Article Text

Abstract
Context: Motor vehicles represent important microenvironments for exposure to secondhand smoke (SHS). While some countries and cities have banned smoking in cars with children present, more data are needed to develop the evidence base on SHS exposure levels in motor vehicles to inform policy and education practices aimed at supporting smoke-free motor vehicles when passengers are present.
Objective: To assess exposure to secondhand tobacco smoke in motor vehicles using passive airborne nicotine samplers.
Methods: 17 smokers and five non-smokers who commute to and from work in their own vehicle participated. Two passive airborne nicotine samplers were placed in each vehicle for a 24-hour period, one at the front passenger seat headrest and the other in the back seat behind the driver. At the end of the sampling period, airborne nicotine was analysed by gas chromatography.
Results: Median (IQR) air nicotine concentrations in smokers’ vehicles were 9.6 μg/m3 (5.3–25.5) compared to non-detectable concentrations in non-smokers’ vehicles. After adjustment for vehicle size, window opening, air conditioning and sampling time, there was a 1.96-fold increase (95% CI 1.43 to 2.67) in air nicotine concentrations per cigarette smoked.
Conclusions: Air nicotine concentrations in motor vehicles were much higher than air nicotine concentrations generally measured in public or private indoor places, and even higher than concentrations measured in restaurants and bars. These high levels of exposure to SHS support the need for education measures and legislation that regulate smoking in motor vehicles when passengers, especially children, are present.
Statistics from Altmetric.com
Involuntary exposure to secondhand smoke accounts for thousands of cases of respiratory, cardiovascular and cancer deaths in the United States each year.1 To prevent mortality and morbidity caused by secondhand smoke, smoke-free regulations banning smoking in public places are being passed in cities and countries around the world.2 3 Public education is also being implemented to discourage smoking inside the home.4 Indeed, households enforcing smoke-free home rules in the US increased from 43% in 1992–3 to 72% in 2003.5 With commuting lengths increasing and the importance of car pooling, it is vital to consider the health risks of exposure to secondhand smoke to motor vehicle passengers who travel with a smoker.
While scarce data quantifying secondhand smoke exposure levels in cars exist,6 7 8 9 motor vehicles represent important microenvironments for secondhand smoke exposure—first, because there is no risk-free level of secondhand smoke exposure1; second, because owing to the confined space within a motor vehicle, tobacco smoke concentrations increase rapidly10 posing serious health risks for passengers who are repeatedly exposed. Epidemiological and mechanistic studies have shown that short-term secondhand smoke exposure can have a substantial adverse impact on the cardiovascular system, similar to active smoking.11 Peak secondhand smoke exposure can also impact lung function decline in asthmatic children.12 Regulatory measures banning smoking in motor vehicles, however, have only been passed in a small number of countries, states and municipalities, and are limited to the protection of children of varying ages.6 13
This pilot study measured air nicotine concentrations in motor vehicles of smokers and non-smokers while they commute to and from work. The application of the protocol under actual driving conditions rather than experimental conditions, as was done in previous studies,7 8 9 14 may better reflect actual exposure concentrations during driving. Given available evidence on the lack of protection of ventilation measures in indoor places,1 15 we hypothesised that ventilation measures in the vehicle, such as having windows down or air conditioning on, may be ineffective in providing complete protection from exposure to secondhand smoke to non-smoking passengers.
Methods
Design and population
This exposure survey used air nicotine passive samplers to characterise passenger exposure to secondhand smoke in motor vehicles. During the summer of 2008, employees of a large medical institution in Baltimore, Maryland, who congregated outdoors around their workplace were invited to participate. To be eligible, the employee had to regularly operate a vehicle and have a daily commute that lasted 30 minutes or more. Smokers also had to regularly smoke within the vehicle. In total, 29 drivers were recruited, 24 smokers and five non-smokers. Each driver received two air nicotine samplers. A total of 17 smokers (71%) and five non-smokers (100%) returned the nicotine samplers, leaving 44 air nicotine samplers in the present study. Reasons for not returning the samplers after initial recruitment included health problems (n = 2), lost samplers (n = 1) and unknown reasons (n = 4). Smokers initially recruited and smokers returning samplers were similar for all participant and vehicle characteristics evaluated at recruitment (table 1). Participation in the study was voluntary. Written and oral consent was obtained from all participants. The study protocol and consent forms were approved by the Johns Hopkins Bloomberg School of Public Health institutional review board.
