of 90 min). Subjective measures assessed included a measure of nicotine craving, nicotine-withdrawal symptoms and a measure of product effects and liking.
Subjects
Participants were recruited from the University of Minnesota and surrounding communities through flyers and advertisements in the local media. To be eligible, potential subjects had to be aged between 18 and 65 years and have had used Copenhagen smokeless tobacco daily for at least 1 year. Subjects with unstable medical or psychiatric conditions, taking drugs likely to interact with the products being tested, using any other tobacco or nicotine products, in whom any of the products tested would be contraindicated, having severe periodontal or other oral lesions or with a history of substance misuse within the previous year were excluded. The study was approved by the University of Minnesota Institutional Review Board and written informed consent was obtained from all subjects.
Laboratory sessions
All laboratory sessions were conducted at the General Clinical Research Center, with each visit lasting approximately 4 h. Before each laboratory session, subjects were required to refrain from using any tobacco product for at least 12 h. Over a total of five sessions, subjects received in a random order 2 g of Copenhagen (a typical amount per dip),13 an Ariva lozenge, a Stonewall lozenge, a Revel pouch (manufacturers’ directions for use of the PREPs suggest that one lozenge/pouch should be used at a time) and a 4 mg Commit lozenge (a standard dose).
Although a 12-h pre-session abstinence was required, to ensure at least 2 h abstinence from smokeless tobacco before product use, 2 h elapsed between subjects’ arrival at the General Clinical Research Center and baseline measurements. Thirty minutes before product use, an indwelling catheter was inserted to facilitate blood draws. After completing baseline questionnaires, subjects placed the assigned product between their cheek and gum for 30 min after which the product was removed and subjects rinsed their mouth with water. Blood was drawn immediately before and at 1, 5, 10, 15, 20, 25, 30, 45, 60, 75 and 90 min after product placement. Questionnaires assessing symptoms of nicotine craving and withdrawal were assessed immediately before product placement. Symptoms of nicotine craving, withdrawal and assessing product effects and liking were also assessed at 5, 15 and 30 min after product placement. During each laboratory session, subjects were allowed to read or watch television after the 30-min period of product use. Laboratory sessions for an individual subject occurred at least 3 days apart.
All blood samples were analysed to determine plasma nicotine concentrations. Concentrations of nicotine in serum were measured by gas chromatography with nitrogen–phosphorus detection.14 All nicotine concentrations represent nicotine base. The lower limit of quantitation was 2 ng/ml in plasma. For samples with nicotine concentrations lower than the lower limit of quantitation (2 ng/ml), a value of 1 ng/ml was used for analysis.
To assess withdrawal symptoms, a modification of a questionnaire previously used to assess withdrawal symptoms in those using smokeless tobacco was applied.15 As withdrawal symptoms were assessed several times over a short time period, questions pertaining to hunger and insomnia were removed. Subjects rated on a scale of 0–4 each of the following seven symptoms: craving, irritability/frustration/anger, anxiety/tension, difficulty concentrating, restlessness, depressed or sad mood and impatience. Craving was reported as an individual measure and the withdrawal score was obtained by adding the scores of the remaining six items. To assess measures of drug effects and liking, subjects were asked to rate 17 measures of drug liking or drug effects on a scale of 1 (not at all) to 10 (extremely). This scale was adapted from scales described previously.16–20
Statistical analysis
Non-compartmental methods (WinNonlin Professional V.5.0, Pharsight Corporation, Mountain View, California, USA) were used to determine each subject’s area under the concentration time curve (AUC), time to reach maximal concentration (Tmax) and maximal nicotine concentration (Cmax). AUC was calculated for the 90-min period during which plasma samples were obtained. A log transformation of AUC, Cmax and Tmax was used for statistical analysis to better approximate a normal distribution. Linear mixed models with random subject effects were used to assess differences of log-transformed outcome measures between the five smokeless tobacco products. Variables included are products and session. Baseline value of each measurement is included as a covariate in the model.
In analysing each of the subjective effects (ie, craving, withdrawal, items on the drug effects and liking questionnaire), the score of each of these measures was treated as a continuous variable. A linear mixed model with random subject effect was applied to analyse the differences among products. Variables included are product, time and session. Baseline value of the measure was included as a covariate for craving and withdrawal symptoms analysis. Interactions between product/session and time were included in the initial models but removed from the final model if not found to be significant. Quadratic term of time as well as its interactions with product/session were included if they were significant.
