Article Text

Abstract
Objective: To determine the efficacy of biomedical risk assessment (eg, exhaled carbon monoxide (CO), or genetic susceptibility to lung cancer) as an aid for smoking cessation.
Data sources: Cochrane Tobacco Addiction Group Specialized Register, Cochrane Central Register of Controlled Trials, Medline (1966–2004) and EMBASE (1980–2004).
Study selection: Randomised controlled smoking cessation interventions using biomedical tests with at least 6 months follow-up.
Data extraction: Two reviewers independently screened all search results (titles and abstracts) for possible inclusion. Each reviewer then extracted data from the selected studies, and assessed their methodological quality based on the CONSORT (Consolidated Standards of Reporting Trials) statement criteria.
Data synthesis: Of 4049 retrieved references, eight trials were retained for data extraction and analysis. Three trials isolated the effect of exhaled CO on smoking cessation rates resulting in the following ORs and 95% CIs: 0.73 (0.38 to 1.39), 0.93 (0.62 to 1.41) and 1.18 (0.84 to 1.64). Measurement of exhaled CO and spirometry were used together in three trials, resulting in the following ORs (95% CI): 0.60 (0.25 to 1.46), 2.45 (0.73 to 8.25) and 3.50 (0.88 to 13.92). Spirometry results alone were used in one other trial with an OR (95% CI) of 1.21 (0.60 to 2.42). Ultrasonography of carotid and femoral arteries performed on light smokers gave an OR (95% CI) of 3.15 (1.06 to 9.31).
Conclusions: Scarcity and limited quality of the current evidence does not support the hypothesis that biomedical risk assessment increases smoking cessation as compared with the standard treatment.
- CO, carbon monoxide
Statistics from Altmetric.com
Despite increasing scientific knowledge about health hazards due to cigarette consumption, there is, in many countries, an increase in the prevalence of smoking among young people.1,2 The gap between knowledge and smoking cessation has been attributed, partly, to smokers’ underestimation of their personal risks of smoking-related illness.3,4
A possible strategy for increasing quit rates might be to provide a personalised feedback on the physical effects of smoking by physiological measurements. We can distinguish three different types of feedback: the first one explores biomarkers of smoking exposure (cotinine and carbon monoxide (CO)); the second one gives information on smoking-related disease risk (eg, lung cancer susceptibility according to CYP2D6 genotyping)5; and the third one depicts smoking-related harm (eg, atherosclerotic plaque and impaired lung functions).6 The rationale for such interventions is to promote risk awareness and motivation to accelerate changes in smoking-behaviour.7,8
Individual studies have provided conflicting data on the effect of physiological feedback.9–17 We aimed to review the data on smoking cessation rates from controlled trials using feedback on the physiological effects of smoking or on the genetic susceptibility to smoking-related diseases. This article is a shortened version of our Cochrane review.18
METHODS
We carried out a systematic review of the current evidence to determine the efficacy of providing smokers with personal feedback, indicating the effects of smoking or susceptibility to smoking-related illness to help them to quit. We included randomised controlled trials in which a physical measurement, such as exhaled CO measurement, spirometry or genetic testing, was used to increase the motivation to quit. We excluded trials in which the effect of biological measurements was confounded by other components (eg, intensive counselling) in the active intervention. We used the most conservative measure of quitting (biochemically validated smoking cessation, when available) at the longest follow-up (at least 6 months), and considered the participants lost to follow-up as continuing smokers.
We searched the Cochrane Tobacco Addiction Group Specialized Register, which includes searches of electronic databases including Medline, EMBASE, PsycINFO and Science Citation Index, and abstracts from the Society for Research on Nicotine and Tobacco and World Tobacco or Health conferences. We conducted additional searches of the Central Register of Controlled Trials, Medline (1996–2004) and EMBASE (1980–2004) for any of the keywords related to the following topics in titles, abstracts or indexing fields: patient education, patient compliance, persuasive communication, spirometry, respiratory function, bronchospirometry, carbon monoxide, forced expiratory flow rates, obstructive lung diseases, genetic testing and genetic susceptibility. Generic terms like “counselling”, “biomarker” or “feedback” were also used to be inclusive of any type of biomedical risk assessment. This search was combined with smoking-related terms and trial design terms.