Summary of participant characteristics
Nicotine monitoring
Air nicotine concentrations in each vehicle were estimated by passive sampling of vapour-phase nicotine using a sampler originally developed by Hammond and Leaderer.16 The samplers were assembled from a 37-mm sampling cassette containing a filter treated with sodium bisulfate and covered by a polycarbonate diffusion membrane at the Secondhand Smoke Exposure Assessment Laboratory of the Johns Hopkins Institute for Global Tobacco Control.
Two nicotine samplers were placed in each vehicle for a 24-hour period in a sealed container. To evaluate levels of secondhand smoke exposure expected for actual passengers, one sampler was placed at the base of the front passenger seat headrest and the other was placed on the lateral hanger in the back seat behind the driver. Drivers were instructed to open the samplers during travelling time within the 24-hour sampling period and to keep them closed otherwise. All participants received and were instructed to use latex gloves when handling the air samplers. At the end of the sampling period, the collected nicotine was extracted from the filters and analysed by gas chromatography using a nitrogen phosphorous detector.
The time-weighted concentration of airborne nicotine was calculated by dividing the amount of nicotine collected by the filter (μg) per volume of air sampled (m3). Volume sampled was calculated by multiplying the time sampled (provided by the participant) by the effective sampling rate of the sampler (25 ml/min).16 We assumed that the sampling rate was not affected by changes in face velocity caused by open windows. Blanks were used to determine the blank-corrected nicotine concentrations and to calculate the nicotine limit of detection (0.0026 μg/ml corresponding to 0.22 μg/m3 for 1 hour of sampling time). For samples below the limit of detection a value half the limit of detection was assigned.
Data collection
At recruitment, participants were asked to respond to a short questionnaire requesting information on age, sex, education, smoking behaviour and vehicle characteristics (vehicle make, model, year and length of ownership) and occupancy (adult, children and smoking passengers). The vehicle types represented included compact and midsize cars as well as minivans and sport utility vehicles (SUVs). For analysis, the vehicles were grouped into size categories of compact/small and midsize/large vehicles. At the end of the sampling period, each driver was requested to report information on time spent in the vehicle, ventilation use, number of cigarettes smoked and vehicle occupancy for any trips occurring during the 24-hour study. Drivers were also asked about knowledge and attitudes regarding the health risks of secondhand smoke, secondhand smoke regulations and the potential impact of motor vehicle smoking bans on their ability to quit smoking.
Statistical analyses
Descriptive analyses were stratified by participant smoking status. Air nicotine concentrations from samplers placed on the front passenger seat headrest (geometric mean 3.9, 95% confidence interval (CI) 1.5 to 10.1) and back seat behind the driver (geometric mean 2.8, 95% CI 1.1 to 7.3) were comparable (p = 0.12) and concentrations are presented as the average of the two air nicotine samplers in each vehicle. Air nicotine concentrations were described using the median and interquartile range (IQR) overall and by participant and motor vehicle characteristics. To compare nicotine concentrations by number of cigarettes smoked within the vehicle, vehicle size and other travelling conditions, we computed crude and multivariable adjusted ratios of the geometric mean of nicotine concentrations and its 95% CI using linear regression models on log-transformed nicotine. The crude and adjusted ratios (95% confidence interval) of geometric means by motor vehicle characteristics were estimated by exponentiating the coefficients and standard errors from the linear regression models on log-transformed nicotine. Analyses were conducted using Stata version 9.0.