Pearson’s correlation coefficients were calculated between subjects’ nicotine AUC and the average craving score (average of score at 5, 15 and 30 min for each laboratory session) as well as between nicotine AUC and average withdrawal scores.
All statistical analyses were performed using SAS V.9.1. A p value of <0.05 was considered significant. The Tukey method was used to adjust p values for pairwise comparisons.
RESULTS
Subjects
Ten subjects completed all five sessions and were used in the analysis. One additional subject completed only one laboratory session and was excluded from the analysis. All the subjects were male. The average age of subjects at the time of enrolment was 30.9 (range 20–49) years. Subjects reported using an average of 2.4 (range 1.5–3.5) tins of smokeless tobacco per week and an average of 8.1 (range: 3–25) dips of smokeless tobacco per day.
Nicotine pharmacokinetics
Figure 1 illustrates the nicotine concentration–time profile for the five smokeless tobacco products. Significant differences were found in nicotine AUC between several products. Copenhagen had the highest AUC of the five products studied, which was significantly higher (p<0.001) than the AUC observed with Commit, Stonewall, Ariva and Revel (table 1). The AUC observed with Commit was significantly higher (p<0.001) than either Ariva or Revel and tended to be higher (p = 0.06) than Stonewall. No other significant differences in nicotine AUC were found between products.
Nicotine area under the concentration–time curve and maximal nicotine concentration for five smokeless products tested

Mean (±SE) plasma nicotine concentrations during and after the use of five smokeless products.
Copenhagen had the highest Cmax of the five products, which was significantly higher (p<0.002) than the Cmax observed with Commit, Stonewall, Ariva and Revel (table 1). The Cmax observed with Commit was significantly higher than Revel (p<0.001), Ariva (<0.001) and Stonewall (p = 0.03). No other significant differences in Cmax were found between products.