Two reviewers independently screened all search results (titles and abstracts) for possible inclusion or to use as useful background. They selected studies for full-text assessment if retained by at least one of the reviewers. Each reviewer then extracted data from the selected studies, and assessed their methodological quality (eg, adequacy of the randomisation process or concealment of allocation) based on the CONSORT (Consolidated Standards of Reporting Trials) statement criteria.19 We converted the study results into odds ratios (ORs) with 95% CIs. An OR >1 favours the intervention group. If it seemed appropriate, the results were pooled using a Maentel–Haenszel fixed-effects model.
RESULTS
We identified 22 trials for possible inclusion out of 4049 references. Eleven studies were excluded because the effect of biomedical risk assessment could not be isolated,20–30 one because smoking cessation was not considered as an outcome,31 one because the biomedical risk assessment was not carried out on the smoker himself but on his or her children32 and one because the full-text article could not be found.33 One of the excluded trials28 generated two reports.28,34
We therefore analysed data from eight trials (table 1). One of them5 tested two interventions (CO measurement and the combination of the latter with feedback about genetic susceptibility), giving rise to three possible comparisons of effectiveness. Three trials tested the effect of exhaled CO measurements alone,5,35,36 three trials tested the combination of exhaled CO measurement and spirometry,37–39 one trial tested the effect of CO and feedback about genetic susceptibility,5 one trial tested spirometry alone,40 one trial tested the effect of undergoing an ultrasonography of carotid and femoral arteries with photographic demonstration of atherosclerotic plaques when present41 and one trial tested feedback about genetic susceptibility to lung cancer.5 The mean number of cigarettes smoked per day varied between 11.9 and 29.2 and was highest in the trials set in a “smoking clinic”.39
Characteristics of included studies
Only one of the eight trials reported an adequate randomisation procedure.40 Only three studies explicitly mentioned that assessors were blinded to allocation at the time of outcome determination.37,38,41 Only one study proposed a formal estimation of sample size before recruitment.38 Biochemical validation of smoking cessation was adequately used in four studies.36,37,39,40 Participation rates (ie, the proportion of those approached who agreed to take part in the trial) were seldom recorded. In two studies,5,39 it was not possible to determine the initial allocation of the participants who were subsequently lost to follow-up, and analysis had to be performed per protocol.
Figure 1 shows the ORs and 95% CIs from the two trials using exhaled CO in a primary care setting as a way to motivate smokers to quit.35,36 These two studies were similar enough in terms of recruitment, intervention and setting to allow the pooling of data. χ2 test did not show evidence for significant heterogeneity. There was no evidence of a significant benefit from these pooled studies (Mantel–Haenszel fixed-effect OR 1.07, 95% CI 0.83 to 1.39).
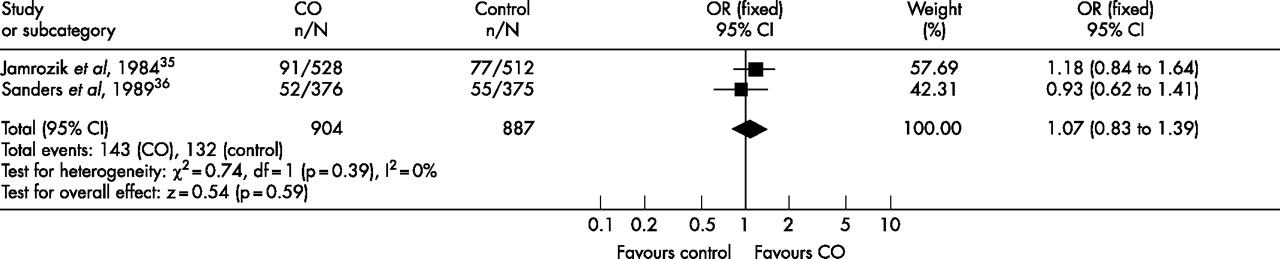
Individual and pooled ORs and 95% CIs from the two trials using exhaled carbon monoxide (CO) in a primary care setting.
