Article Text

Abstract
Objective: To estimate the incremental cost-effectiveness ratio of a structured community pharmacist-based smoking cessation programme compared with usual care.
Design: A cost-effectiveness study using a healthcare system perspective
Population: Two simulated cohorts of smokers: male and female aged 40, 50 and 60 years who regularly smoke 10–20 cigarettes per day.
Intervention and comparator: A structured community pharmacist-based smoking cessation (CPSC) programme compared to usual care.
Main outcome measure: Cost per life year gained (LYG) attributable to the smoking cessation programme.
Results: The CPSC programme results in cost savings of 17 503.53 baht (£250; €325; $500) to the health system and life year gains of 0.18 years for men and; costs savings of 21 499.75 baht (£307; €399; $614) and life year gains of 0.24 years for women. A series of sensitivity analyses demonstrate that both cost savings and life year gains are sensitive to variations in the discount rate and the long-term smoking quit rate associated with the intervention.
Conclusion: From the perspective of the health system, the CPSC programme yields cost savings and life year gains. This finding provides important information for health policy decision-makers when determining the magnitude of resources to be allocated to smoking cessation service in community pharmacy.
Statistics from Altmetric.com
Smoking is associated with increases in morbidity, mortality and healthcare costs worldwide.1–3 It has also been recognised as an important cause of deaths and chronic diseases in Thailand. Annually, approximately 52 000 residents in Thailand die from smoking-related diseases.4 5 Over 79 of lung cancer and 88 of chronic obstructive pulmonary diseases are caused by smoking.6 In 1999, it was estimated that $6 million or 0.1 of Thai total healthcare expenditure was incurred for management of smoking-related diseases.7
Smoking cessation has been accepted as a crucial strategy in tobacco control because such intervention reduces the incidence and impact of a range of costly chronic diseases, improves health-related quality of life and yields savings in healthcare cost.8–12 Evidence has consistently demonstrated the effectiveness of various health professional-based smoking cessation interventions.13–19 However, in Thailand, a recent survey in 2005 revealed that less than 70 of smoking cessation clinics still provided services for Thai smokers who seek professional help.20
A community pharmacy provides an excellent setting in which to provide a smoking cessation programme, as the pharmacy would have regular contact with residents of the area.21 In Thailand, more than 1000 community pharmacists were trained and provide smoking cessation services.22 Based on a recent review of the literature, community pharmacist-based smoking cessation programmes have been shown to be cost effective.23–32 However, several cost-effectiveness studies30–32 calculated life years saved for successful quitters’ estimates based on US population estimates.33 We believe that such methods and estimates may not be applicable to the long-term outcomes of smoking cessation programmes in Thailand. Strictly speaking, these studies were conducted in countries that are different from Thailand in terms of life expectancy of population, healthcare system and medical costs of smoking-related diseases. Therefore, cost-effectiveness evidence of smoking cessation programmes in Thailand is still needed. The main purpose of this study is to determine the incremental cost-effectiveness ratio of a structured community pharmacist-based smoking cessation (CPSC) programme compared to a usual care in order to assist health policy decision-makers in determining whether resources should be allocated to support community pharmacist-based smoking cessation services in Thailand.
METHODS
Overall description
This analysis compares a structured CPSC programme and usual care. The CPSC programme includes systematic identification and documentation of smoking status; provision of a personalised and supportive advice on smoking cessation; an assessment a smoker’s interest in quitting and level of nicotine dependence; and the provision of appropriate therapy with self-help materials and seven scheduled 10-minute follow-up visits. Usual care consists of discussion on smoking status, assessment of motivation and nicotine dependence, provision of brief advice and support as well as provision of therapy without follow-up care.
We use standard techniques in economic evaluation and decision analysis in order to assess the costs and effectiveness of a CPSC programme. A decision tree is used to depict the consequences of smoking cessation for those who continuously abstain from smoking for 12 months. These long-term outcomes are derived by applying a Markov model of disease state transition to a simulated cohort of Thai residents. The Markov model links long-term smoking cessation to reductions in the risk of developing various important smoking related diseases comprising chronic obstructive pulmonary disease (COPD), lung cancer, stroke and cardiovascular diseases. In the base-case analysis, we have used a hypothetical cohort of Thai men and women aged 40 years, who regularly smoke 10–20 cigarettes per day. We use this base population because it is typical of Thai smokers.34
The healthcare system perspective is used in our analysis; hence only direct medical costs are included. The cost-effectiveness ratio is expressed as the incremental costs per life year saved. In this study, all analyses are performed using Microsoft Office Excel 2003. The Markov model simulates a hypothetical cohort according to age, sex and smoking status. All participants begin in a healthy state before transition to other health states. The model uses a cycle length of one year. Transitional probabilities are conditional on age, sex and smoking status. The absorbing state is death. The time horizon used in this study is the lifetime for a Thai resident.