No significant differences in Tmax were observed between the three products in which nicotine concentration consistently increased above baseline among subjects (ie, Copenhagen, Commit, Stonewall), with Cmax observed at an average of 27–33 min after starting product use.
Subjective effects
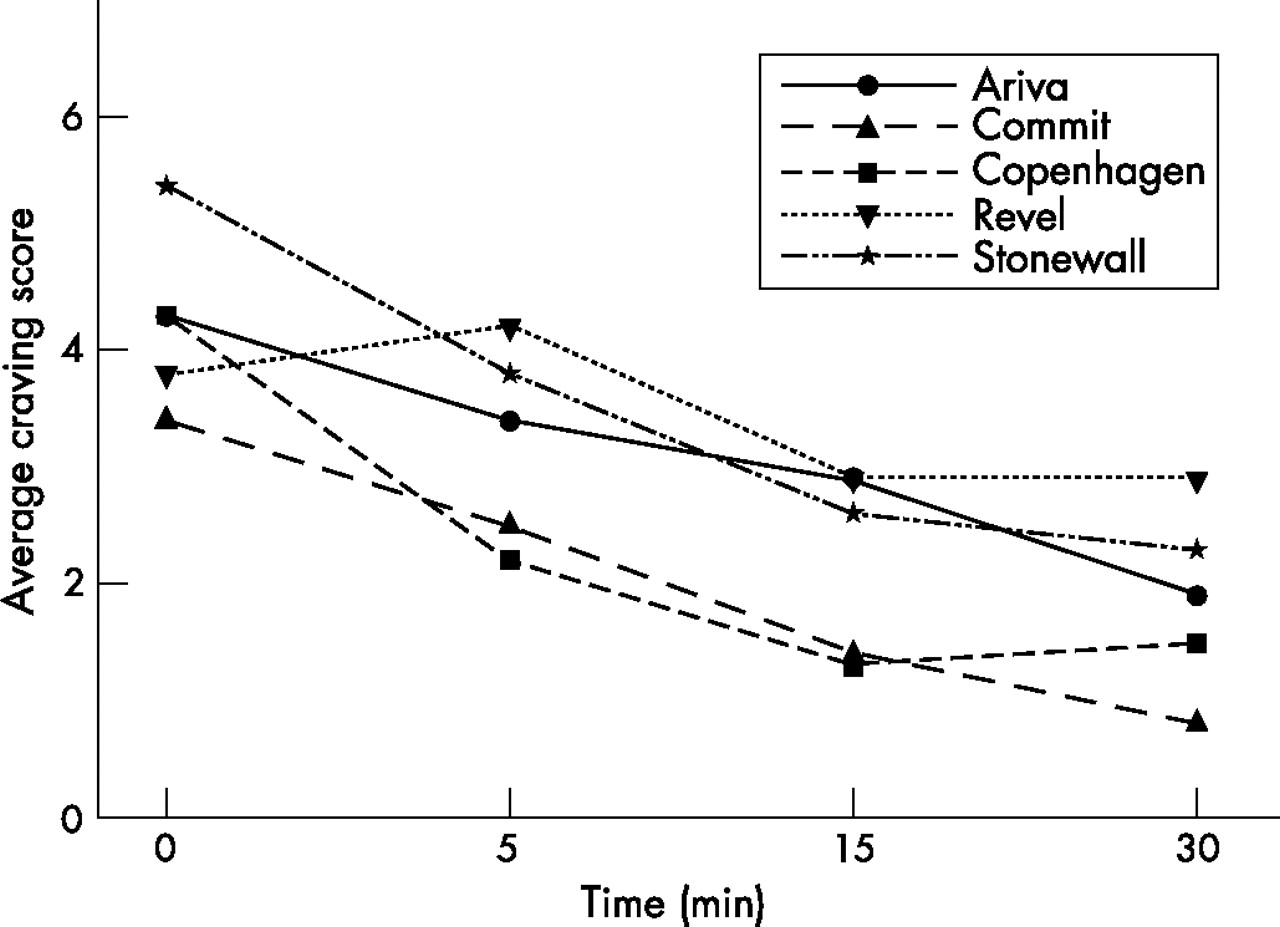
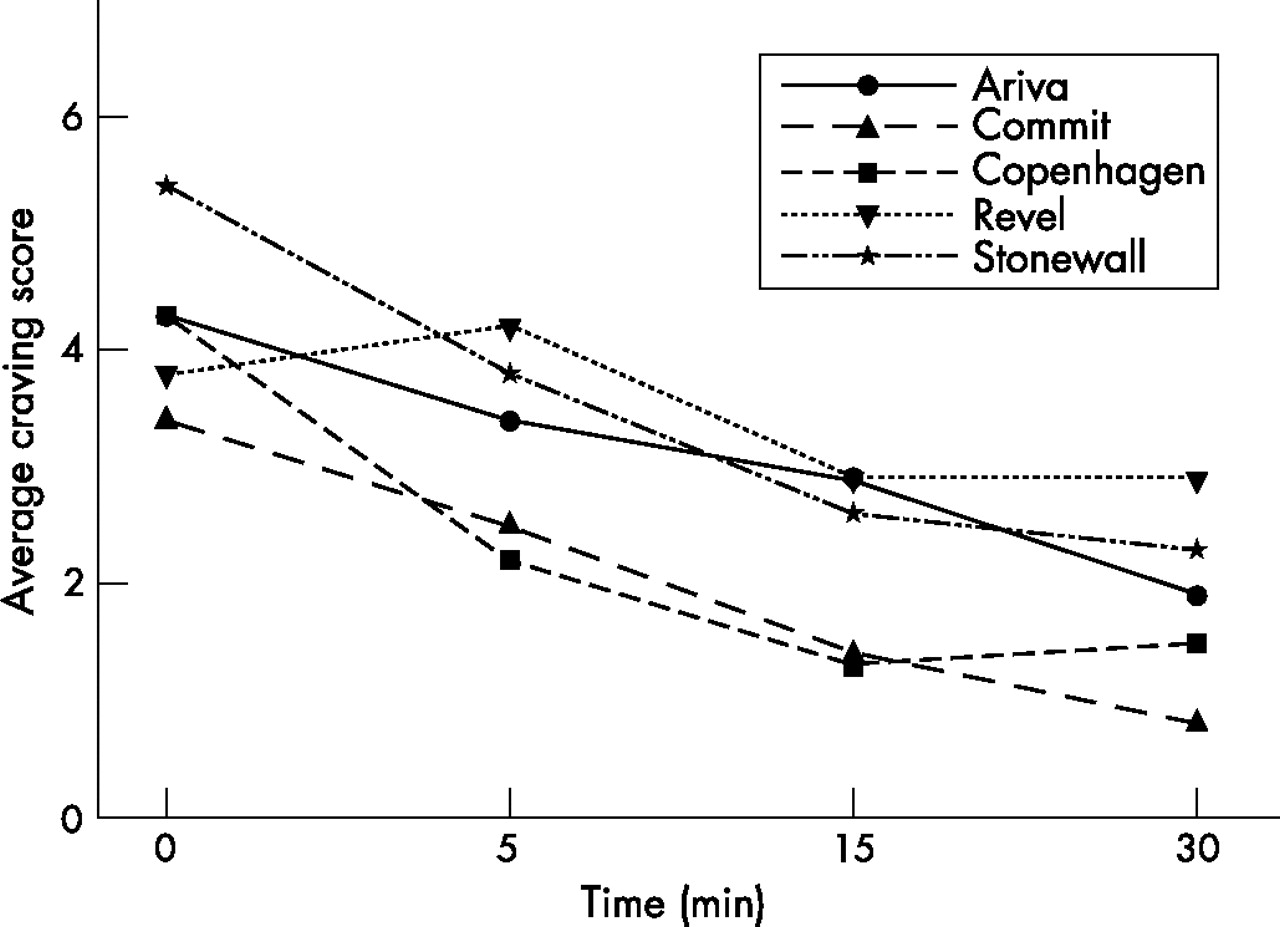
Figure 2 illustrates the time course of craving and fig 3 illustrates the time course of withdrawal symptoms during the 30 min that the products were being used. There was a significant main effect of time for both craving (p<0.001) and withdrawal (p<0.001), indicating that craving and withdrawal symptoms declined as subjects used these products. There was, however, no time×product interaction for either craving or withdrawal, indicating that there was no difference between products in the decline of withdrawal symptoms.
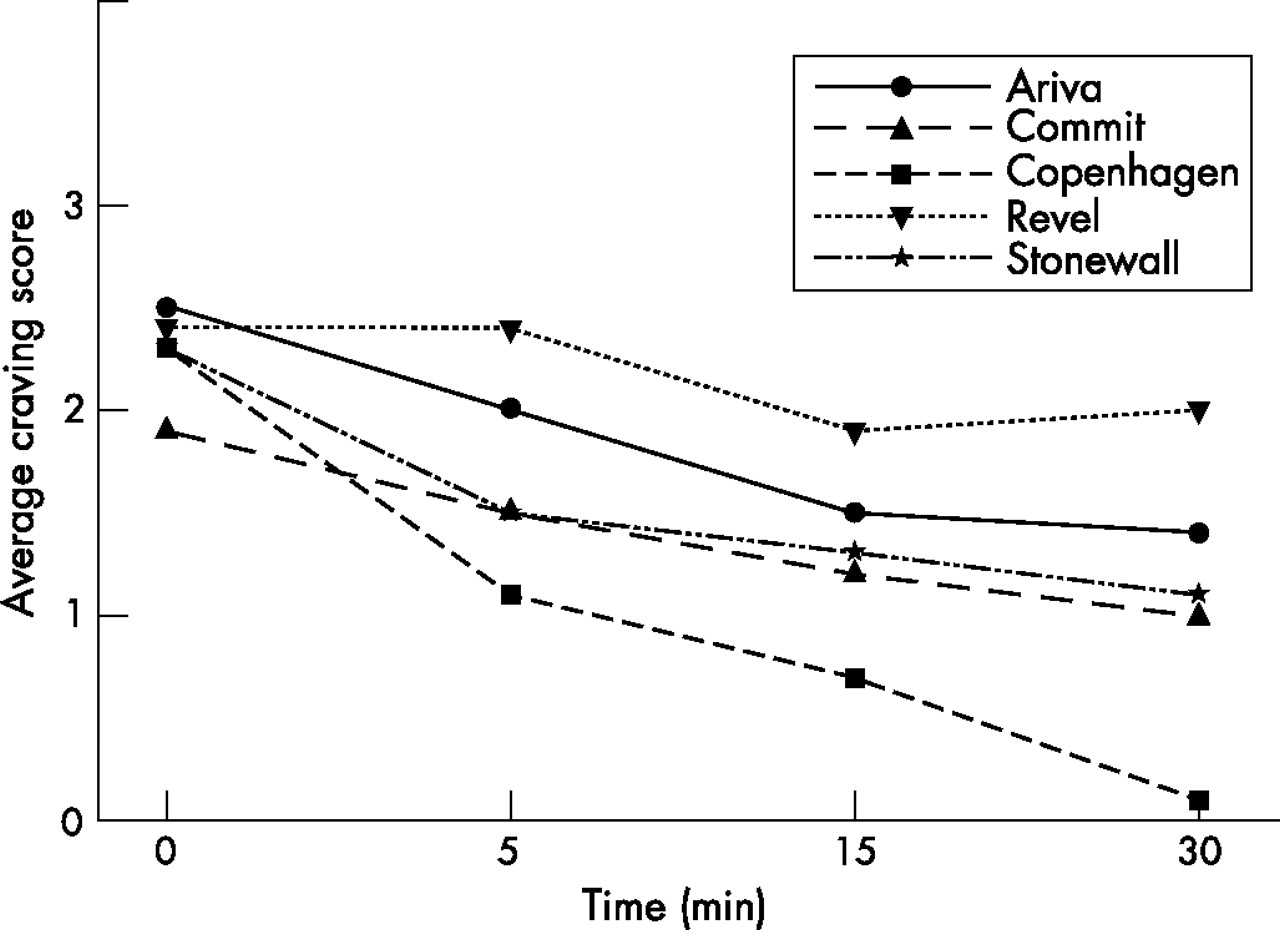
Mean craving score during use of five smokeless products.