Results
Participant and motor vehicle characteristics
Mean age of study participants who returned the nicotine air samplers (n = 22) was 37 (SD 12) years, 50% were men and 71% had college education or more, with little differences by smoking status (table 1). On average, smoking participants drove 7 (SD 1) days a week and 2 (SD 1) hours/day compared to 5 (SD 2) days a week and 1 (SD 1) hour/day for non-smoking drivers. Smoking drivers smoked in their vehicle on a daily basis and all smoked filtered cigarettes. The number of cigarettes smoked during the sampling period (mean 4.65, SD 2.34) was similar to the average number reported as being smoked daily in the vehicle (mean 5.09, SD 2.75). The size of the vehicle was compact/small for 35% and 60% of smoking and non-smoking drivers, respectively. In 45% of motor vehicles there was at least one passenger in addition to the driver and in 31% there was at least one child passenger, with no major differences by smoking status. None of the non-smoking drivers permitted smoking in the vehicle. All smoking drivers allowed smoking within the vehicle, although 71% of them allowed it only without passengers and with use of ventilation.
Air nicotine concentrations
The median (IQR) sampling time during the 24-hour period was 105 (80–135) minutes. Thirteen samplers had air nicotine concentrations below the limit of detection, including 10 samplers from five non-smokers and three samplers from two smokers. The smoking driver with both front and rear samplers below the limit of detection reported smoking a total of three cigarettes and having the windows down more than halfway during the overall 40-minute sampling time (the shortest commute of all of the drivers in the study). For the other smoking driver, only the rear sampler was below the limit of detection although the nicotine concentration in the front sampler was also relatively low (3.2 μg/m3). The vehicle was a large SUV with ventilation on and a total of five cigarettes were smoked during 110 minutes of sampling time.
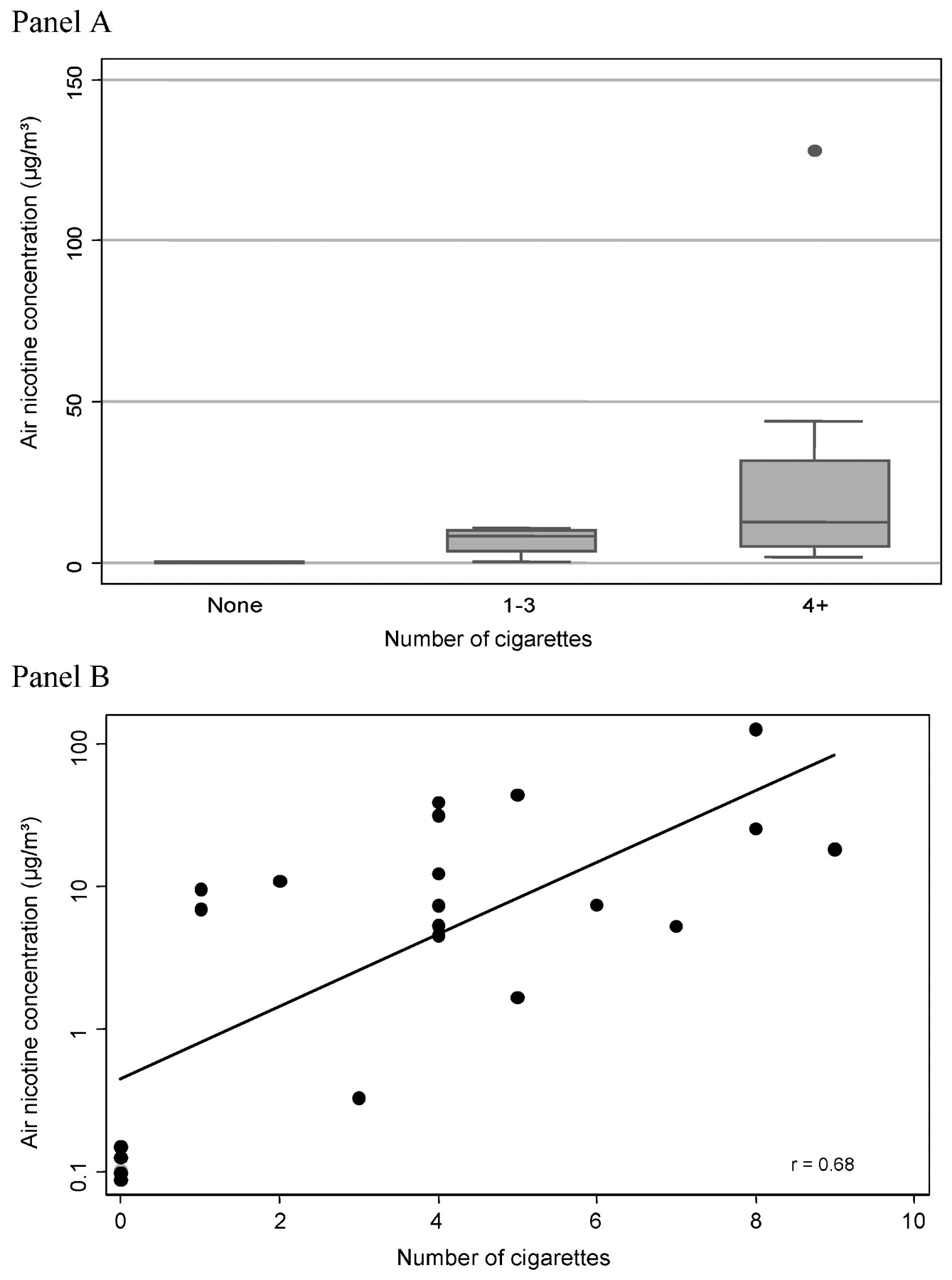