Likelihood of events
Event probabilities used in the model are shown in table 1. The likelihood of successful quitting was derived from a systematic review of randomised controlled trial data that assessed individuals who had stopped smoking for 12 continuous months.35 The reported continuous quit rate was 14.3 in the CPSC group and 2.7 in the usual care group. Relapse rate and natural quit rate were not considered in our analysis because the existing cost-effectiveness study indicated they had a slight effect on the results.30 In this study, we assumed that smokers who are abstinent at one year remain abstinent for life.
Risks of developing smoking-related diseases were based on international published studies. Based on a 10-year prospective cohort study,36 the annual risk of COPD for smokers and ex-smokers was 1.22 and 0.34, respectively. The risk of lung cancer, derived from an 8-year multi-ethnic cohort study,37 was 0.24 for smokers and 0.08 for ex-smokers. We estimated the annual probabilities of developing coronary heart diseases (CHD) and stroke from the Framingham’s risk equation as performed in Johannesson et al.38 The equation yields the risk of cardiovascular disease using blood pressure and total cholesterol levels for Thai residents as derived from the InterASIA study.39 We adopted a method developed by Johansson et al40 to estimate transition probabilities for each sub-CHD health state. The transition probabilities for CHD were based on the proportion of the distribution of each health state within CHD (acute myocardial infarction, myocardial infarction unrecognised, chronic heart failure, angina and sudden death).
Age-specific mortality for the Thai population6 was used as the transition probability from a healthy state to death. Probabilities of dying from smoking-related diseases were based on estimates in the Thai and international literature. In order to calculate the mortality rate from COPD, the age-specific Thai mortality rate was multiplied by the hazard ratio (or relative risk) of dying from COPD.41 The lung cancer mortality rate was based on data from a 5-year cohort study42 that followed lung cancer patients at 14 large hospitals in Thailand. The annual mortality rate for diseases within CHD were based on mortality estimates derived from the Framingham’s equation using a similar approach to that used by Johanesson.38
Costs
The total cost of smoking cessation interventions by community pharmacists were based on the summation of the pharmacists’ training costs, the pharmacists’ fee and the cost of medications. Cost of the pharmacists’ training course was acquired from the Thai Pharmacy Network for Tobacco Control (PNTC).22 Pharmacists’ fees were taken from a costing study of 40 Thai community pharmacies conducted by Nantamongkol et al.43 The cost of drugs aiding smoking cessation were based on estimates offered by the Drug and Medical Supply Information Center (DMSIC).44
The disease-specific treatment costs were derived from recently published Thai studies. The cost of lung cancer was taken from estimates of the economic cost of lung cancer at Siriraj Hospital and the National Cancer Institute.45 Lung cancer costs were 53 980.96 baht per person per year. The cost of COPD was derived from the average direct cost of COPD at Ramathibodi Hospital over the period July 2000–June 2001.46 47 Such cost estimates were 59 721.30 baht per person per year. The cost of acute myocardial infraction, the cost of chronic heart failure and the cost of angina were obtained from a study concerning diabetes complication costs from Buddhachinaraj Hospital database.48 In our study, cost of unrecognised myocardial infarction was assumed to be zero. The annual cost of acute myocardial infarction, angina and chronic heart failure were 31 911, 22 892 and 29 738 baht per person per year, respectively. Cost of stroke was taken from the cost for patients receiving care at Prasat Neurological Institute during 1999.49 This annual cost of stroke was 50 331.50 baht per person per year. All costs in this study were adjusted to 2005 Thai baht using the medical and personal care consumer price index for Thailand 1994–2005.50 The exchange rate used to convert Thai baht to US dollars is 35 baht per US dollar.