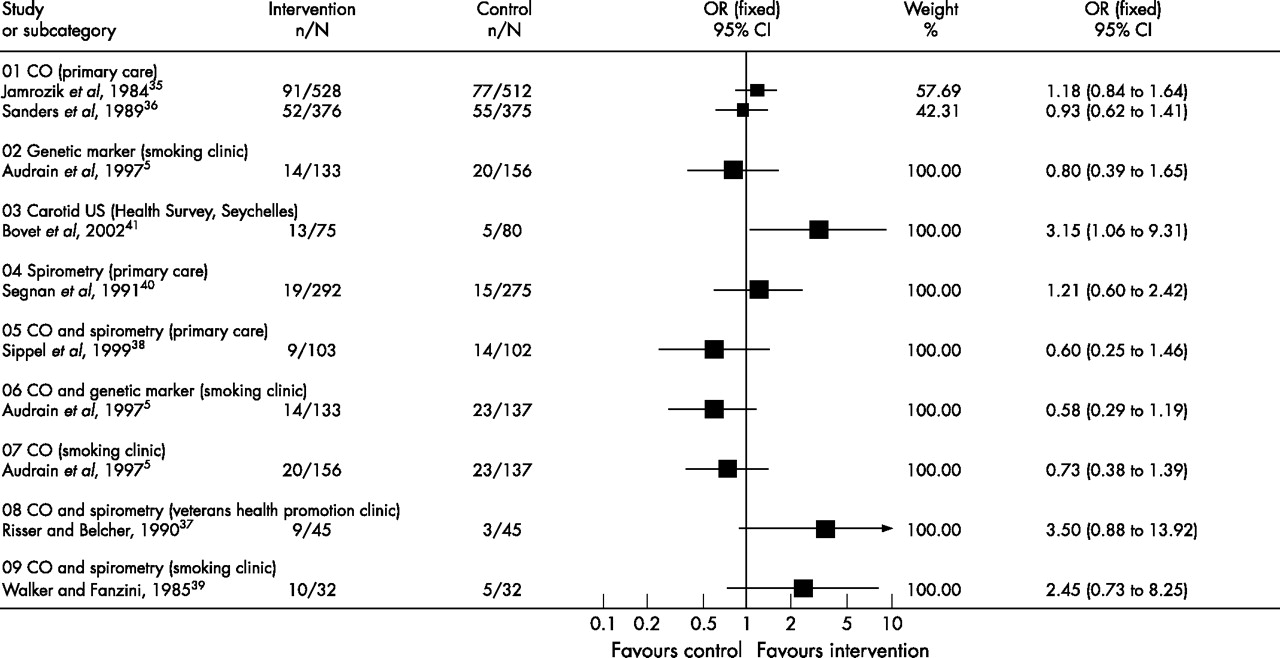
Figure 2 shows the individual ORs and 95% CIs from all the included interventions. Three studies isolated the effect of exhaled CO measurement on smoking cessation rate5,35,36 with ORs (95% CI) of 0.73 ( 0.38 to 1.39), 1.18 (0.84 to 1.64) and 0.93 (0.62 to 1.41), respectively. Exhaled CO measurement and spirometry were used together in three trials37–39 with ORs (95% CI) of 3.50 (0.88 to 13.92), 0.60 (0.25 to 1.46) and 2.45 (0.73 to 8.25), respectively. We did not pool these studies because of heterogeneous settings that would preclude the drawing of clinically relevant conclusions. Spirometry results were used in one primary care-based trial40 with an OR (95% CI) of 1.21 (0.60 to 2.42). One trial5 used both genetic susceptibility to lung cancer alone with an OR (95% CI) of 0.80 (0.39 to 1.65), as well as genetic susceptibility to lung cancer combined with exhaled CO measurement with an OR (95% CI) of 0.58 (0.29 to 1.19). Finally, ultrasonography of carotid and femoral arteries was used in one trial41 with an OR (95% CI) of 3.15 (1.06 to 9.31). This study was conducted among light smokers (average 10–12 cigarettes a day).

{kind=link}
{kind=link}
Individual ORs and 95% CIs from all included interventions.
DISCUSSION
Owing to the scarcity of evidence of sufficient quality, we could make no definitive statements about the effectiveness of biomedical risk assessment as an aid for smoking cessation. Existing evidence of lower quality does not, however, support the hypothesis that biomedical risk assessment increases smoking cessation as compared with the standard treatment.
Only two studies were similar enough in terms of recruitment, setting and intervention to allow pooling of data and meta-analysis. Their combined results further tended towards the null hypothesis. The external validity of the only study with a statistically significant positive OR41 can be questioned as the sample was made up predominantly of male light smokers (average 10–12 cigarettes a day).