Median (IQR) air nicotine concentrations in smokers’ vehicles were 9.6 μg/m3 (5.3–25.5) compared to undetectable in non-smokers’ vehicles during the sampling period (table 2). The maximum nicotine concentration, 128.1 μg/m3, occurred in a small vehicle with a total of eight cigarettes smoked during the 105-minute sampling period. The driver reported having the windows closed and used air conditioning throughout the sampling period. Air nicotine concentrations increased with increasing number of cigarettes smoked during the sampling period (median air nicotine 8.3 μg/m3 and 12.5 μg/m3 for one to three cigarettes and four or more cigarettes smoked, respectively) (fig 1). Air nicotine concentrations were 1.96 times higher (95% CI 1.43 to 2.67) per cigarette smoked after adjustment for vehicle size, window opening, air conditioning and length of sampling time with small differences before adjustment (ratio 1.79; 95% CI 1.41 to 2.27) (table 2).

{kind=link}
Air nicotine concentrations* (μg/m3) in motor vehicles by number of cigarettes smoked. *Average of front and rear air nicotine concentrations. (A) Box plots where horizontal lines within boxes represent medians; boxes, interquartile ranges; bars, values within 1.5 times the interquartile range; solid circles, outlying data points. (B) Scatterplot where the line represents the linear dose-response relation between the number of cigarettes smoked and the log10 nicotine concentrations; r is the Spearman correlation coefficient.
Air nicotine concentrations* (μg/m3) by vehicle and travelling characteristics
Among smoking drivers, median air nicotine concentrations were higher in compact/small vehicles (median 32.3 μg/m3) compared to midsize/large vehicles (median 7.5 μg/m3) (table 2). After adjustment for number of cigarettes and other driving condition characteristics, air nicotine concentrations in smokers’ vehicles were 4.34-fold time increased in compact/small vehicles compared to midsize/large vehicles, although the confidence intervals were wide (table 2). Median air nicotine concentrations were similar in vehicles that opened windows less and more than halfway for most of the trip. However, after adjustment for the number of cigarettes, car size and other driving conditions, there was a 60% decrease in air nicotine concentrations in the vehicles that reported having their windows opened more than halfway for most of the trip (table 2).