Analysis
The incremental cost-effectiveness ratio was estimated to determine whether the benefits derived from the CPSC programme, measured by life years gained, offered value for money. This intervention programme was compared to usual care. In the base-case analysis, a discount rate of 3 was used to adjust both costs and outcomes using standard discounting conventions.51–54
Sensitivity analysis using Monte Carlo simulation was conducted in order to assess the effects of varying assumptions on the study findings. The decision analysis model was simulated on 1000 iterations. A cost-effectiveness acceptability curve was plotted based on the results derived form the Monte Carlo simulation. In addition, a series of one-way sensitivity analyses, two-way sensitivity analysis and threshold analyses were also undertaken to investigate the effects of altering parameters including discount rate, continuous abstinence rate, cost of smoking cessation programme and cost of smoking-related diseases. Discount rates on cost and outcome of 0, 3, 5 and 10 were used. Quit rates were varied by their 95 confidence interval, and intervention costs were altered from low to high estimates of resources use.
Main assumptions
There were four main assumptions that warrant emphasis: (1) The risk of smoking related diseases were uniform over time. (2) Smokers will only experience, at most, one disease over their lifetime. (3) In each cycle of the Markov model, the transition to next health state is irreversible. (4) Smokers will receive only one smoking cessation programme during their lifetime.
RESULTS
Costs and outcomes
In the base-case analysis, compared with the usual care, the CPSC programme results in cost savings of 17 503.54 baht ($500) and 21 499.75 baht ($614) for men and women, respectively. Furthermore, CPSC also leads to increases in life expectancy of 0.181 years for men and 0.244 years for women. Thus, the CPSC programme rather than usual care results in cost savings and gains in life years. The estimated incremental cost and life year gained for participants aged 40, 50 and 60 years are depicted in table 2.
Sensitivity analysis
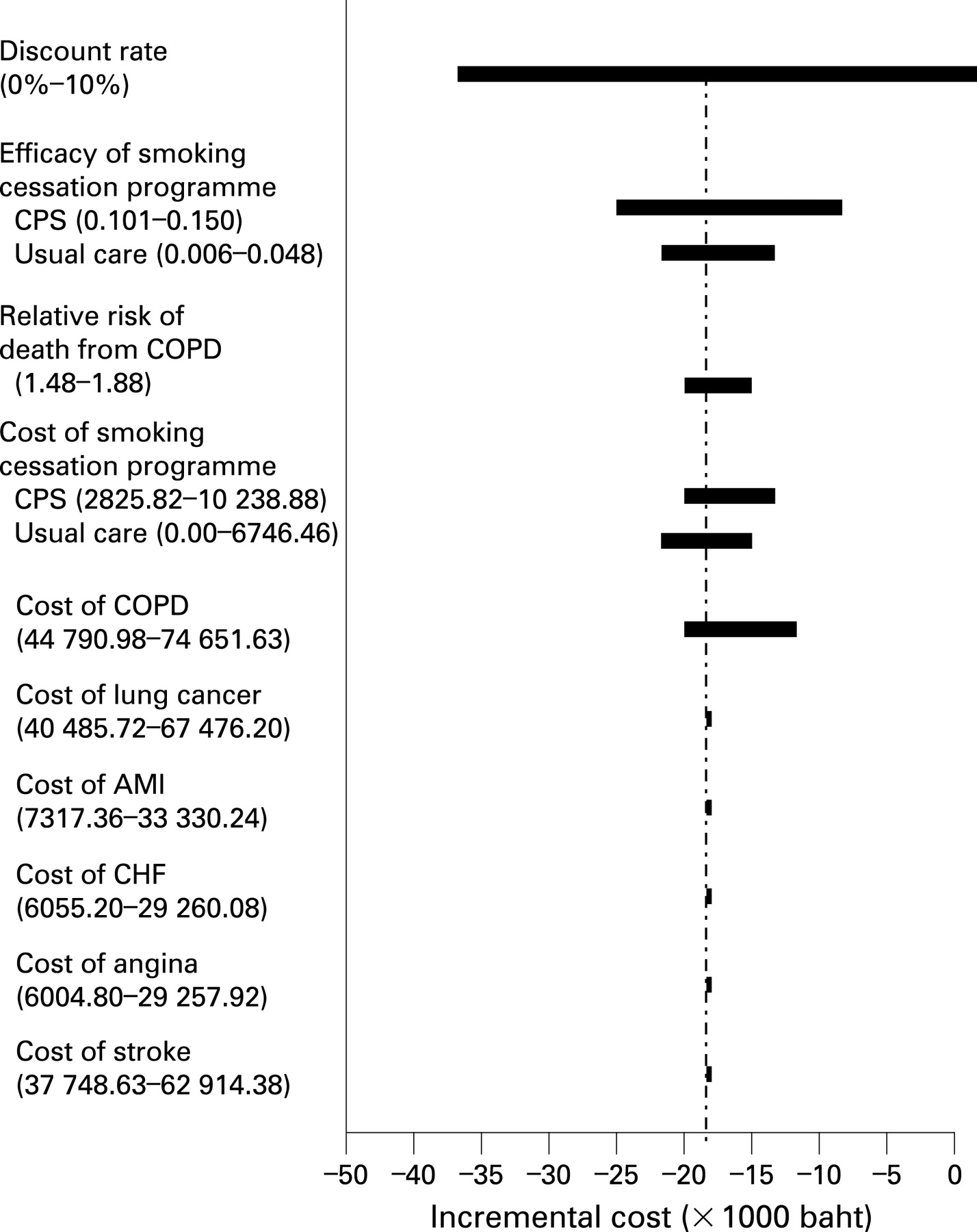
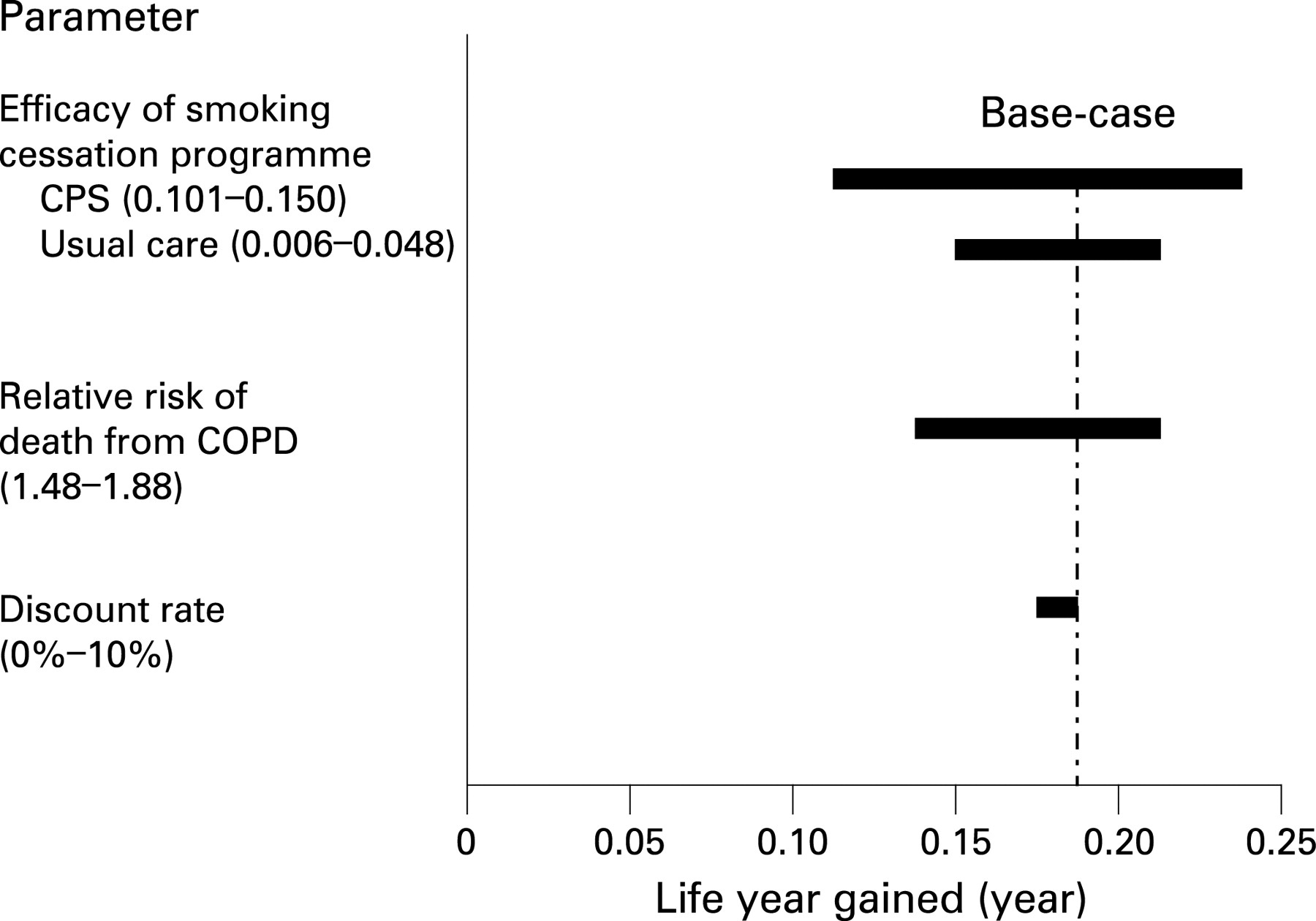
A series of one-way analyses, based on a 40 year old male smoker, demonstrated that incremental costs were influenced by the discount rate and the 12-month abstinence rate (fig 1). Incremental life expectancy was sensitive to the 12-month abstinence rate (fig 2). Using the 95 CI for the 12-month abstinence rate, total cost savings and life expectancy gains ranged from 9827.17 to 24 919.09 baht and from 0.115 to 0.246 years, respectively.