Other studies identified by our search strategy did not isolate the specific effect of biomedical feedback.20–30 Two of these studies27,28 demonstrated an OR significantly favouring the intervention group rather than the control group. Demonstration of smokers’ child’s exposure to environmental tobacco smoke by measuring the child’s urinary cotinine level was used in another trial32 with an OR (95% CI) of 0.15 ( 0.01 to 2.89). We excluded this study from our analysis, because, it seemed to us that providing biomarker feedback about someone else’s health (even one’s own children) would act differently and may not contribute to counteracting the hypothesised personal optimistic bias.3,4 Smoking cessation was, moreover, documented as a secondary outcome in this study, as the primary outcome was a smoking ban in the home. In any event, this trial did not show a positive effect; the study had low power to detect an effect and its quality was limited. One study identified by McClure42 as “in press” seems never to have been published,43 and several attempts to contact the authors failed to provide us with more detailed information.
An earlier non-systematic review was conducted on the use of biomarkers in smoking cessation.42 The aim of this work was to review the theoretical rationale and the empirical evidence regarding this practice. Focus was, therefore, not specifically directed at the assessment of the efficacy of biomarker feedback as a way to increase smoking cessation. Therefore, the review included non-randomised trials,13,44–46 trials providing multicomponent interventions that precluded the isolation of the specific effect of biomarkers feedback,9,11,34 trials comparing the effect of abnormal test results versus normal test results rather than test versus no tests,12 and trials reporting outcomes other than smoking cessation. Four studies mentioned by McClure were also retained in our review.5,35,37,39 We identified four more trials for our review.36,38,40,41 When focusing on efficacy data, McClure concluded that biomarkers feedback may enhance the likelihood of cessation, because a trend for increased abstinence was found in three randomised trials.37,39,43 The fact that two of these trials37,39 are subject to major methodological limitations (small samples, inadequate randomisation procedures), and that the report of Hoffman et al43 remains unpublished, calls for great caution in drawing such conclusions.
What is already known on this topic
-
Feedback on biomedical characteristics indicating effects of smoking, or susceptibility to smoking-related illness, has been advocated to help smokers to quit.
What this study adds
-
Due to the scarcity of evidence of sufficient quality, we could make no definitive statements about the effectiveness of biomedical risk assessment as an aid for smoking cessation.
-
Existing evidence of lower quality does not, however, support the hypothesis that biomedical risk assessment increases smoking cessation as compared with the standard treatment.
-
The methodological quality of trials exploring this research question needs to improve substantially.
In most of the studies included in the current review, the biomedical testing component was added to intensive quit-smoking sessions, with counselling lasting up to 60 min and completed by written material and reinforcement sessions or follow-up telephone calls. The incremental effect of biomedical risk assessment might have been diluted by the high intensity of the standard care used. It is also possible that the changes in motivational stages induced by biomedical risk assessment are too subtle to be characterised as directly leading to a successful quit attempt.47 Another possible explanation for the absence of effectiveness of biomedical risk assessment provided in addition to counselling could be the potentially counterproductive effect of communicating normal results to smokers. Only two included studies provided some insight about smoking cessation rates according to test results. Sippel et al38 did not find any correlation between smoking cessation and abnormal spirometry results, whereas Bovet et al41 found a non-significant lower smoking cessation rate among participants without plaques at ultrasonography compared with participants who did not undergo ultrasonography. Similarly, whether the presence of smoking-related symptoms may modify the effect of biomedical feedback is unknown. These particular questions, and the way to communicate normal test results should be explored in future trials.
Acknowledgments
We thank Olivier Terraz of the Institute for Social and Preventive Medicine, University of Lausanne, for his assistance in retrieving and selecting references identified by our search strategy, and Alvine Bissery of the same institution for her statistical expertise. We also thank Jon Britton and Jonathan Foulds for their helpful suggestions on the protocol, and Andy McEwen and Lion Shahab for constructive comments on the earlier drafts of this review.
REFERENCES
Footnotes
-
Funding: This study was funded by the Clinical Epidemiology Center (CEPIC), University of Lausanne, Switzerland
-
Competing interests: JC was the coauthor of one of the studies included in the review (
) -
RB, BB and JC designed the study, reviewed the studies identified and checked the data. YM reviewed the studies identified and checked the data. RB and YM wrote the first draft of the article, and BB and JC provided substantive subsequent contributions. RB is the guarantor.
-
The results of a Cochrane Review can be interpreted differently, depending on people’s perspectives and circumstances. Please consider the conclusions presented carefully. They are the opinions of review authors, and are not necessarily shared by The Cochrane Collaboration.