Knowledge and attitudes
All smokers and non-smokers acknowledged that smoking in the motor vehicle poses a health risk to the passengers (table 1). Fifty-three per cent of the smokers reported that being unable to smoke in their cars would help them to quit smoking. Ninety-three per cent of smokers agreed with the statement that motor vehicles should be smoke-free on a voluntarily basis and only 7% of the smokers agreed that motor vehicles should be smoke-free by regulation.
Discussion
In this study, conducted in motor vehicles under actual driving conditions, air nicotine concentrations measured in smokers’ vehicles were strikingly higher than the non-detectable concentrations found in non-smokers’ vehicles. Air nicotine concentrations within the vehicle increased with the number of cigarettes smoked. The size of the vehicle and the use of ventilation were also relevant determinants of air nicotine concentrations, although opening windows more than halfway for most of the trip could not eliminate exposure to secondhand smoke. The location of the sampler (front seat or rear seat) had relatively little impact on nicotine concentrations within the vehicle.
Our findings are consistent with other studies showing high concentrations of particulate matter of less than 2.5 μm in diameter (PM2.5) measured after smoking a cigarette under stationary and moving experimental conditions.7 8 14 17 While ventilation rates markedly changed depending on window opening, vehicle speed and air conditioning, PM2.5 and carbon monoxide concentrations increased rapidly under all experimental conditions. After converting average PM2.5 concentration during the time over which the cigarette was smoked and its decay period to a 24-hour reference time, smoking two cigarettes within the vehicle resulted in PM2.5 concentrations equal to 42 μg/m3, higher than the 24-hour US Environmental Protection Agency’s ambient air quality standard for PM2.5 (35 μg/m3).7 With recirculation on and closed windows, peak PM2.5 concentrations were much higher.7 In another study, PM concentrations after smoking a cigarette were 10-fold higher than PM concentrations emitted from an idling eco-diesel engine.14 Studies conducted during actual driving conditions also measured high PM concentrations in Boston, US6 and Crete, Greece.18
Information on smoking behaviour within cars is also available through questionnaires and observation. A cross-sectional study of smoking in cars in New Zealand found a 4.1% point prevalence of smoking in cars, with higher prevalence in lower compared to higher socioeconomic status areas, and with 23.7% of smoking cars having other occupants exposed to secondhand smoke.19 In Canada, children in grades 5–12 who had been passengers in smoking cars were nearly twice as likely to respond that smoking should not be allowed in cars with children.20 21 Moreover, being exposed to secondhand smoke in vehicles has been associated with an increased risk of current and persistent wheeze10 and higher levels of nicotine-dependent symptoms in children,22 and with increased respiratory symptoms in young adults.23
Secondhand tobacco smoke health risks have led to the introduction and adoption of legislations to protect passengers from exposure to secondhand tobacco smoke within motor vehicles. So far, legislation has focused on protecting children, with differences in the age range considered. In Arkansas, legislation restricts smoking in motor vehicles where children under age 6 are present, corresponding to the age that children are required to be in car seats.13 In Louisiana and Puerto Rico, smoking bans in motor vehicles cover children up to age 13.24 In California, legislation bans smoking in all vehicles with passengers under age 18.25 At least 10 other US states and several countries have introduced or passed legislation to protect motor vehicle passengers from secondhand smoke exposure. Other countries such as New Zealand have invested in media campaigns advocating no smoking in motor vehicles.19 Public support for smoke-free motor vehicles is also increasing, being as high as 96% of respondents in some surveys.26 As more public places are becoming smoke-free, legislations in motor vehicles are less viewed as government intrusion into private matters, especially when children are included. Indeed, ethical analyses have shown that banning smoking in cars while children are present is the most ethically justifiable position, emphasising the concept of non-malfeasance with regard to child passengers.27