In the two-way sensitivity analyses, if the long-term quit rate resulting from the CPSC programme was more than usual care by 0.02 or greater, cost savings were maintained. The CPSC programme continues to result in life years gained as long as long-term quit rate from the CPSC programme is more than the quit rate from usual care by 0.001 or greater. In 84 of the 1000 Monte Carlo simulations, the CPSC programme led to cost savings and life years gained (fig 3). Moreover, the results of the probabilistic sensitivity analysis are also presented by cost-effectiveness acceptability curve (CEAC) (fig 4). The CEAC indicates the probability that a community pharmacist-based smoking cessation programme is cost effective compared with a usual care, over a range of the decision-maker’s willingness to pay or maximum acceptable ceiling ratio (λ). If λ is 315 000 baht per life year gained, which is three times of Thai GDP per capita, the probability that a structured CPSC programme is cost effective is found to be 0.996.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The community pharmacist-based smoking cessation (CPSC) programme results in gains in life expectancy and cost saving. These findings are important pieces of information to aid policy-makers in planning budget allocations to support smoking cessation services for Thai smokers. This study is the first conducted to estimate the long-term effects of CPSC using a disease based model for Thailand.
Our approach is different from previous cost-effectiveness studies of CPSC interventions.30–32 Those studies calculated the expected increase in life expectancy associated with smoking cessation from the US published data.33 Unfortunately, that approach is not applicable to Thailand as basic demographic and socioeconomic characteristics of the Thai population deviate from those jurisdictions.
Our findings suggest that the CPSC programme is cost saving. This is because of the lower cost of the programme compared to the cost of smoking-related diseases. In the near future, if a smoking cessation training programme for community pharmacists is included in the curriculum for Thai pharmacy students, the training programme costs would be reduced substantially. Therefore, CPSC programmes should result in even more cost saving.
Our cost-saving results are quite different from those found in the current literature.30–32 Those studies reported CPSC programmes were not cost saving; however, the cost increase was relatively small compared to the gains in life years. The cost-saving findings were absent in these studies because they did not take into account the costs of smoking-related diseases. There has been continuing debate regarding the difference in lifetime medical costs between smokers and non-smokers. Some studies55–57 have indicated that lifetime costs of smokers were not different from non-smokers while others provide counter-arguments because of the greater life expectancy of non-smokers.7 58 Instead of adopting either of these assumptions, we included the cost of smoking-related diseases in our model because excluding these costs led to a significant underestimate of the benefits of smoking cessation.
Our findings are consistent with the results reported in cost-effectiveness studies of other smoking cessation interventions using disease-based approach. Feenstra et al59 reported the one-year implementation of minimal general practitioners counselling in the Dutch population would save healthcare costs for smoking-related diseases by €5700 and yield 1.4 life years comparing to current practice. Johansson et al60 estimated that a “quit-and-win” contest for mothers of pre-school children provided cost-savings of Swedish krona (SEK) 20 000–35 000 per quitter and offered gains of 0.42 to 0.53 life years. In addition, the Health and Economic Consequence of Smoking model (HECOS)61 illustrated quitting by three standardised interventions in the United Kingdom, pharmacological treatment, general practitioner advice and group therapy resulted in reduction in cost of smoking related diseases of £4.5 million to £36 million.