{kind=link}
{kind=link}
{kind=link}
Mean nicotine withdrawal symptom score during use of five smokeless products.
Overall, craving during the 30 min that the product was used was significantly lower during the use of Copenhagen than during the use of any of the other four products (p<0.03). Craving during the use of Stonewall, Ariva and Commit was lower than during the use of Revel (p<0.05). No other significant differences in craving were observed between products. Withdrawal symptoms during use of Copenhagen were significantly lower than during use of Revel (p = 0.009). No other significant differences in withdrawal symptoms were observed between products. A significant (p<0.001) negative correlation (correlation coefficient = −0.494) was observed between nicotine AUC and craving score, but not between nicotine AUC and withdrawal symptoms.
Among the items assessed on the drug effects and liking questionnaire, no differences between any of the products were found in response to questions asking whether subjects (1) felt any bad effects from the study product; (2) felt alert; (3) felt relaxed; (4) felt a head rush; (5) felt a tremor in hands, arms or face; (6) felt light-headed/dizzy; (7) felt drowsy; (8) felt energetic; or (9) felt jittery. Scores when using Copenhagen were significantly higher than when using any of the other products in response to questions asking subjects (1) whether they felt any good effects from the study product (p<0.001); (2) to rate how satisfying the product was (p<0.001); (3) to rate how much they liked the study product (p<0.001); (4) to rate how much they desired the study product (p<0.001); and (5) to rate how strong the study product was (p<0.005). No significant differences in these measures were seen between any other products. Scores were significantly higher when using Copenhagen than when using either Commit (p = 0.017) or Revel (p = 0.039) when subjects were asked whether they felt a fast/pounding heart, and significantly higher than when using Commit when subjects were asked to rate whether they felt high (p = 0.016).
DISCUSSION
This study shows that there are significant differences in the nicotine pharmacokinetics and in the subjective effects of various forms of smokeless nicotine products. The use of Copenhagen resulted in the greatest exposure of nicotine and was associated with the lowest levels of craving and the highest scores on many aspects of product effects and liking. Medicinal use of nicotine resulted in greater exposure to nicotine and higher Cmax than the use of either Ariva or Revel. Medicinal nicotine was equivalent to the PREPs studied with respect to drug effects and liking measures, and nicotine-withdrawal symptoms, and resulted in lower craving scores than those observed with one of the other products studied (ie, Revel).
Considering that Copenhagen was the regular brand for all the subjects in this study, it is not surprising that use of Copenhagen was associated with the lowest levels of craving and the highest ratings of many measures of product effects and liking. Additionally, use of Copenhagen resulted in far higher concentrations of nicotine than the use of any of the other products, further explaining Copenhagen’s subjective effects. The relative rapid delivery of substantial amounts of nicotine during use of Copenhagen is consistent with that reported previously.12,21 The peak concentrations of nicotine obtained from the nicotine lozenge were similarly comparable with previous reports.22 Interestingly, two of the tobacco products studied (ie, Ariva and Revel) did not result in any sustained increase in plasma nicotine concentrations, and all three of the reduced exposure products (Ariva, Revel and Stonewall) resulted in lower maximal nicotine concentrations than the nicotine lozenge. This is consistent with our results indicating that the subjective effects from use of medicinal nicotine were either equivalent to or in the case of craving, superior to the effects reported from using the new tobacco products.