While the main goal of banning smoking in motor vehicles is to protect non-smoking passengers from the health effects of secondhand smoke, additional benefits may include helping smokers to quit and reducing motor vehicle accidents. In our study, 53% of the smoking participants reported that banning smoking in motor vehicles could help them quit. Research conducted in Australia found that smokers had an increased risk of being involved in a motor vehicle accident than their non-smoking counterparts, and driving while smoking also increased this risk.15 In Taiwan, smokers had nearly double risk of motor vehicle mortality than non-smokers after adjustment for socioeconomic status and alcohol use were taken into account.28 Banning smoking in cars may thus contribute to reducing car accidents. From an economic perspective, implementing smoking restrictions in cars may also prove beneficial during the sale of a vehicle. A study conducted in San Diego, California, found smoking status within a vehicle to be significantly associated with the vehicle asking price upon resale even when controlling for Kelley Blue Book (KBB) value and make of the car, reflecting changes in preferences for smoke-free environments,29 as well as the residual secondhand smoke that can accumulate within the vehicles for several days after a cigarette is smoked.30
What this paper adds
This study measured secondhand smoke exposure, as determined by air nicotine concentrations, in motor vehicles during actual driving conditions.
Air nicotine concentrations in smokers’ vehicles were strikingly higher than the non-detectable concentrations in non-smokers’ vehicles and increased with the number of cigarettes smoked.
These high levels of secondhand smoke exposure support the need for legislation that bans smoking in motor vehicles when passengers are present.
Strengths of our study include the measurement of nicotine, a specific tracer for tobacco smoke that is commonly used to assess secondhand smoke exposure as a surrogate for other toxic and carcinogenic components in tobacco.11 31 Moreover, while recall bias may have affected the reporting of the number of cigarettes smoked, window opening and air conditioning use, air nicotine is an objective marker of secondhand smoke that is not affected by self-report. Our questionnaire requested information on filtered vs non-filtered cigarettes. Information on the type (that is, light vs regular) and brand of filtered cigarettes, however, was not collected and could not be related to air nicotine concentrations. Because this study aimed to measure secondhand smoke during actual driving conditions, air exchange rates of ventilation patterns within the vehicles were not directly measured. Also, uncertainties in the implementation of study procedures by the driver such as the installation and use of samplers as directed, including opening and closing the samplers, is a potential limitation of this study. While the sample size was small and multivariable models must be interpreted cautiously, we had sufficient statistical power to detect differences in air nicotine concentrations in smoking and non-smoking vehicles and to evaluate exposure levels with increasing number of cigarettes smoked. Finally, various types of vehicles including compact and midsize cars, minivans and SUVs were represented in the study.
While there is no safe level of secondhand smoke exposure, air nicotine concentrations in motor vehicles were generally higher than air nicotine concentrations measured in public32 or private indoor places,33 and even higher than concentrations measured in restaurants and bars that allow smoking.34 Because smoking in cars can contaminate the vehicle surface and environment after active smoking has occurred,30 further research is needed to assess possible exposure during periods following active smoking. For instance, studies comparing air nicotine concentrations during driving periods to air nicotine concentrations during 24-hour periods could be useful. Meanwhile, the high air nicotine concentrations measured in motor vehicles in this study support the urgent need for smoke-free education campaigns and legislative measures banning smoking in motor vehicles when passengers, especially children, are present. This study represents one of the few to quantify nicotine concentrations in cars and, although a pilot study, it has implications for informing larger studies and supporting policies aimed at reducing exposure to secondhand smoke in motor vehicles.
Acknowledgments
The authors thank Dr Jonathan Samet for his comments and suggestions provided to a previous version of this manuscript.
REFERENCES
Footnotes
Funding This project was supported by a Clinical Investigator Award from the Flight Attendant Medical Research Institute (FAMRI).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.