Because of the uncertainty of data used in the model, we explore possible variability in our outcomes using sensitivity analyses. The cost savings were sensitive to both the discount rate and the cessation rate while gains in life years were sensitive to the cessation rate, relative risk of death from COPD and the discount rate. These influential parameters are similar to what has been reported in the existing cost-effectiveness literature concerning smoking cessation programmes provided by community pharmacists.30–32 Furthermore, we also assess the uncertainty of combination parameters on our findings using probabilistic sensitivity analysis (PSA), which offers a complete picture of the impact of parameter uncertainty on the findings. The cost-effectiveness acceptability curves suggest that the probability that the CPSC programme is cost saving compared to usual care is approximately 0.84.
Our study has some limitations that should be addressed. First, owing to the limitation of epidemiological and utility parameters in Thailand, we considered only tobacco-related diseases that had the highest prevalence among smokers6 and had significant impacts in Thailand, although smoking causes a number of serious diseases. In addition, we estimated long-term effects of the smoking cessation programme in terms of life years saved rather than quality adjusted life year (QALYs). Second, in our analysis, relapse rate and natural quit rate were not considered because of the scarcity of these data in Thailand. Moreover, the existing cost-effectiveness study also indicated that both relapse rate and natural quit rate had a slight effect on the cost-effective results.30 Third, since we obtained cost parameters from various references in the existing Thai literature, it might be argued that different sources of costs data may lead to inaccurate costs estimation. Nevertheless, all cost parameters were obtained from the best available studies. Fourth, owing to scarcity and difficulty in accessing data, the risk of CHD and stroke were estimated from the Framingham risk equation38 while the one-year transition probability of COPD was calculated from the 10-year cumulative incidence in the Swedish population.36 Furthermore, the likelihood of lung cancer was derived from an eight-year cumulative risk of lung cancer in a Japanese-American cohort study.37 With regard to the background mortality, we did not adjust the age-specific mortality for the inclusion of cardiovascular, lung cancer and COPD deaths. We used Thai age-specific mortality rate to estimate probability of death of the healthy population. It should be noted that using unadjusted background mortality rate from smoking-related diseases may lead to overestimation of the probability of death among the population. However, this lack of adjustment is unlikely to change the overall point estimate much as it is applied to both cohorts: smokers and quitters. For risk of death from COPD, risk of death from CHD and stroke, these estimates were drawn from an international study.38 It might be argued that evidence from international studies cannot accurately depict the impact of smoking cessation for the Thai population. Nevertheless, we believe that all of our input parameters are derived from the best available sources of information. In future, should there be improved evidence regarding smoking-related morbidity or mortality, this model is amenable to the incorporation of such data.
Our study shows the cost savings and gains in life years resulting from a CPSC programme. These findings are very favourable and could be interpreted by policy-makers as paramount evidence to strongly endorse the decision to support the programme; however, most of the decision-making cannot generally be based solely on a cost-effectiveness analysis. Before deciding to reimburse smoking cessation programmes, decision-makers may be interested in knowing other important issues about the characteristics of the populations that benefit from the programme. In addition, it is crucial to review the existing reimbursement system for smoking cessation programme in other countries in order to develop appropriate systems for introduction into the Thai context. Moreover, policy-makers may need to know how the implementation of reimbursement affects behaviour of healthcare professionals, care recipients as well as to gauge the impact on the total healthcare budget. Lastly, before policy-makers decide to reimburse for this cessation service, there might be a need to develop the standards for quality control of the provision of smoking cessation services in community pharmacies.
CONCLUSION
In summary, a CPSC programme yields cost savings and provides life year gains. In future, if this programme were supported by the government, it will allow a number of Thai smokers with an interest in quitting to have access to a smoking cessation programme that would help them to become a successful quitter.
What this paper adds
-
A community pharmacist-based smoking cessation (CPSC) programme is an effective way to increase access to cessation assistance for smokers interested in quitting. Several cost-effectiveness studies were conducted, but none of them focused on developing countries. In addition, the life expectancy calculated in all studies was based US population estimates; these were not applicable to Thai population.
-
This cost-effectiveness study found that the CPSC programme resulted in gains in life expectancy and cost savings. These findings provide the best Thai-specific data available for health policy decision-makers as they plan allocation of resources for smoking cessation.
Acknowledgments
We thank Dr Piyarat Nimpitakpong and Dr Peter C Coyte for their critical comments of this manuscript. In addition, we acknowledge the technical assistance of Dr Chuanchom Thananitisak during the initial stage of this research project.
REFERENCES
Footnotes
-
Funding: This study was supported, in part, by a grant from the Thailand Research Fund and Thai Pharmacy Network for Tobacco Control (through the Thai Health Promotion Foundation).
-
Competing interests: None.