The use of nicotine replacement therapy as an aid to smokeless tobacco cessation has not been studied extensively; however, the available data suggest that at best it results in small increases in smokeless tobacco cessation rates.23 The PREPs studied do not seem to have either pharmacokinetic characteristics or subjective effects that would suggest they would be more effective than medicinal nicotine in increasing quit rates from older smokeless tobacco products (eg, moist snuff). However, the potential of PREPs to cause diseases associated with smoking or smokeless tobacco use (eg, cancer and cardiovascular disease) is largely unknown. An in vitro study assessing the amount of tobacco-specific nitrosamines in the new tobacco products has found that although levels found in these three PREPs were lower than that found in Copenhagen, there was a wide variability between products (ie, levels in Revel were higher than in either Ariva or Stonewall) and all products had higher levels than the trace amounts found in medicinal nicotine.7
Although the dosages studied are those recommended on the packaging of the products evaluated, actual use may differ substantially and probably depends on multiple factors such as cost, packaging and marketing. Overall daily exposure to nicotine will depend on the pharmacokinetic properties of these products and on the frequency and pattern of use throughout the day. Additionally, unlike medicinal nicotine, which in the US is subject to regulation by the Food and Drug Administration, tobacco products (including PREPs) do not undergo review by regulatory agencies. Marketing for the reduced exposure and spitless products has suggested that these products are safer than cigarettes and may either completely substitute for smoking or be good alternatives to smoking in areas where smoking bans preclude cigarette use.24 Since the number of cigarette smokers in the US is currently much higher than the number of smokeless tobacco users, these advertising strategies have been aimed largely at cigarette smokers rather than at users of traditional smokeless tobacco products.25 Medicinal nicotine, in the US, is approved only as an aid for complete cessation and not as an aid for harm-reduction strategies such as long-term substitution of tobacco or for acute use where smoking restrictions are imposed. Manufacturers of medicinal nicotine therefore cannot similarly advertise these agents. This disparate regulatory environment may therefore lead to differences in the marketing of these products and therefore to differences in the acceptance and use of these products.
Our study does not deal with the subjective effects of these products in cigarette users, but the pharmacokinetic characteristics of the products would make it doubtful that these products would provide greater physical satisfaction to smokers than would medicinal nicotine. Furthermore, it is unlikely that products such as Ariva or Revel would totally substitute for smoking because of the low levels of nicotine delivery. Given the unknown risks of these products, medicinal nicotine would be a more appropriate alternative for smokers unable to smoke because of smoking restrictions but wanting to reduce craving and withdrawal symptoms.
In conclusion, our study found that among regular users of smokeless tobacco, nicotine concentrations during use of Copenhagen were substantially higher than during use of any of the three new PREPs or during use of medicinal nicotine. Consequently, use of Copenhagen was associated with the lowest craving scores and the highest ratings on drug effects and liking characteristics. Among the other four products studied, medicinal nicotine resulted in higher nicotine concentrations and was equivalent to or superior to the other agents in reducing craving. Since the health risks of the new smokeless tobacco products are largely unknown, our study suggests that smokeless tobacco users or smokers seeing a safer product should be encouraged to use medicinal nicotine rather than any of the other products assessed in this study.
What this paper adds
-
New smokeless tobacco products, often marketed as potential reduced exposure products that are safer or more convenient to use than cigarettes, are being introduced into the marketplace. There is at this time, however, little information regarding the nicotine pharmacokinetics of these products or their effects on nicotine craving, nicotine withdrawal and other subjective measures of product effects or liking.
-
This study examined these measures for three of the new smokeless tobacco products (Ariva, Revel and Stonewall) and found that compared with medicinal nicotine (Commit lozenge), use of these products results in lower nicotine concentrations and in either equivalent or higher ratings on subjective measures. Since the health effects of these newer products are largely unknown, smokers or smokeless tobacco users wishing to switch to a lower-risk product should be encouraged to use medicinal nicotine.
REFERENCES
Footnotes
-
Funding: This study was supported by grant # P50DA013333 (Transdisciplinary Tobacco Use Research Center), grant # K23DA017307 and grant # M01-RR00400 (General Clinical Research Center Program).
-
Competing interests: None.